Looks like a bullet: An iatrogenic mishap cause by tool misuse
11/10/2020
Ahmed Shawky
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Proper clinical practice in Endodontics requires careful and detailed knowledge on the know how of using different instruments, tools and devices used in the treatment course. Even in the simplest cases, violating the limitation of some instruments or misusing/misplacing those instruments may lead to severe iatrogenic errors which may act as a barrier against providing the proper standard of endodontic care.
The aim of this article is to present a case of previously treated maxillary central incisor with a radiopaque foreign body and symptomatic apical periodontitis.
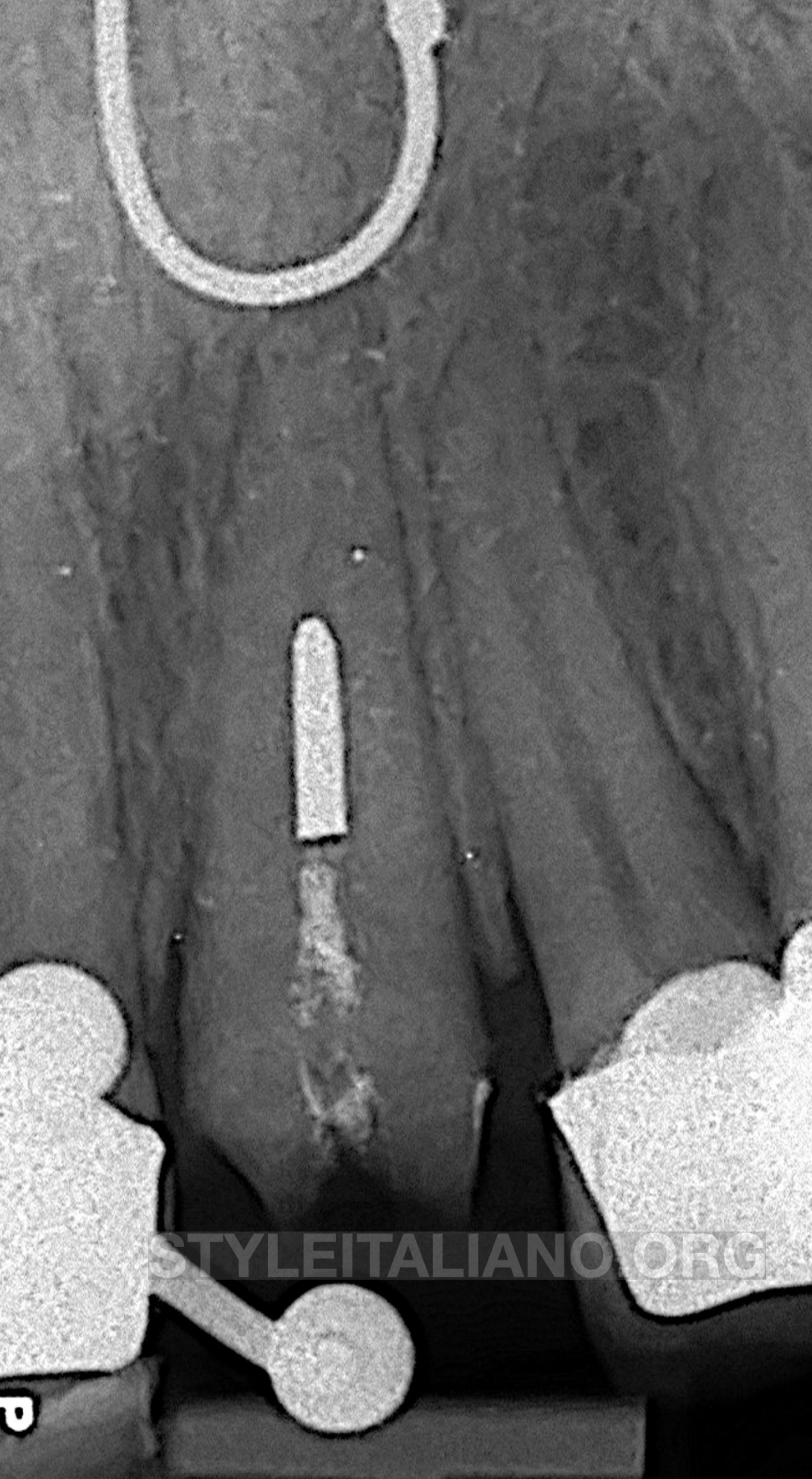
Fig. 1
Pre-operative evaluation
29 years old male presented complaining of dislodged PFM crown from a maxillary central incisor which has been sensitive to biting for couple of weeks before crown loss. Clinical examination revealed a previously treated and prepared maxillary central incisor that is tender to mild percussion. Radiographic examination revealed a radiopaque fragment in the middle portion of the root canal. Apical to the fragment, the canal didn’t seem to be prepared.
