Management of deep split in mandibular premolar
02/10/2023
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
A thorough knowledge of the root canal anatomy and its variation is required for achieving success in root canal therapy, along with diagnosis, treatment planning and clinical expertise. Outcome of endodontic therapy depends on the complete disinfection of the entire root canal system followed by a three-dimensional obturation. One of such variation of the root canal system is seen in mandibular premolars with the presence of more than one or two canals. Various cases that have been reported showed mandibular second premolars with the presence of two or more canals with 40%. Tzanetakis et al reported the incidence of two or more canals in the mandibular second premolar that ranged from1.2 to 34%. The occurrence of three canals in the mandibular second premolars has been reported to be 0.0 to 0.4%.11-15. The aim of this article is to discuss the successful management of endodontic treatment performed on right mandibular second premolar having three canals with three different apical foramina.

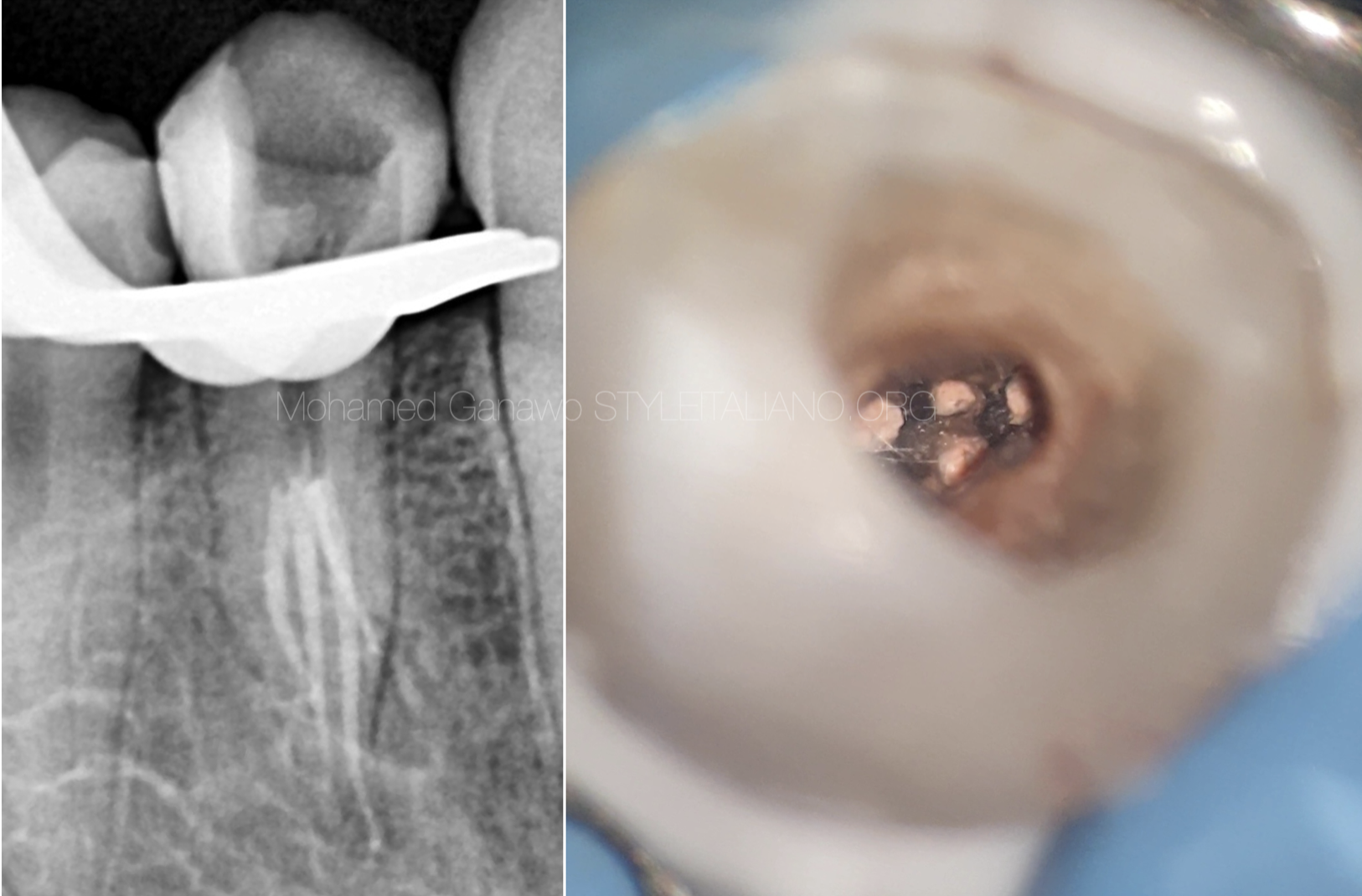
Fig. 1
A 54year female patient was referred to Dr.Doshi’s Dental Clinic and Root Canal Centre by the earlier dentist as after the access opening , the dentist was finding difficulty to treat the case due to the presence of anatomical variation or extra roots in mandibular second pre-molar.
