

Management of a Type III Radix Entomolaris in a first lower molar
10/07/2023
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Understanding the anatomical variations of the root canal system is a must to achieve the main goals of our treatment.
The radix entomolaris is the most common variation in mandibular molars.
With the help of CBCT we can measure and see the original shape of the additional root, thus creating a predictable strategy for cleaning, shaping, and filling the root canal system.
In this case we are treating a previously initiated Radix Entomolaris in a young patient with limited mouth opening, calcification of the coronal third, and long roots.
The main objective of root canal treatment is to prevent or eliminate apical periodontitis, and in order to achieve this, we must know the different anatomical variations of the teeth.
One of the most common variations in mandibular molars is the existence of a supernumerary third root, which can be found often distolingually, it is known as Radix Entomolaris and it was described for the first time by Carabelli in 1844.
In African, European, and Asian demographics, the frequency ranges from 3% to 5%, while in the Mongoloid populations it can reach a frequency of 40%.
There are three types of Radix Entomolaris described in the literature, based on the Ribeiro & Consolaro classification, with Type III being the most difficult to treat, presenting curvature in the coronal third, and buccal curvature from the middle third or apical third of the root.
Knowing that missed canals are one of the main causes of endodontic failure, we must be aware of this type of anatomical variation, despite it not being particularly frequent.

Fig. 1
A young 13-year-old patient comes to the office with severe pain that radiates to his ear and prevents him from chewing.
His dentist performed an unsuccessful endodontic treatment because of the coronal third calcification.
In the preoperative X-ray we can observe long roots, coronal calcification, and suspect an additional distal root.
Considering the fact that the tooth had already been previously treated, removing a large amount of coronal tissue, and putting the anatomical complexity into account, we decided to take a CBCT to come up with the most conservative strategy.
The diagnosis was previously initiated therapy with symptomatic apical periodontitis.

Fig. 2
Image of the sagittal plane of the CBCT where we can see the long distal root and the apical curvature of the messial canals.

Fig. 3
Image of the axial plane of the CBCT showing the independent distolingual canal.

Fig. 4
Image of the coronal plane of the CBCT showing the Type III Radix Entomolaris
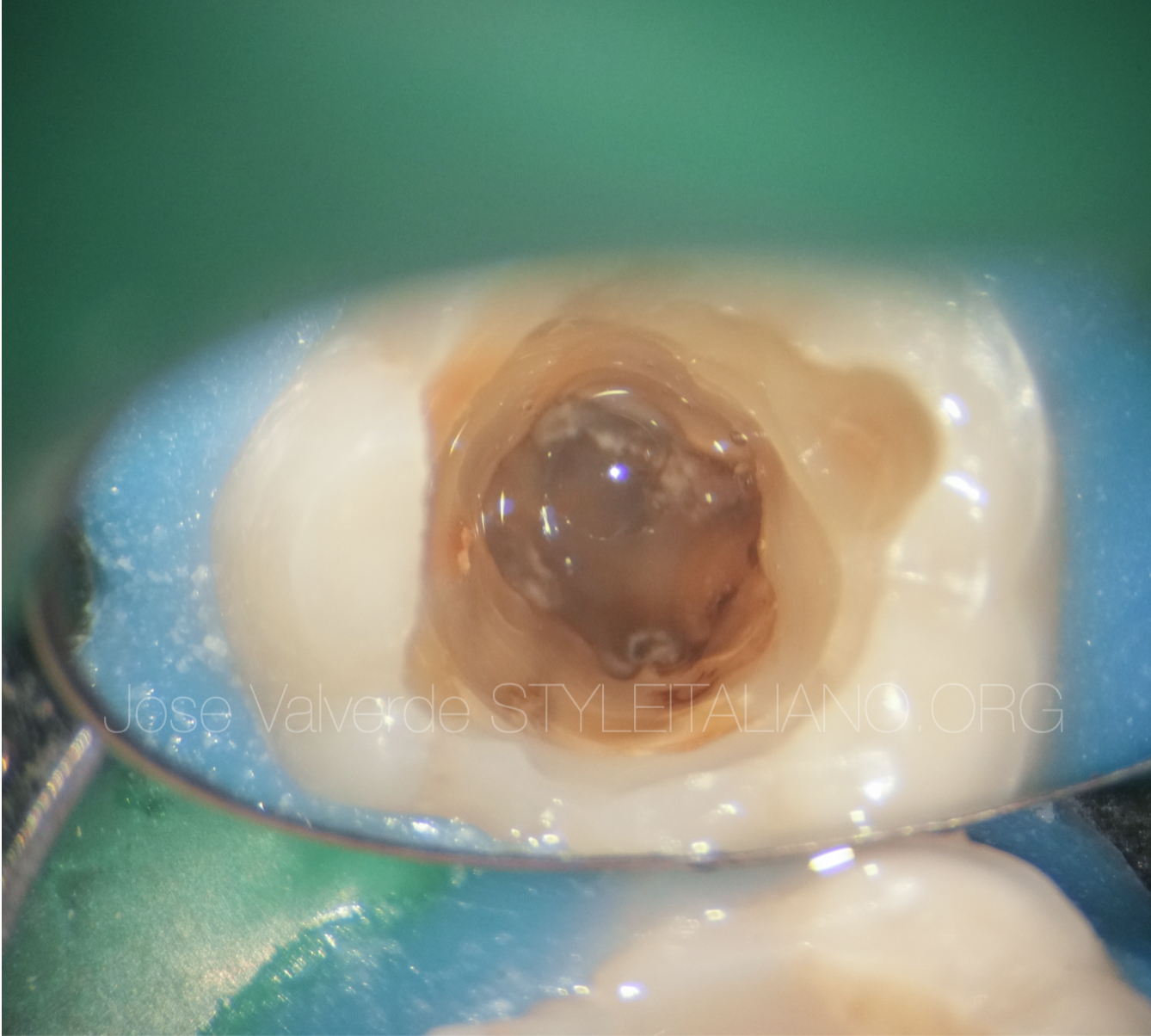
Fig. 5
Previous operator tried to find the canals with no success.
Without magnification and without the correct knowledge of anatomy, a large amount of dentin was removed.
In cases like that, it is crucial to see the different colors of the pulp chamber, and carefully remove only the necessary dentine.

