Everything changes except for anatomy!
26/12/2023
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Successful root canal therapy requires a thorough knowledge of both the external and internal anatomy of root and its canal morphology. Extra roots or root canals, if not detected, are a major reason for endodontic failure.Maxillary molars show considerable anatomic variation and abnormalities with respect to the number of roots and root canals.
The anatomical characteristics of permanent maxillary first molars are complex and are generally described as teeth with three roots: Two buccal root canals and one palatal root canal. In recent articles, two palatal and two mesiobuccal root canals have been reported separately. The incidence of a second mesiobuccal root canal (MB2) is 58.4% (Asghari et al,2015). While the incidence of a second distobuccal canal is between 1.6% and 9.5% (Martins et al, 2018). The anatomy and morphology of roots in the permanent maxillary first molar and root canals vary greatly.
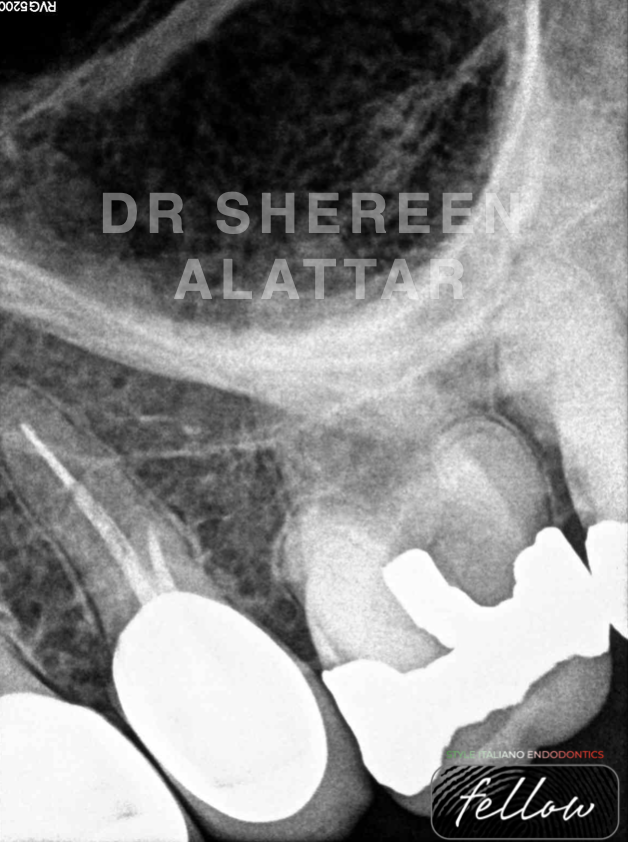
Fig. 1
A 41-year-old gentleman was referred to my office suffering from
spontaneous and intermittent pain that had worsened, particularly at night, on the upper left side of the jaw.
The diagnosis based on clinical examination and X-ray imaging, was symptomatic irreversible pulpitis. Nonsurgical endodontic therapy was initiated for the left maxillary first molar.
The mesiodistal width of the buccal roots in the preoperative radiograph suggests the presence of a second root canal in each of those roots. (Fig. 1)
To start off, a long shank round diamond bur was used to remove the old amalgam filling and prepare the access cavity.