Radiographic diagnosis Fig.1 :-
The simplest, non-invasive clinical method to provide a clue about the canal morphology is a preoperative periapical radiograph and an angulated radiograph from 30° mesial or distal projection.
Radiographic evaluation of tooth no.45 revealed :-
Access cavity preparation was already done by earlier dentist.
The tooth with one canal splitting into three in the middle third region of the root.
Management –
Mandibular premolars exhibits a complex canal anatomy. This makes it difficult to clean and seal the areas which contain infected debris or soft-tissue remnants. Many modified techniques have been proposed to accomplish meticulous cleaning and shaping for a successful root canal treatment.The associated challenges can arise during diagnosis, cleaning and shaping to obturation.
Use of narrow ultrasonic endodontic tips aid to scout and find the extra root or canal orifice below the underlying dentin.
Location and negotiation of canals –
After achievement of endodontic access and removal of tissue from the pulp chamber, modifications in the access design facilitates location and negotiation of the complete root canal system. If the outline morphology is oval, the number of canals can be two or three or more. Endodontic ultrasonic tips plays a crucial role in modification of the access cavity to locate extra canal.
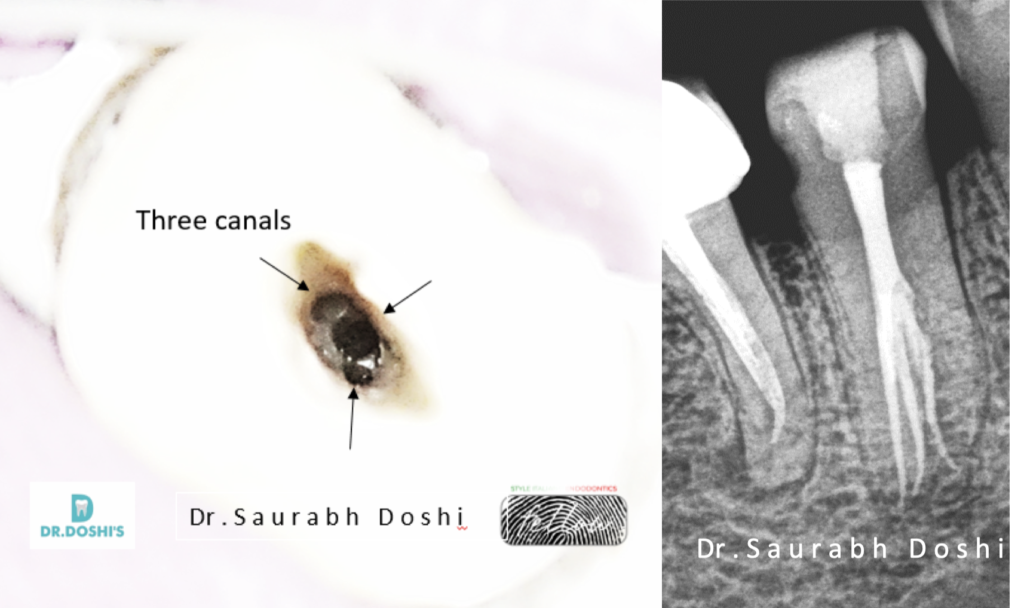
After the refinement of the access cavity under rubber dam isolation, canal splits or trifurcation were negotiated using stainless stell K-file no.8 and K-file no.10

Fig. 2
Cleaning and Shaping -
Glide path preparation was done using stainless steel K-file no 10 and K-file n0.15 to make it smooth and reproducible path from canal orifice to physiologic terminus(apical constriction) until the file becomes super loose in the canal splits.