Fig. 6
It is very important to use ultrasonics or long neck burs.
In this case, an EndoTracer 004 (Komet) was used to remove dentin following the minimally invasive way, exposing the distolingual canal.

Fig. 7
In cases of coronal curvature, it is essential to start with small manual files without applying apical pressure.
We fill the chamber with EDTA gel to facilitate manual instrumentation with K-files 06, 08 and 10 (Dentsply).
We advance through the canal pre-curving the tip of the file, with a clockwise-counterclockwise movement.
When we notice resistance at the tip of the file, we should not apply apical pressure. We go back cutting at the exit, making a pull movement.
We must repeat this process with K- files 06, 08 until reaching the working length.
Finally, we will proceed to shape the canal with a size 10 K-file until reaching a minimal glidepath, that is, that the file is completely loose in the canal.
After minimal glidepath and working length measurement we start shaping the canals with BlueShaper Pro (Zarc4Endo).
In this case we are dealing with long canals, all of them measuring 24mm.
We fill the pulp chamber with 4.25% NaOCl during the entire shaping procedure and we start working each canal in thirds, performing a vertical instrumentation, without apical pressure and without brushing the walls of the canals.
We check with a 10 K-File (Dentsply) that we have not lost patency during shaping.
After each rotary file we clean the canals with NaOCl using an Irriflex tip (ProduitsDentaires) and refill the pulp chamber to renew the irrigant.
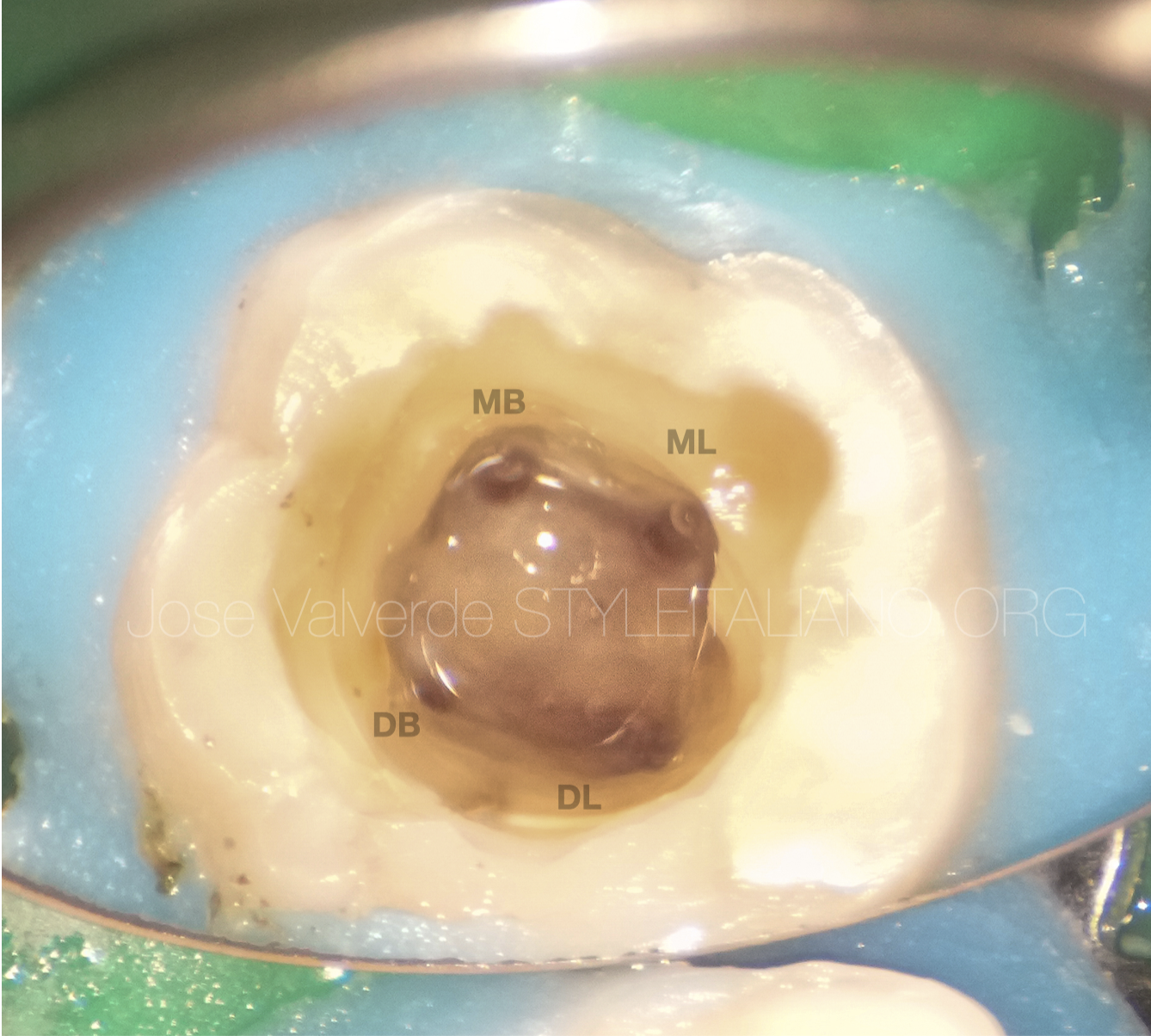
Fig. 8
We finish the three main canals with 25/06, increasing the apical preparation up to 30/03 in the mesials, and 35/03 in the distobuccal.
The distolingual canal was shaped up to 25/04, increasing the apical size up to 30/03 because of the complexity of the coronal and medial curvature.
By enlarging the apical preparation with lower taper files, we were able to improve the mechanical and chemical cleaning of the apical third without compromising the pericervical dentin.
Apical negative pressure with Irriflex (ProduitsDentaires) and 4.25% NaOCl in all canals. We repeat the process with EDTA 17%.
Sonic activation of the irrigants and a final wash with unactivated 4.25% NaOCl.
We use physiological serum to clean the canals before obturation.