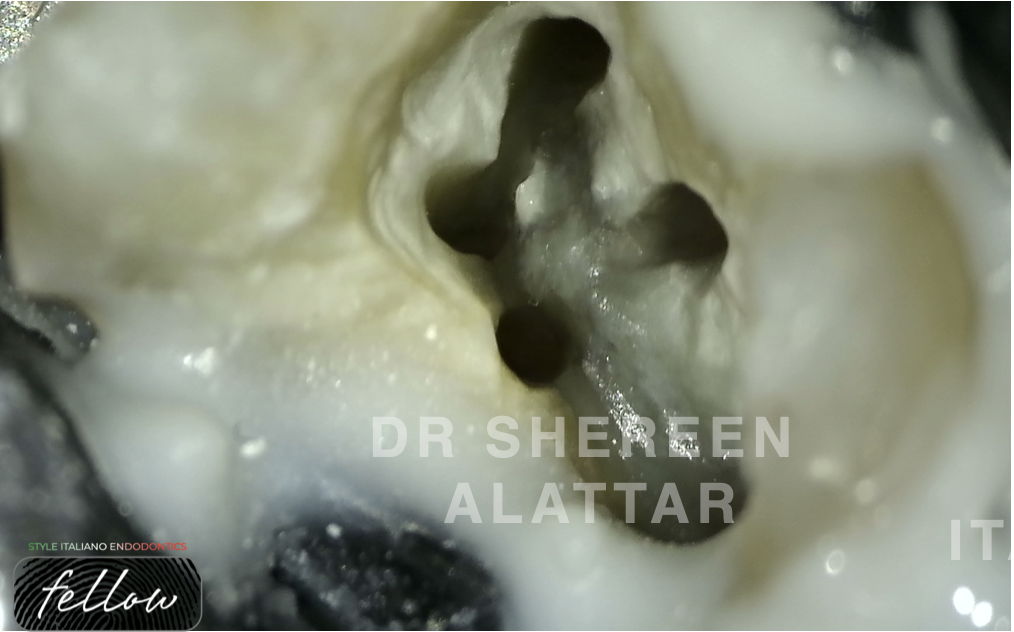
Fig. 2
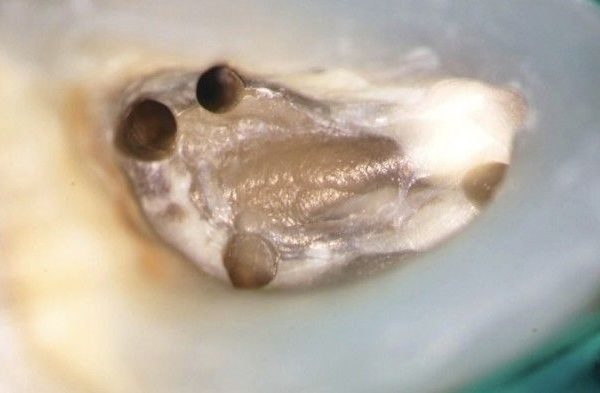
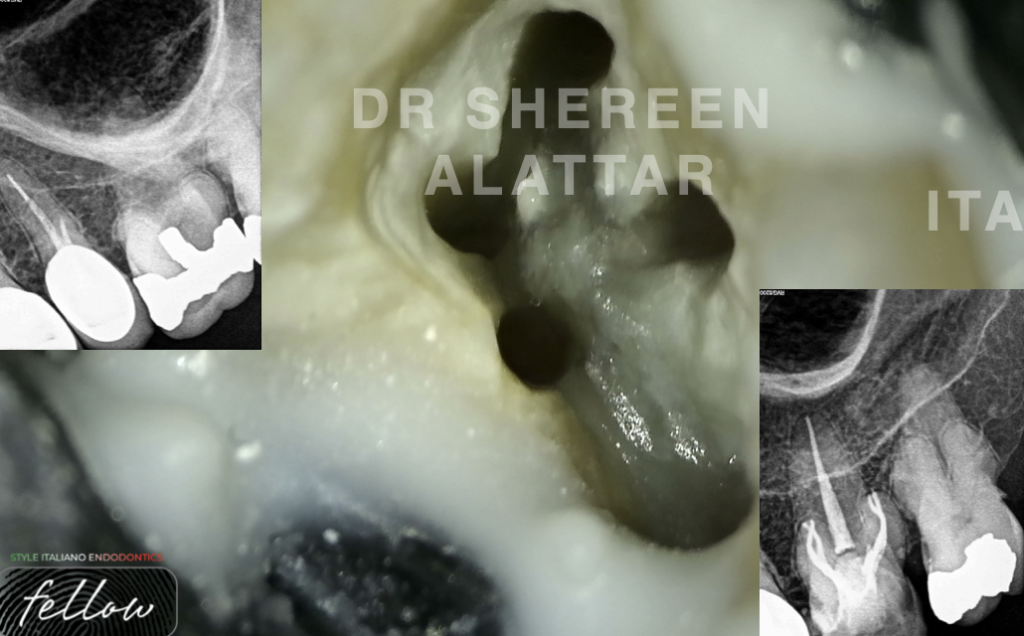
Upon inspection with a DG-16 endodontic explorer under the operating microscope, the pulp chamber floor revealed 3 canal openings. The mesiobuccal (MB1), distobuccal, and palatal canal orifices were located in their regular locations at the angles in the floor-wall junction.