A diagnosis of a pulpless, previously treated tooth with apical periodontitis was finally recorded
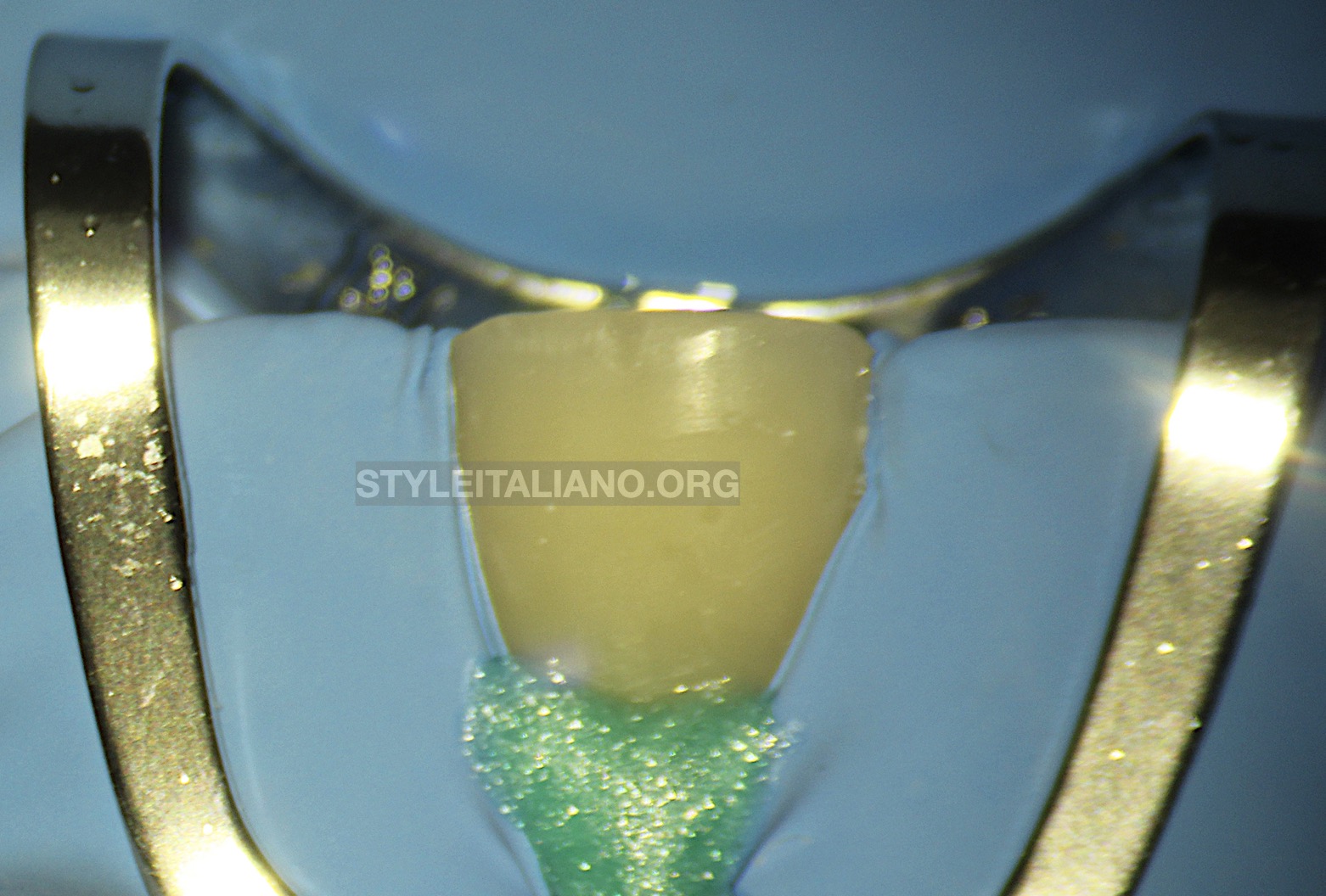
Fig. 2
Pre-endodontic build up and isolation
Due to the crown mutilation and the possibility of mutli-visit treatment, a decision was taken to execute a proper pre-endodontic