Fig. 9
After irrigation, we dry the canals leaving it with moisture to improve the setting of the hydraulic cement.
We fill the middle third of the canal with NeosealerFlo (Avalon Biomed) with gutta-percha 04 (SybronEndo).
Warm vertical compaction was carried out in all of the canals.

Fig. 10
In the orthoradial angulation we can see the coronal curvature in the distolingual canal and how long the canals are.

Fig. 11
Mesializing the X-rays focus we see how a second curvature also appears in the middle third of the distonlingual canal and how the messial canals are independent.
Fig. 12
Distolingual angulation allows us to see the end of the distal canal clearly.
Conclusions
In cases of complex anatomical variations, the use of CBCT is of great help, since it allows us to measure the degree of curvature of the additional root and understand what type of Radix Entomolaris we are dealing with.
Understanding of the different anatomical variations of the teeth that we are going to treat is essential to successfully meet the objectives of our endodontic treatment.
Bibliography
DE MOOR, R. J. G.; DEROOSE, C. A. J. G.; CALBERSON, F. L. G. The radix entomolaris in mandibular first molars: an endodontic challenge. International endodontic journal, 2004, vol. 37, no 11, p. 789-799.
SIQUEIRA JR, Jose F., et al. Causes and management of post-treatment apical periodontitis. British dental journal, 2014, vol. 216, no 6, p 305-312
AAZZOUZI-RAISS, Karim, et al. Effects of conservative access and apical enlargement on shaping and dentin preservation with traditional and modern instruments: A micro-computed tomographic study. Journal of Endodontics, 2023, vol. 49, no 4, p. 430-437.
THOMAS, Anchu Rachel, et al. Comparative evaluation of canal isthmus debridement efficacy of modified EndoVac technique with different irrigation systems. Journal of endodontics, 2014, vol 40, no 10, p. 1676-1680
DRUKTEINIS, Saulius; CAMILLERI, Josette (ed.) Bioceramic materials in clinical endodontics. Berlin/Heidelberg, Germany: Springer, 2021