Afterwards, I switched to the piezoelectric ultrasonics instead of high speed handpiece to rectify the access cavity.
Further removal of dentinal shelf beginning from the orifice of the mesiobuccal canal and moving toward the orifice of the palatal canal with ultrasonic tip (ET 18D tip, Acteon) clearly unveiled the orifice of the MB2 canal. The same was applied to the distobuccal canal and therefore DB2 canal was found.
The use of piezoelectric ultrasonics in endodontic access refinement can expose what many clinicians refer to as a "dentinal roadmap", for instance; differentiating the pulp chamber floor from secondary dentin, possibly provide clues to the location of hidden canals.
A well designed and well executed access is paramount to achieving proper cleaning, shaping, and obturation of the root canal system (Plotino et al, 2007).
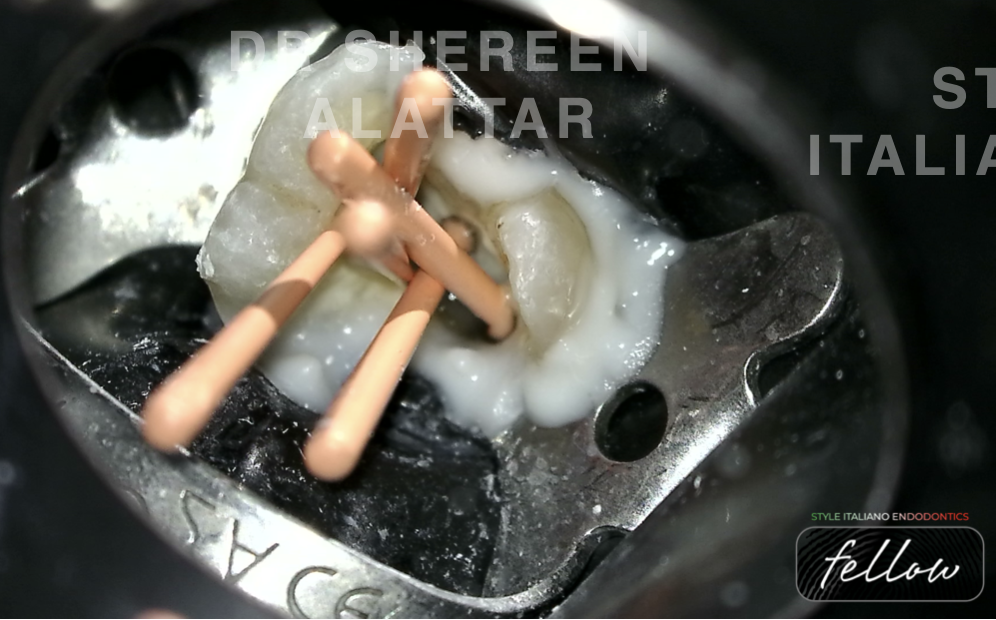
Fig. 3
Cleaning and shaping were performed using rotary instruments along with 17% EDTA gel (canal lubricant and chelating agent), 5.25% sodium hypochlorite was used as the working solution. All the mesiobuccal and distobuccal canals were enlarged to size 30/0.04, whereas the palatal canal was enlarged to size 40/0.04.