build up to maintain acceptable esthetics during the treatment period and to aid in the otherwise complicated isolation of the tooth
Primary isolation was done using 212 SA clamp and heavy rubber sheet. Secondary isolation was done using a light curable gingival barrier.
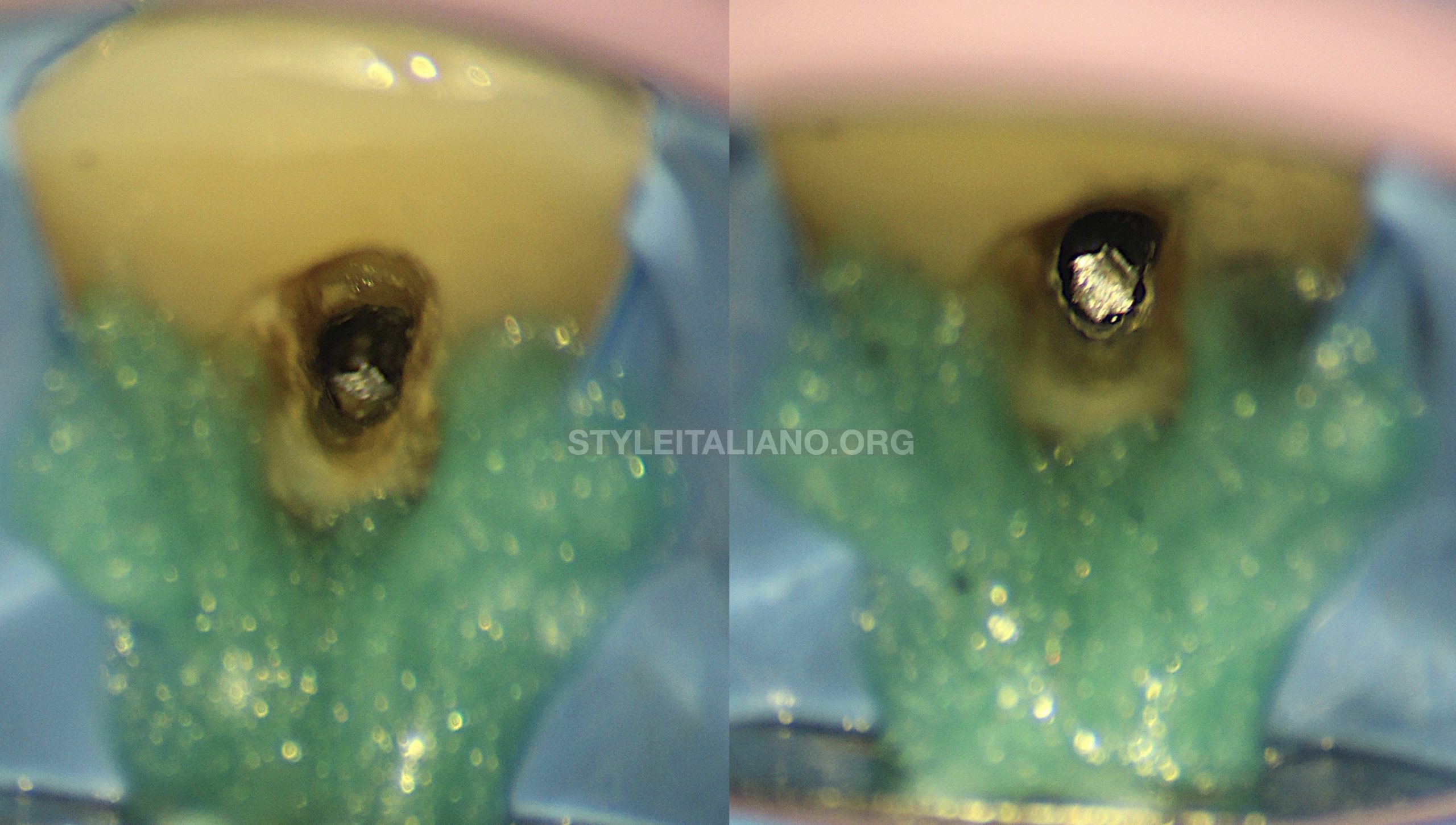
Fig. 3
