Endodontic management of a mandibular first molar with pulp stone obliterating the floor of pulp chamber – a case report.
29/07/2021
Garima Poddar
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
The goals of an endodontic treatment are to prevent and intercept the process of pulpal/ peri radicular pathosis and to also prevent its reinfection after the treatment. For achieving this, a good diagnosis of the case, followed by chalking out a feasible and appropriate treatment plan and its execution is important. Starting from good clinical and radiographic evaluation of the case, to following a good treatment protocol and using necessary tools and techniques proves to be helpful for the same.
This article is a case report of root canal treatment of a mandibular first molar with pulp stones obliterating the floor of the pulp chamber, and its endodontic management which included, pulp stone removal, proper cleaning, shaping and tri dimensional obturation.
Case Report-
Patient information –
Age- 30
Gender- Male
Medical history- Non contributory.
Tooth identification- Mandibular right first molar (tooth 46)
Chief complaint-
Patient complained of pain and discomfort in mandibular right posterior region since 15 days. The tooth showed tenderness to percussion.
Diagnosis- Pulpal –
Peri apical – Chronic apical periodontitis.
Preliminary procedures:
1. Local anesthesia- Inferior alveolar nerve block was given using 2% lignocaine with adrenaline injection.
2. Rubber dam isolation- tooth number 46 was isolated using rubber dam isolation.
3. Magnification- The root canal treatment was done under a dental operating microscope for better visualization.

Fig. 1
The following details were seen on the radiograph of the tooth-
- Deep disto proximal decay was observed which was involving pulp.
- Pulp stone could be appreciated obliterating the pulp chamber of the tooth.

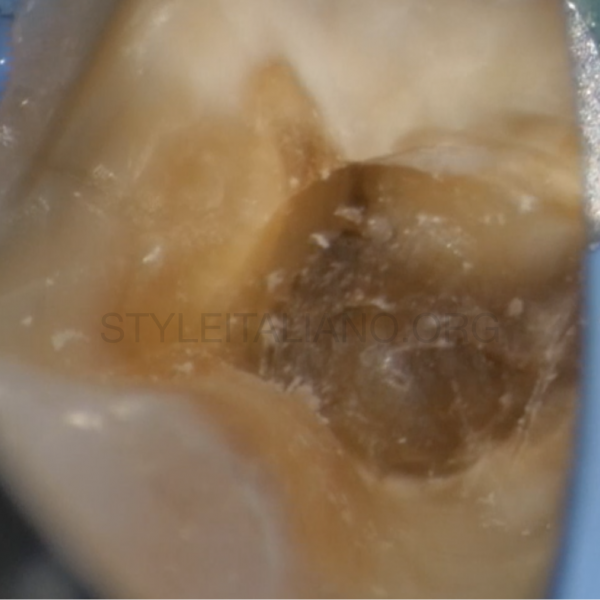
Fig. 2
The tooth was isolated, caries was excavated, pre-endo build up was done using liquid dam.
There was some blood oozing from beneath the pulp stones.

Fig. 3
Pulp stones were removed using ultrasonic tips by breaking the large chunk which was obliterating the entire floor, into smaller fragments.

Fig. 4
Pulp stones were removed using ultrasonic tips by breaking the large chunk which was obliterating the entire floor, into smaller fragments.

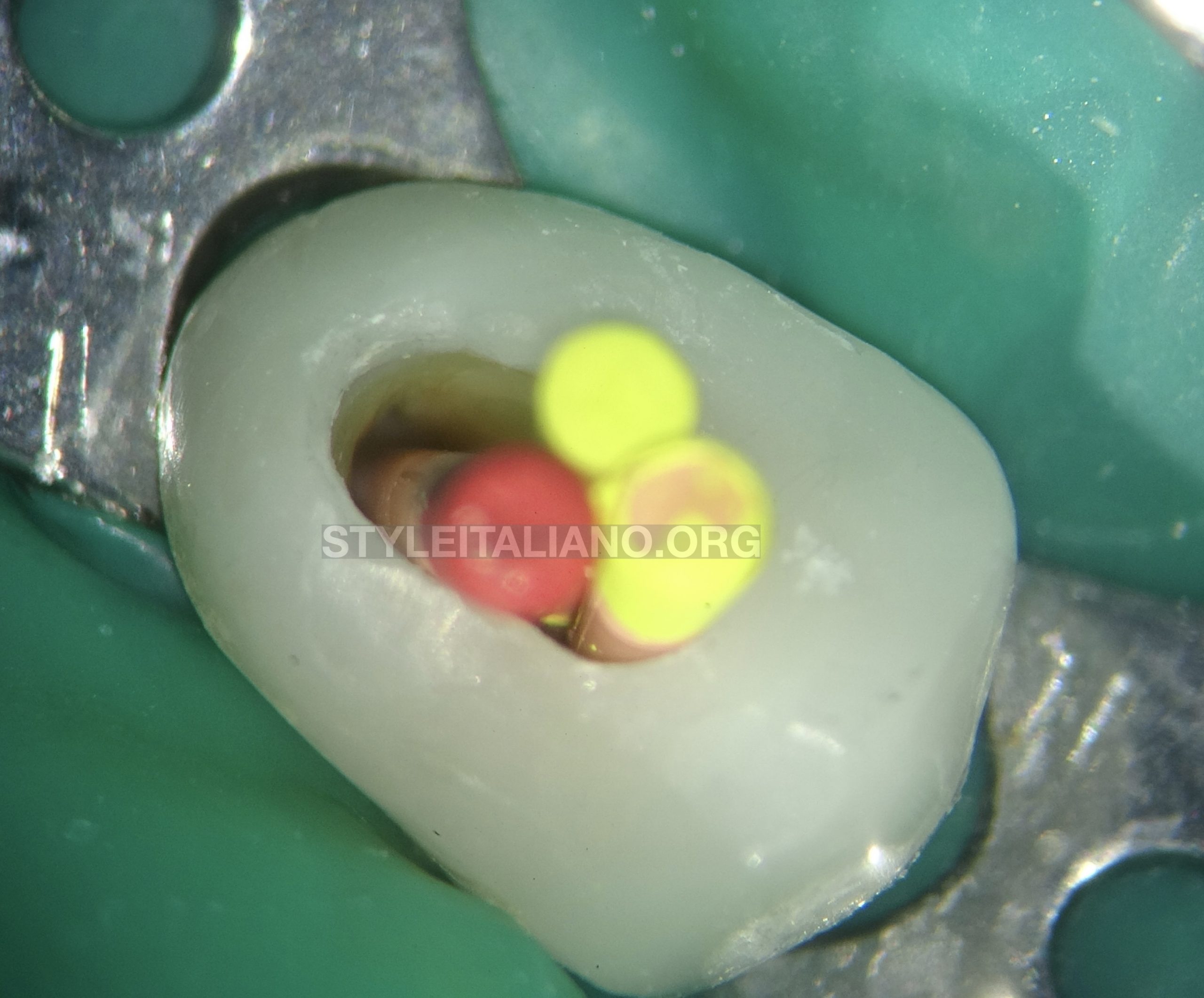
Fig. 5
They were then lifted up with the help of spoon excavator.