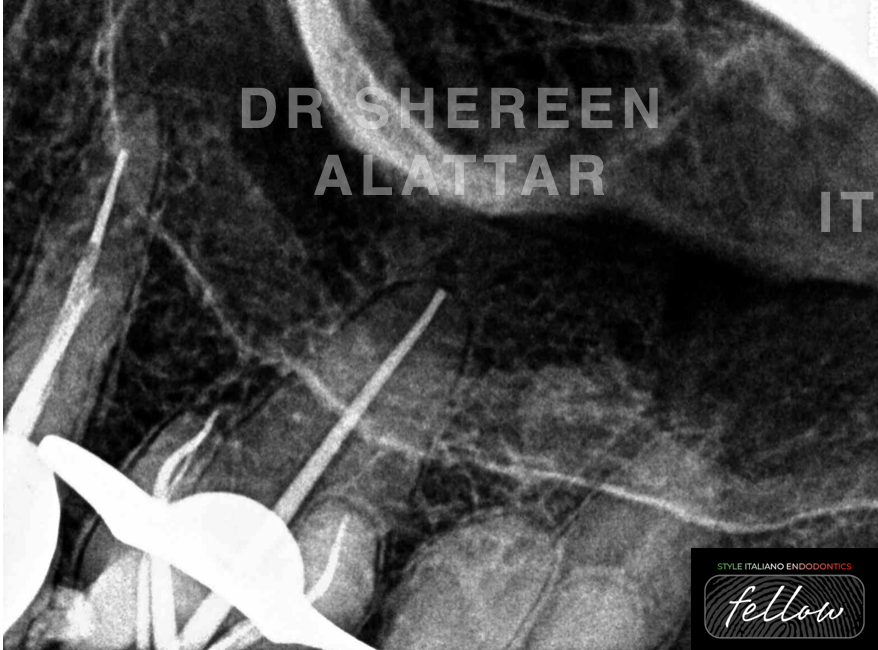
Fig. 4
Fine medium gutta percha cones were customised using the perforated ruler and a master Cone fit radiograph was taken

Fig. 5
Obturation was performed using warm vertical compaction technique where System B was used with the Buchanan fine plugger and the temperature was set at 200°C.

Fig. 6
About the author:
Dr Shereen Alattar (DDS, MSc) has graduated from Saint Joseph University in Beirut, Lebanon, where she received her Master’s Degrees in the specialisation of Endodontics. She works in a referral-based practice limited to endodontics in Amman, Jordan.
She is a fellow member in Style Italiano Endodontic Group and an active member in the Jordanian Scientific Committee of the Jordanian Dental Association and in the Jordanian endodontic society
Conclusions
Ultrasonics allow me to preserve precious dentin and get the hidden canal orifices uncovered. To everyone asking whether the use of ultrasonics is a luxury in endodontics; I say, habit converts luxury into necessity.
Everything has changed, except the anatomy of teeth and their roots. Therefore, we must become students of endodontic anatomy. Students of endodontic anatomy know that their clinical success is absolutely dependent on their ability to treat root canal systems to their full apical and lateral extents; they know how to choose files to match the canal form they are in but, most of all, they expect everything going forward to change except the anatomy.
Bibliography
- Asghari V, Rahimi S, Ghasemi N, Talebzadeh B, Norlouoni A. Treatment of a Maxillary First Molar with Two Palatal Roots. Iran Endod J. 2015;10:287–289.
- Martins JNR, Gu Y, Marques D, Francisco H, Caramês J. Differences on the Root and Root Canal Morphologies between Asian and White Ethnic Groups Analyzed by Cone-beam Computed Tomography. J Endod. 2018;44:1096–1104.
- Plotino, G., Pameijer, C. H., Grande, N. M., & Somma, F. (2007). Ultrasonics in endodontics: a review of the literature. Journal of endodontics, 33(2), 81-95
- Briseño-Marroquín B, Paqué F, Maier K, Willershausen B, Wolf TG. Root Canal Morphology and Configuration of 179 Maxillary First Molars by Means of Micro-computed Tomography: An Ex Vivo Study. J Endod. 2015;41:2008–2013.