Management of complicated crown fracture of newly erupted maxillary central incisor. Conservative approach with 3 years follow up
13/07/2024
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Coronal fracture by trauma is the most frequent type of dental injury in the permanent dentition. The majority of dental injuries involves the anterior teeth, especially the maxillary incisors due to their anterior position and protrusion caused by the eruptive process. Several factors influence the management of coronal tooth fractures, including extent of fracture, pattern of fracture and restorability of fractured tooth (associated root fracture), secondary trauma injuries (soft tissue status), presence/absence of fractured tooth fragment and its condition for use, occlusion, esthetics, and prognosis. One of the options for managing coronal tooth fractures, is the reattachment of the dental fragment when it is available. Reattachment of a fragment to the fractured tooth can provide good and long-lasting esthetics (because the tooth’s original anatomic form, color, and surface texture are maintained). Coronal fractures of permanent teeth with pulp exposure present both endodontic and restorative challenges. For young patients in whom the exposed pulp maintains its vitality, pulpotomy is the best endodontic treatment option. A partial pulpotomy, known as the Cvek technique is indicated for teeth having the following characteristics : traumatic pulp exposure with open apex or thin dentinal walls. This technique involves amputation of the dental pulp 2 mm apical to the affected pulp tissue.
There are several reattachment techniques such as:
- Bonded technique: Re-attachment of the fragment with no additional preparation.
- Chamfer technique: Re-attachment of the fragment after 1.0 mm-depth chamfer was placed in the fracture line in the buccal surface.
- Over-contour technique: Re-attachment of the fragment after superficial preparation on the enamel extending 2.5 mm coronally and apically from the fracture line with a depth of 0.3 mm.
- Internal groove technique: Internal dentinal groove and re-attachment of the fragment.
Reis and colleagues have shown that:
A simple reattachment with no further preparation of the fragment or tooth was able to restore only 37.1% of the intact tooth’s fracture resistance,
whereas a buccal chamfer recovered 60.6% of that fracture resistance;
Bonding with an over contour and placement of an internal groove nearly restored the intact tooth fracture strength, recovering 97.2 and 90.5% of it, respectively.

Fig. 1
7 years old girl presented to my dental clinic with crown fracture of the right maxillary central incisor.
She presented to the clinic 4 h after the trauma.
Clinical examination revealed complicated crown fracture of the right maxillary central incisor with pulpal exposure of approximately 1 mm. There was no sign of trauma to the adjacent primary teeth, which were vital and not mobile.

Fig. 2
Periapical radiographic examination showed incomplete root development, open apex, thin dentin wall, no periapical pathology, and absence of root or alveolar bone fractures

Fig. 3
The intact tooth fragment was brought to the clinic by her mother.
The possibility of reattaching the same tooth fragment was explained to the patient’s mother.
Endodontic management included partial
pulpotomy. The treatment plan was accepted.
To avoid dehydration during clinical and radiographic evaluation and endodontic therapy, the tooth fragment was immersed in saline solution.