Working length determination was done using stable coronal reference point using electronic apex locator and the same was confirmed using radiograph.
After working length determination , shaping of the spilt canals was done in the sequence of 20-4% , 25.-4% rotary files to conserve remaining dentin thickness( RDT)
Irrigation protocol –
5.24% sodium hypochlorite was used in between instrumentation using 30 gauge side vented needle.
After shaping, following protocol was used using activation device (Air Sonic activation using eddy polymeric tip.)
17% EDTA – 1 ml per canal – air sonic activation using eddy polymeric tip.
Distilled water to flush the canal.
5.25% sodium hypochlorite -10 ml for three canals- refreshing solution after every 2 ml – air sonic activation.
Distilled water as a final irrigating solution.

Fig. 3
Obturation protocol –
Master Cone Selection was done for all three canals and canals were dried using paper points.
Root canals were obturated one canal at one time, gutta percha was coated with AH plus resin sealer .Gutta percha were seared at each canal orifice , canal by canal three times using touch and head device with slightly bent tip 2% Narrow Anterior heat plugger using Carl Zeiss (Extaro 300) dental operating microscope.
Photo under operating microscope , Downpacking the gutta percha in the root canal in middle third of canal. (Radiograph and clinical image)

Fig. 4
Since the MTA takes around 6-8 hours for complete setting, the patient was called on the next day and the moist gauze was removed and a plugger was used to check the consistency of the MTA and to examine if the material was thoroughly set. Full length of the root canal was obturated with MTA and verified on the periapical radiograph . The patient was advised full coverage prosthesis.
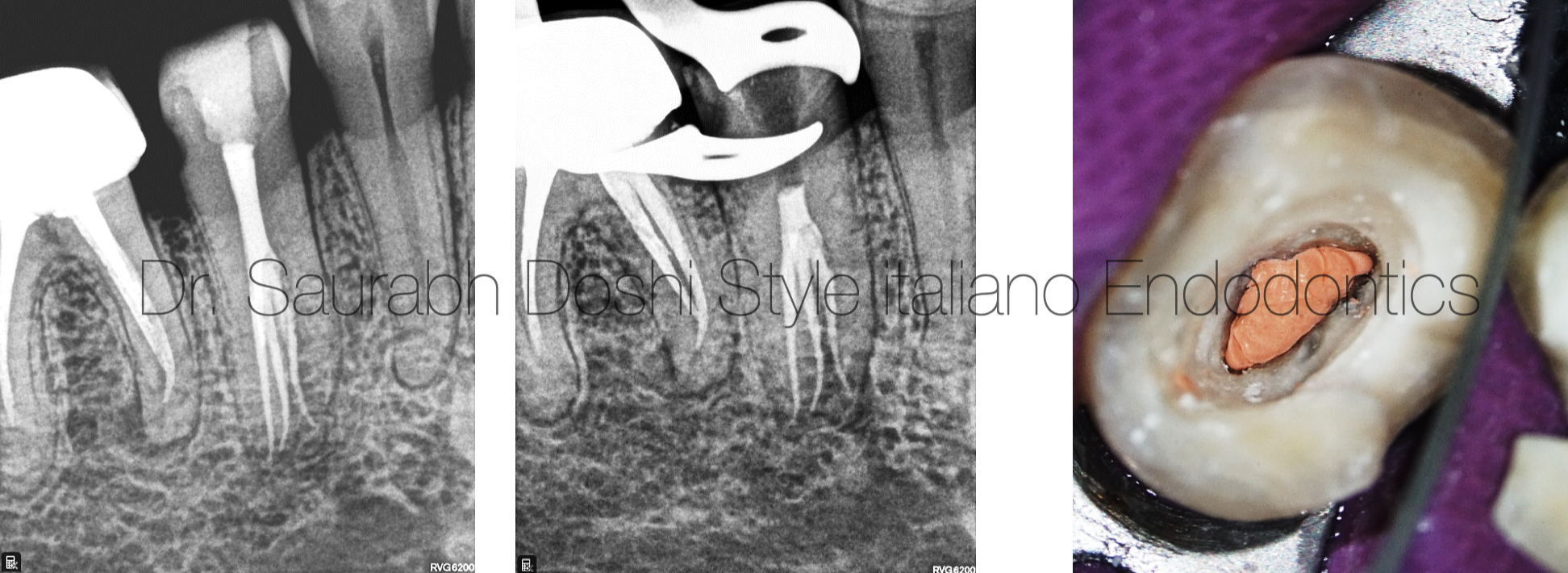
Fig. 5
Subsequently, thermoplasticized obturation (backfill) was performed in increments using backfill gun.