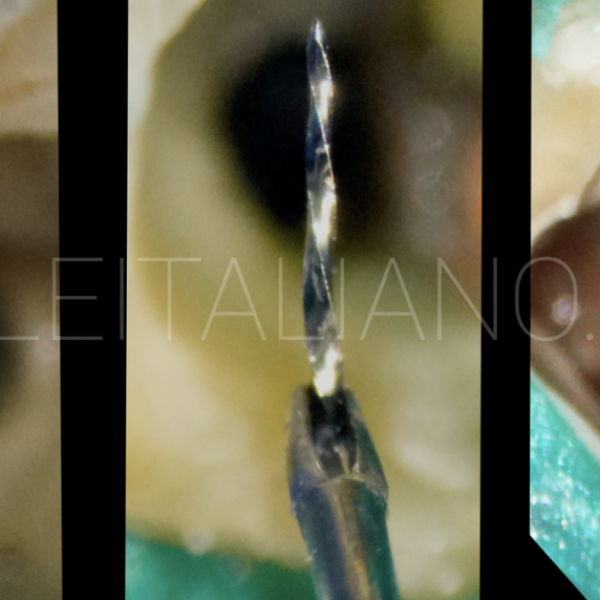
Straight line access to the fragment
Under high microscopic magnification, straight line visual access to the fragment was achieved by removing all overhanging dentin palatally. This was done by refining the previously attempted access using diamond coated ultrasonic tip.