Fig. 4
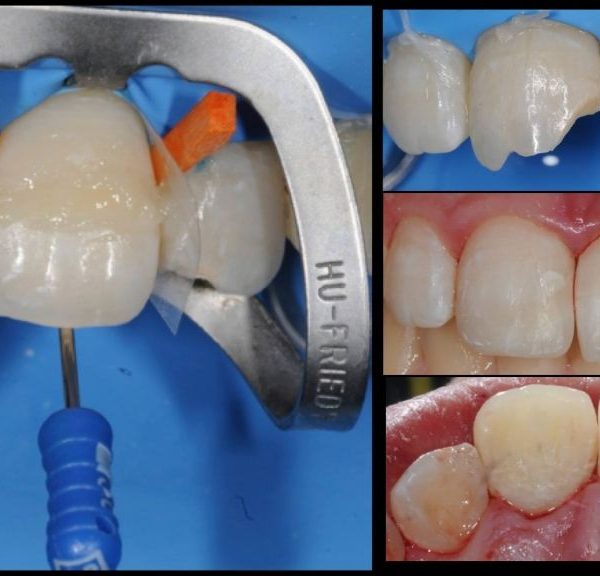
A local anesthetic was administered and the affected tooth was isolated with a rubber dam.
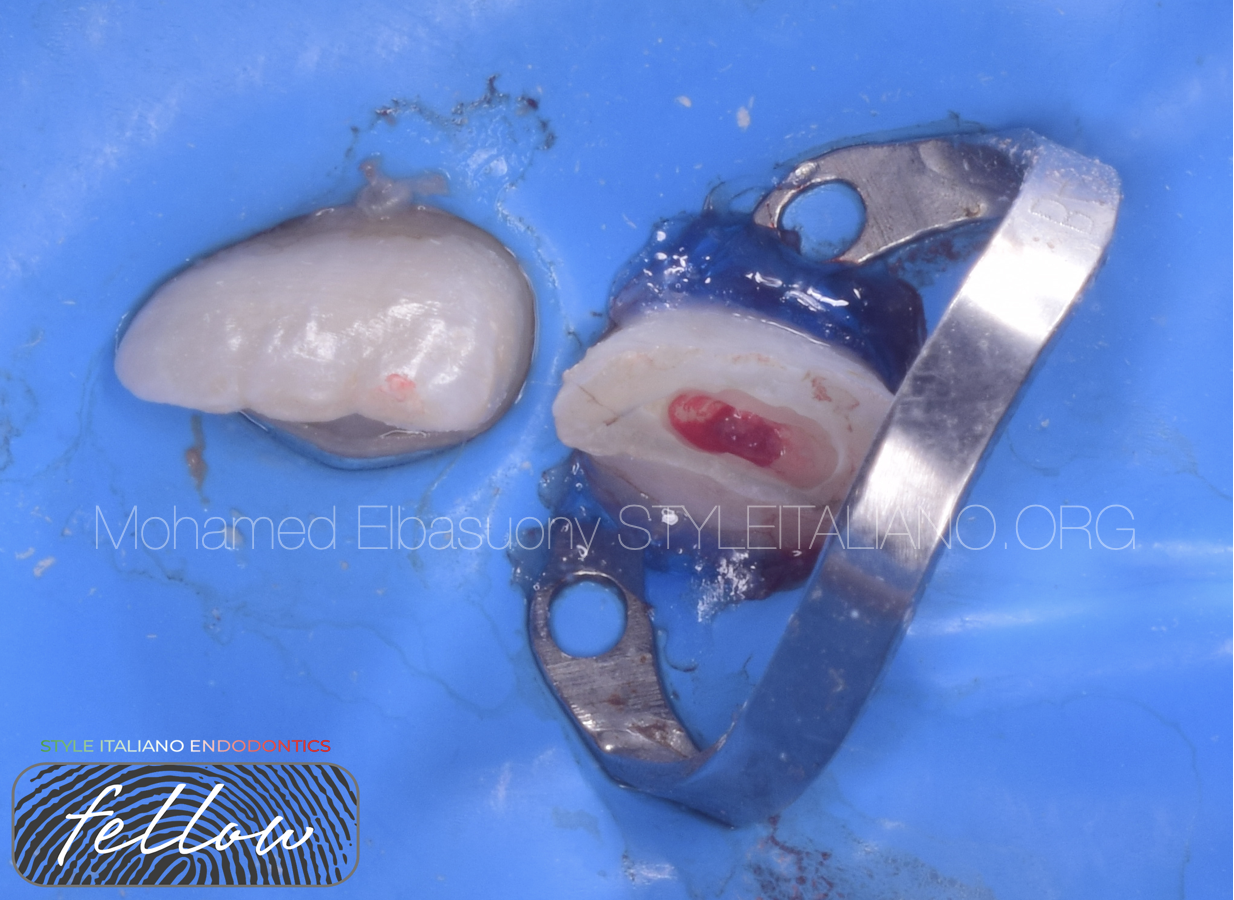
Fig. 5
Round bur (with continuous saline rinsing) was used to amputate the pulp close to the exposure site to a depth of 2 mm.