Post endodontic restoration –
The access cavity was then sealed using core build up material to achieve a coronal seal.

Fig. 6
Dr. Saurabh Doshi
2015 : Diploma in Laser Dentistry (Austria)
2017 : Masters with honour in Endodontics from M.A.Rangoonwala Dental College and research centre, Pune, India.
2021 : Diplomate of Indian Board of Endodontics from prestigious Indian Endodontic Society , acclaimed and internationally.
Author of Book “The Root Canal Obturation – Past , Present and Future”
Saurabh Doshi has been a speaker in various Indian Dental Association Forums.
Director : Dr. Doshi’s Dental Clinic and Root Canal Centre, Baramati , India.
Practicing exclusive Micro-Endodontics and Restorative Dentistry.
A passionate clinician , avid sportsman and a doting father.
Conclusions
Complexities in the internal anatomy of mandibular premolars are well documented in the literature.Mandibular premolars with their root canal systems are considered the most difficult teeth to treat endodontically due to their wide variation of internal and external root morphology and also that the division of the roots and/or root canals in these teeth usually occurs in the middle and apical thirds which makes detection of these anatomical variations difficult.
Considering the number of root canal, apical deltas, and lateral canals, they are supposed to be the most difficult teeth to manage.Reports with the existence of 3, 4, or even 5 root canals for mandibular premolars have been documented, which suggests a possibility of missing an extra root or canal.
Proper diagnostic imaging along with an adequate knowledge of the root canal anatomy and its possible variations is necessary for successful endodontic treatment. Proper interpretation of periapical radiographs taken in more than one angle is mandatory to detect any morphological variations of teeth.
The periodontal ligament space may show a sudden narrowing of the root canal space on its division into two or more canals Dentin map analysis on the floor of the pulp chamber also helps in the location of all the root canals.
Use of magnification and illumination, especially use of operating microscopes in bi-furcation or tri-furcation split cases plays a crucial role in its endodontic treatment more conservatively due to enhanced visibilty.
Access preparation was modified with ultrasonics for thorough visualization of the root canal as well as ease of placement of initial apical file and shaping and cleaning of the apical third of the root canal system. Many authors have reported one orifice in the lingual side and two in the buccal for mandibular premolars with three canals.
Determination of working lengths of each root with electronic apex locator and also relating them them to radiographs reduces the chances of flare-ups. A through cleaning and shaping of all three canals till working length , irrigation and its activation of irrigant and three dimentional obturation using thermoplasticized obturation technique followed by adequate coronal restoration, plays a vital role in prognosis of endodontically treated tooth.
The anatomy of the mandibular premolar has complex variations . Adequate knowledge of root canal anatomy and its variations, careful interpretation of periapical radiographs and CBCT, modification of access cavity, proper inspection of pulpal floor, and a detailed examination of the internal morphology of tooth under magnification and illumination are important prerequisites for a successful endodontic treatment.
Bibliography
Rossman LE, Hasselgren G, Wolcott JF. Oral facial dental pain and emergencies: endodontic diagnosis and management. Cohen S, Hargreaves KM, editors. Pathways of pulp. 9th ed. St. Louis (MO): Mosby; 2006
Cleghorn BM, Christie WH, Dong CC The root and root canal morphology of the human mandibular second premolar: a literature review. J Endod 2007 May;33(5):1031-1037.
Vertucci FJ. Root canal morphology of mandibular premolars. J Am Dent Assoc 1978 Jul;97(1):47-50.