Fig. 6
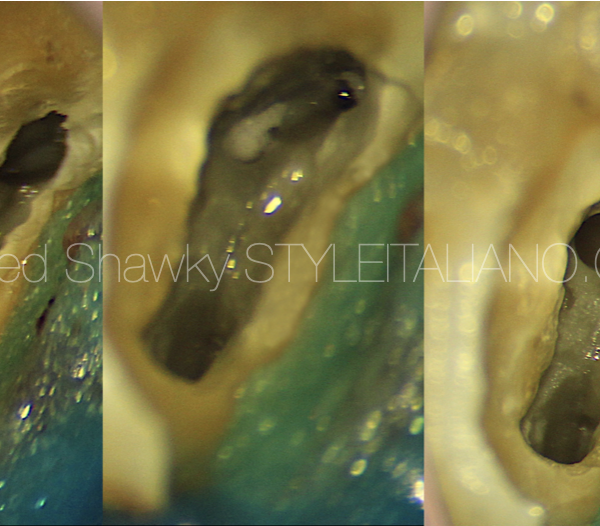
Once, the floor was clear of the pulp stones, the canals were negotiated and cleaning and shaping of canals was done.
One large distal canal and two mesial canals were found.
The isthmus area between mesio buccal and disto buccal was troughed using ultrasonic tips and was cleaned properly.

Fig. 7
Shaping protocol-
Coronal flaring was done using One flare file (Micromega, France).
10k file was used to instrument the canal till in became loose in the canals.
Glide path preparation was done with the help of One G file (Micromega, France).
The canals were shaped up till 25-06% using 2 shape files( Micromega).
Irrigation protocol-
Throughout shaping, 5.25% sodium hypochlorite was used after each file. Side vented 30 gauge needles were used for irrigation.
After shaping, the following protocol in each canal, was used for irrigation and activation of irrigants-
1). 17% EDTA – 1ml per canal was used which was activated with an ultrasonic activator.
2). Distilled water used to flush the canals.
3). 5.25 % sodium hypochlorite was then injected in the canal and was ultrasonically activated. (4 such cycles repeated per canal)
4). Distilled water.

Fig. 8
Canals were dried with paper points. Cone fit intra oral radiograph was made.
Canals were obturated with warm vertical compaction technique using EQ-V (Meta biomed). Sealer used was Ah plus (Dentsply Maillefer).

Fig. 9
Immediate post obturation x-ray revealed an interesting fill in the apical third of distal canal. An apical delta was filled up.

Fig. 10
Another immediate post obturation radiograph was made at a different angulation using tube shift technique.
Conclusions
A sound knowledge of the root canal anatomy and reading the pre-operative radiographs well, is important for performing the root canal treatment properly.
Using magnification and good source of illumination helps in treating such teeth in a conservative manner, because of better visualization.
Ultrasonics plays a vital role in pulp stone removal, refining the access cavity and even for activation of irrigating solutions.
Also, determining the correct working length of each canal is a very important step in a root canal treatment. Thorough cleaning, shaping and then a three dimensional obturation of canals till the exact working length, plays a vital role in a good prognosis of a tooth being endodontically treated.
Pulp stones obliterating the floor and canals could lead to missing out of a canal and might result in a failed endodontic treatment.
Their interpretation on radiographs and removal with the aid of magnification, illumination and ultrasonic tips proves to be helpful in carrying out the treatment of such teeth
Bibliography
- Goga R, Chandler NP, Oginni AO. Pulp stones: A review. Int Endod J. 2 0 0 8 ; 41( 6 ) : 4 5 7– 4 6 8 .
- Plotino, Gianluca & Pameijer, Cornelis & Grande, Nicola & Francesco, Somma. (2007). Ultrasonics in Endodontics: A Review of the Literature. Journal of endodontics. 33. 81-95. 10.1016/j.joen.2006.10.008.
- Fulton S. Yee, Jay Marlin, Alvin Arlen Krakow, Poul Gron,Three-dimensional obturation of the root canal using injection-molded, thermoplasticized dental gutta-percha,Journal of Endodontics,Volume 3, Issue 5,1977,Pages 168-174,ISSN 0099-2399.