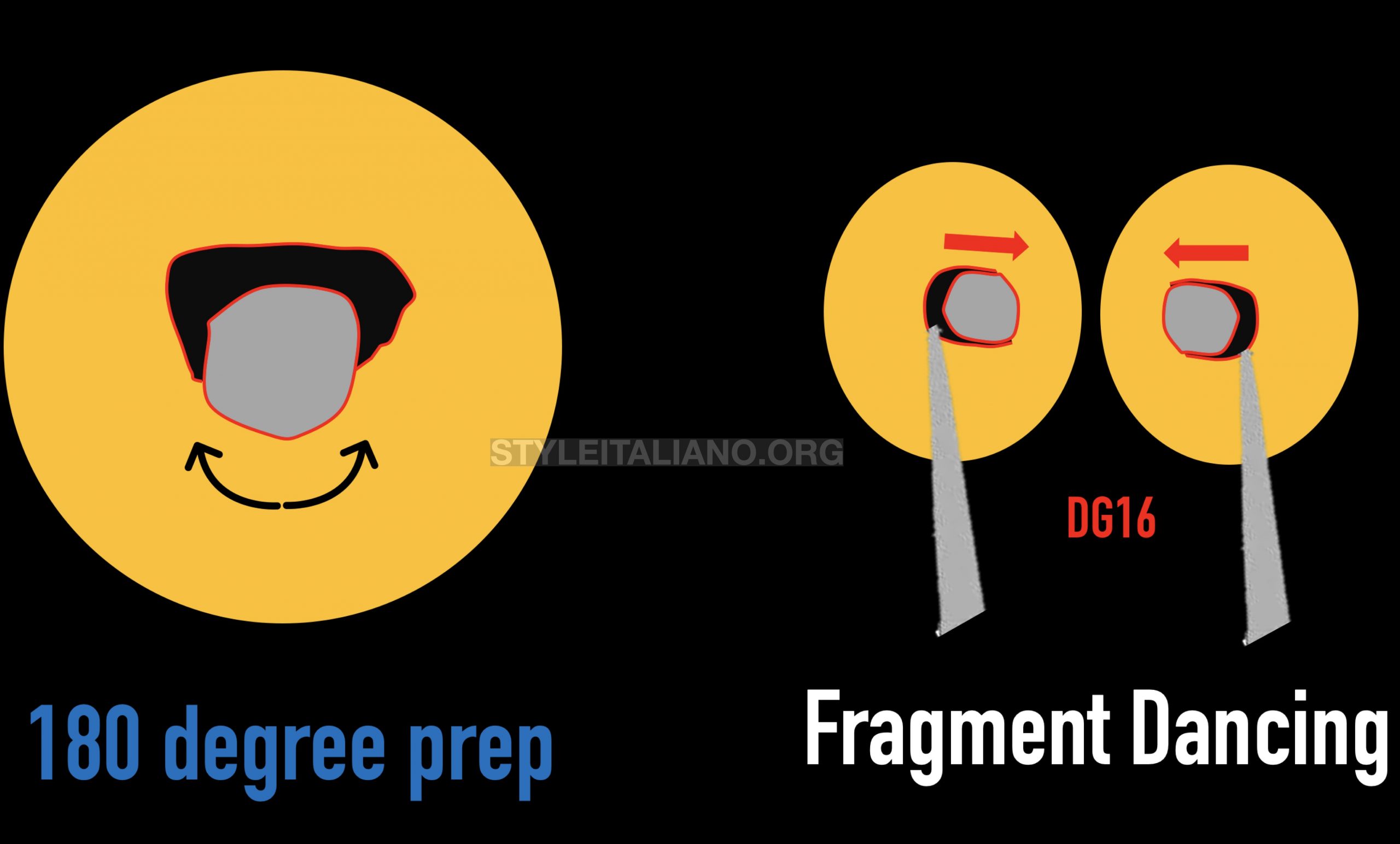
Fig. 4
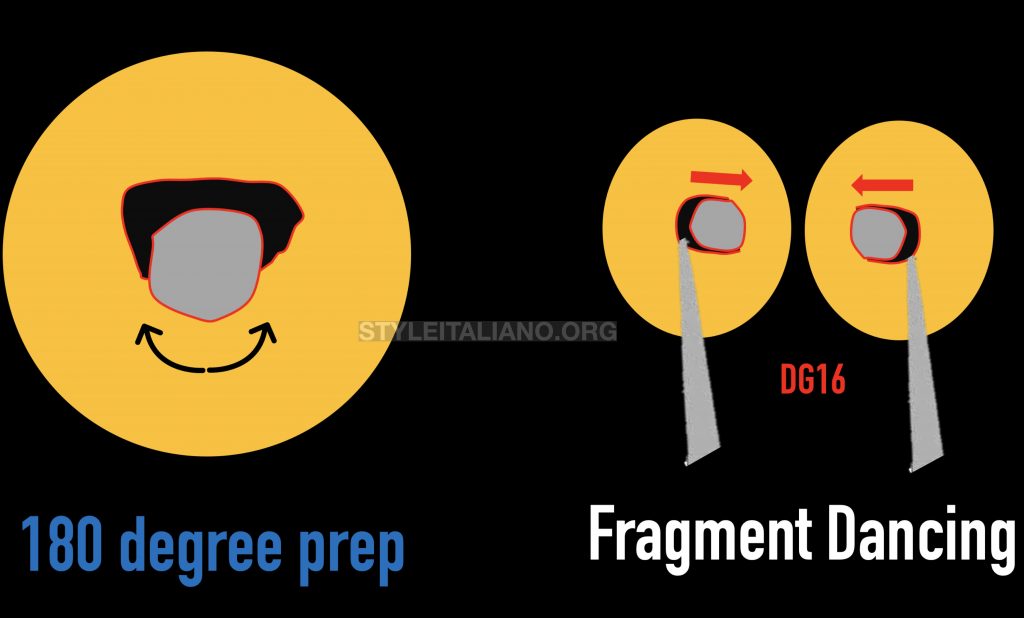
Planning retrieval of the foreign fragment
Due to the cross-section of the coronal part of the root canal in a maxillary central Incisor, it was assumed that fragment is engaging dentin palatally [in the narrow part] while being free in the labial direction [wide part]. This was confirmed by inserting a hand #20 k-file bypassing labial to the fragment.
The plan was to prepare a 180 degrees preparation to a depth of 1-2 mm lingual to the fragment until visual confirmation of looseness is evident
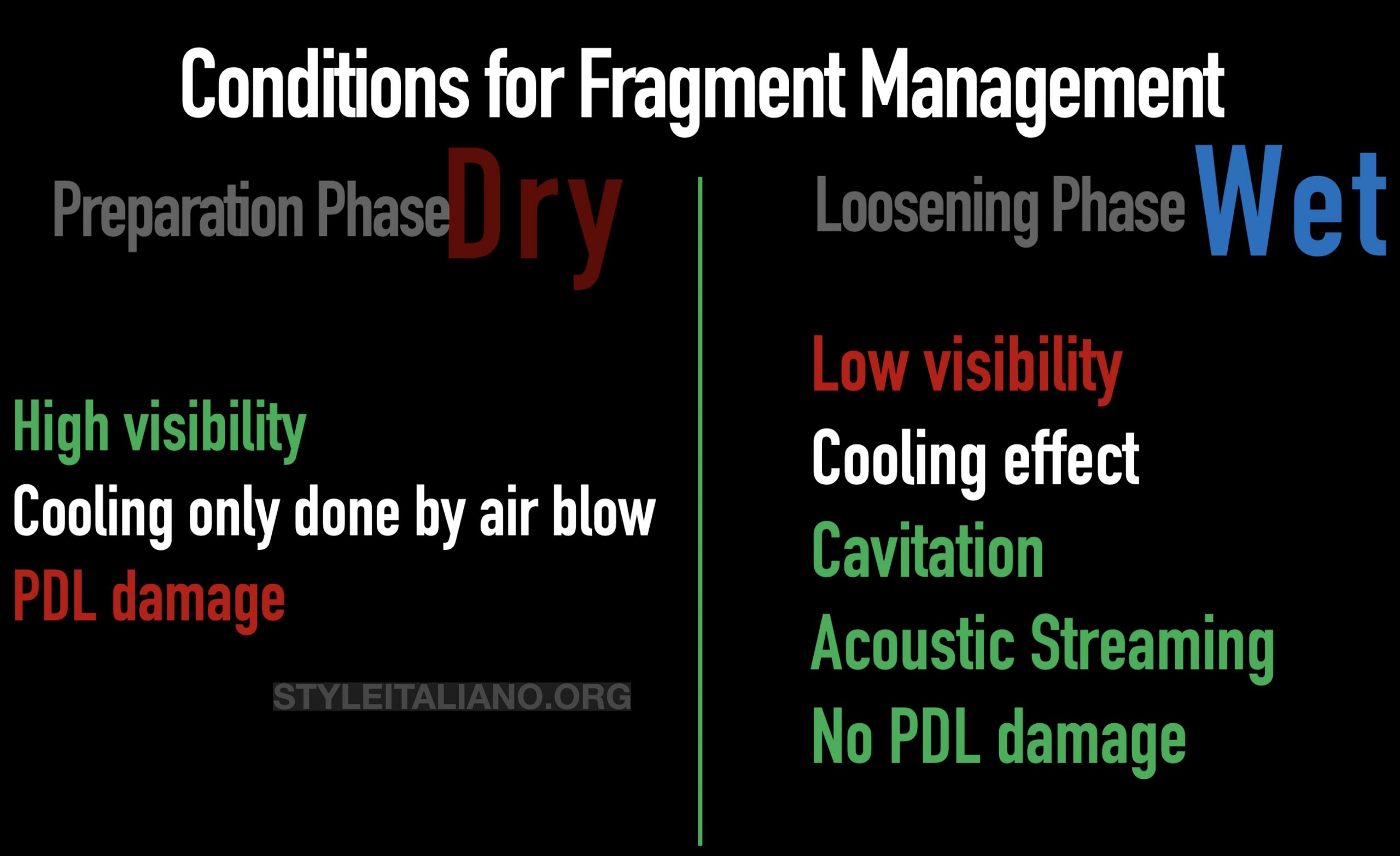
Fig. 5
Conditions for fragment management
It has to be highlighted that different stages of management dictate the use of different conditions and media.