Fig. 6
Bleeding control and MTA application.
Bevel preparation on the enamel surface of the fragment and tooth structure was performed using taper stone.
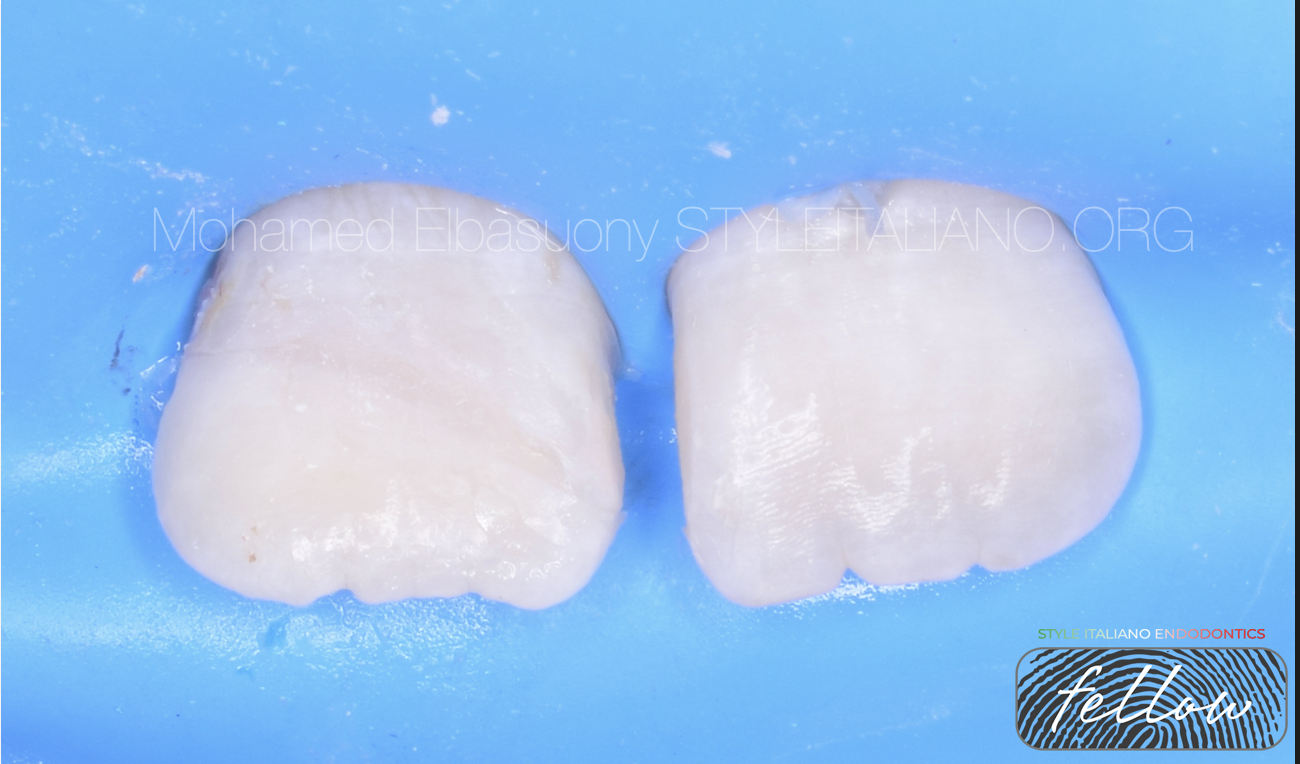
Fig. 7
Both the fragment and the remaining dental structure were acid etched using 37% phosphoric acid for 30 s for the enamel and 15 for the dentin; the acid was eliminated by rinsing with distilled water and drying.
Dental adhesive was applied to both the fragment and the tooth and light cured for 40 s
Composite resin was used to adhere the fragment to the tooth.

Fig. 8
Periapical radiograph after reattachment.

Fig. 9
Before and after photo

Fig. 10
6 months follow up

Fig. 11
12 months follow up

Fig. 12
18 months follow up
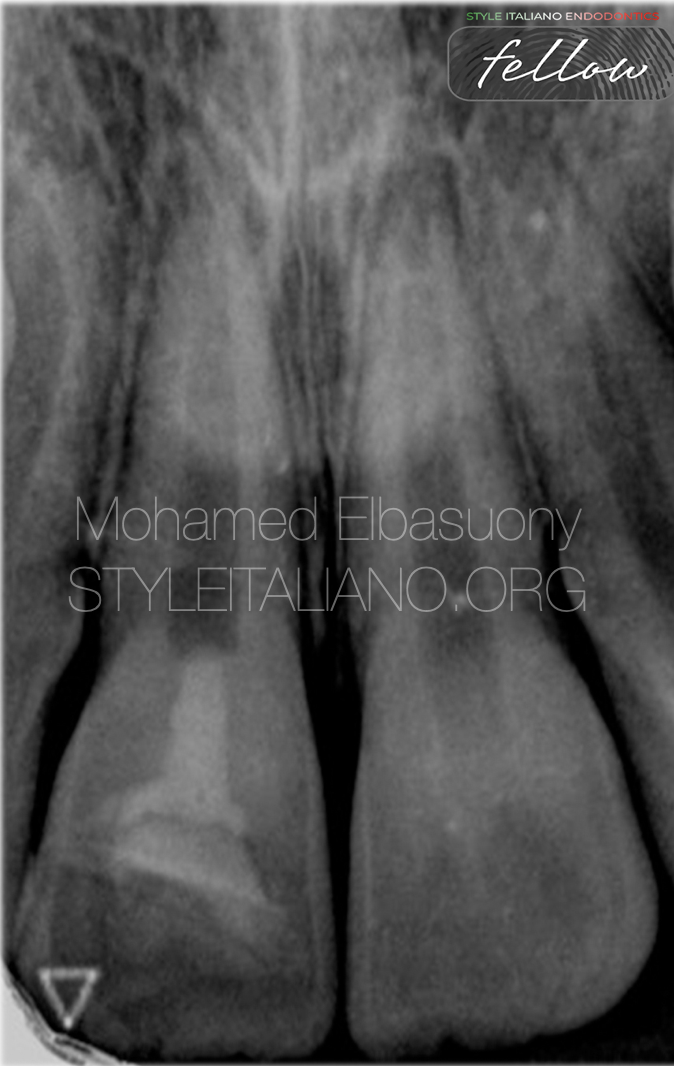
Fig. 13
24 months follow up