During preparation phase, a dry condition was used to provide good visibility, where cooling during preparation is done using a stropko tip blow. It is important to adopt the mother in law rule [10 second rule] during the preparation phase to avoid periodontal damage
During the loosening phase, wet condition is used to provide a cavitation effect and acoustic streaming that will aid in loosening
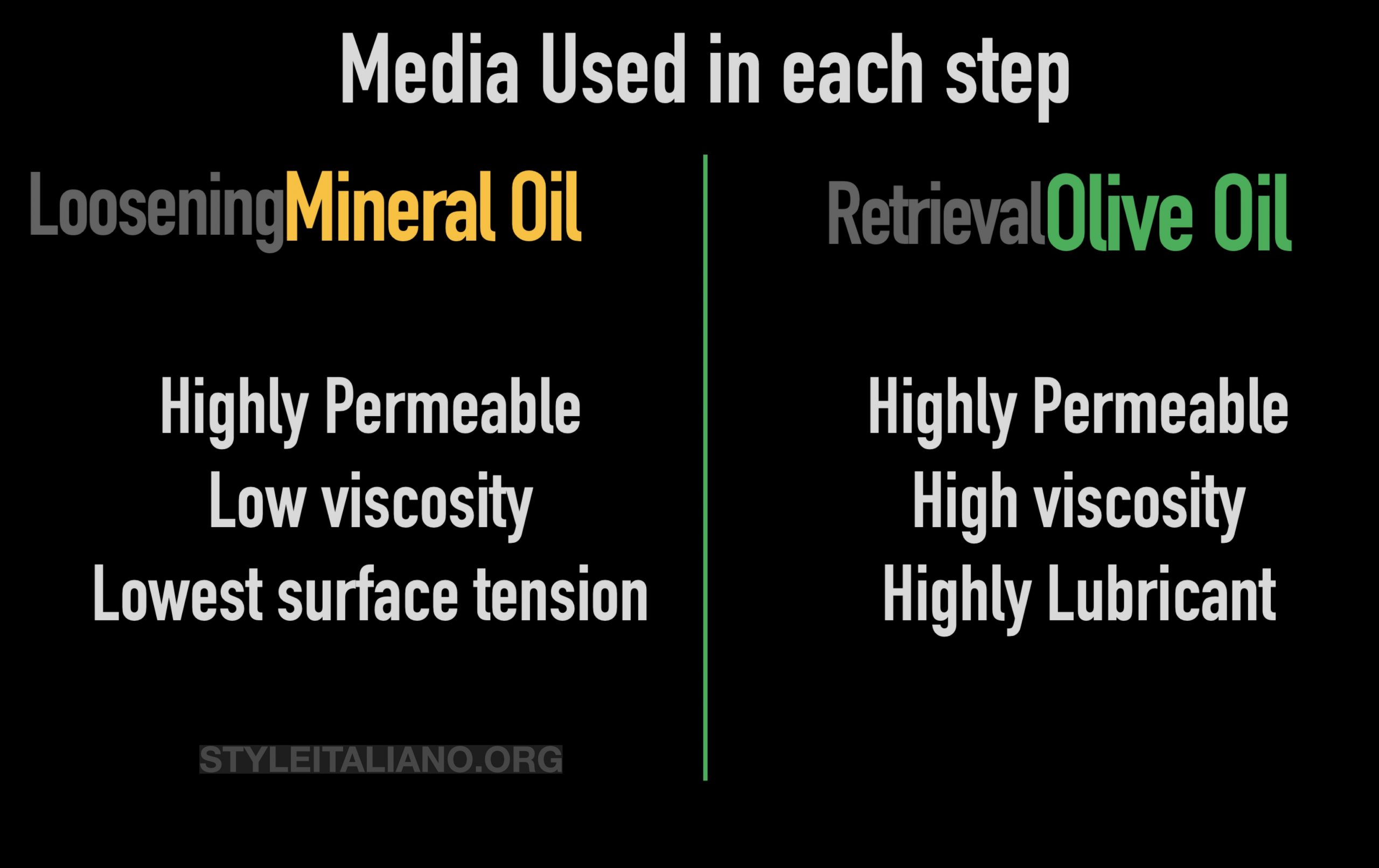
Fig. 6
Type of media used in each step of management:
During the loosening phase, Mineral oil [Johnson’s baby oil] was used as it permeates beneath the fragment well owing to low surface tension and viscosity
During the retrieval attempt, based on the recommendation of Dr. Yoshi Terauchi, olive oil has been used owing to its high lubrication potential as well as its high viscosity.
Retrieval attempts using Ultrasonic activation
Once the fragment become dancing in the root canal space, Olive oil was used to fill the pulp chamber to the cavo-surface margin. An ultrasonic tip was activated in the preparation site and labially [alternatively] until the fragment popped out from the root canal [Video]
It appeared that the fragment was a broken Endo-Z bur

Fig. 7
Visual Confirmation
After retrieval, high magnification was used to confirm that the root canal space is free from any impediment.
Canal preparation was done using reciprocating files [45/.05]

Fig. 8
Obturation:
Following cone fitting procedures, the root canal was obdurated using GP and resin sealer using warm vertical compaction technique.
Conclusions
- Instruments that are designed to operate in the pulp chamber [such as; Endo-Z burs] should never be used in the root canal as this bears the risk of damage to the tooth to fracture of the misplaced instrument
- Treatment planning and the use of proper instruments and materials are of prime importance when dealing with root canal impediments
- The use of high magnification and illumination during management of root canal impediments is essential. This will lead to maximum conservation of the tooth tissues which has a direct influence on tooth survival after root canal treatments
Bibliography
1- Fracture of Separated File Fragments by Using Ultrasonic Vibration under Various Canal Conditions. J Endod 2013;39:1300–1305)
2- Evaluation of the Efficiency of a New File Removal System in Comparison With Two Conventional Systems. J Endod 2007;33:585–588