Fig. 14
30 months follow up
Appearance of dentine bridge
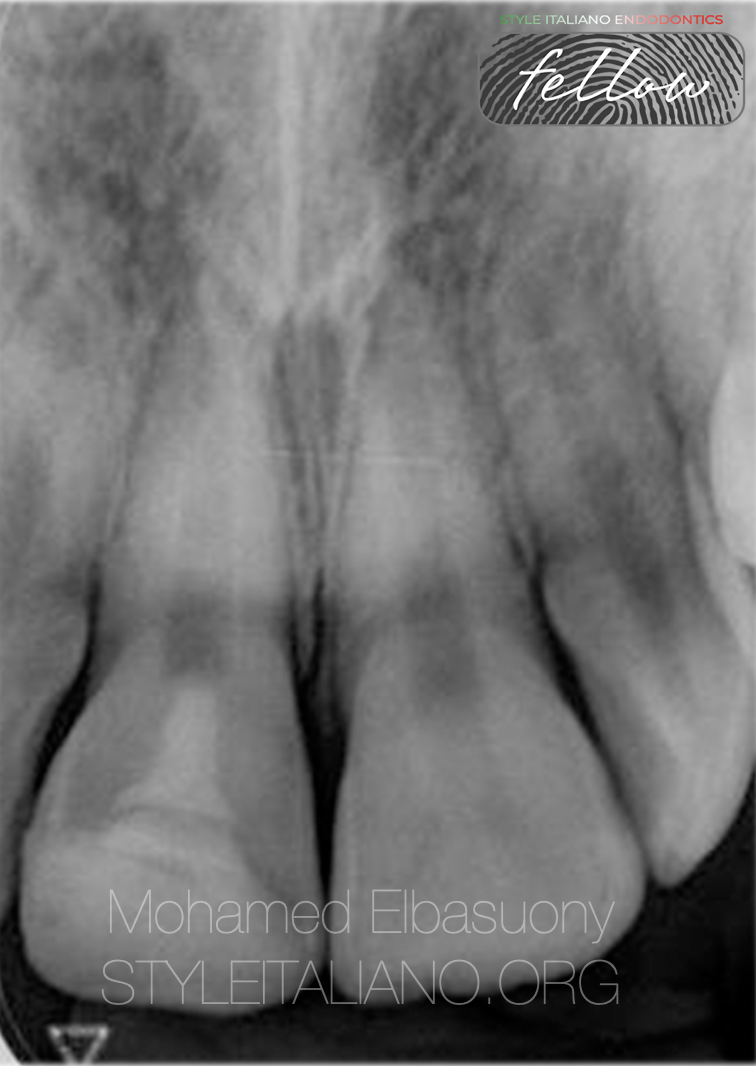
Fig. 15
After 36 month follow up, the patient came with secondary trauma, but in this time the fragment was missed.
Composite restoration was used to restore the missing part of the tooth structure.

Fig. 16
About the author:
Mohamed Elbasuony
BDS from faculty of dentistry, Mansoura university in 2013.
Diploma in Endodontics at faculty of dentistry, Mansoura university in 2018.
Enrolled in the MSc in Endodontics at faculty of dentistry, Mansoura university in 2020.
StyleItaliano Endodontics Fellow
Endodontic Specialist.
Conclusions
The best restorative option for treating fractured anterior teeth is reattachment of the tooth fragment because the tooth’s original anatomic form, contour,
surface texture, color, occlusal alignment, translucence, and function are maintained.
Although the reattachment of fractured tooth fragments is not a final treatment, it offers an excellent restorative option for clinicians and patients because it restores tooth function and aesthetics, requires less time in the dental office, and represents a cost-effective approach.
Bibliography
Andreasen JO, Andreasen F, Andersson L. Textbook and color atlas of traumatic injuries to the teeth. 3rd ed. St Louis (MO): Mosby; 1994.
Reis A, Francci C, Loguercio AD, et al. Re-attachment of anterior fractured teeth: fracture strength using different techniques. Oper Dent 2001;26(3):287–94.
Reis A, Loguercio AD, Kraul A, Matson E. Reattachment of fractured teeth: a review of literature regarding techniques and materials. Oper Dent 2004;29(2):226–33.