Denticles/Pulp stones- A hinderance or not?
15/06/2023
Garima Poddar
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
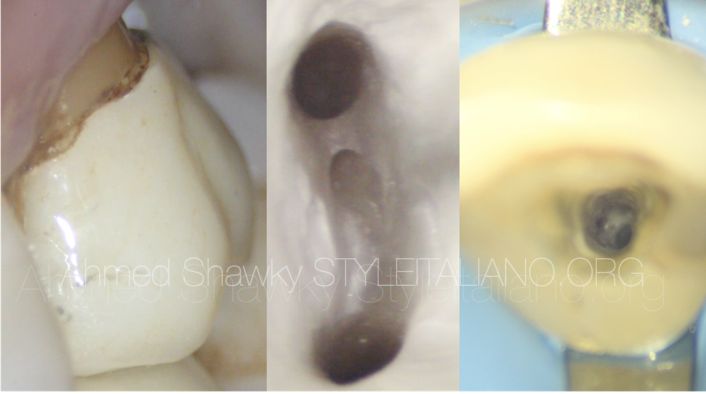
Pulp stones are defined as foci of calcifications that form within the pulp chamber, more frequently in the coronal pulp cavity and sometimes in radicular pulp space.
In the year 1921, Norman and Johnson first mentioned about dental pulp calcifications and called them dental pulp nodules. These were later termed as denticles.
Kronfeld and Boyle classified pulp calcifications histologically into two types- 1. True forms- This type is made up of irregular dentine and is lined by odontoblasts.
2. False forms -formed from degenerative cells which calcify.
They may also be classified as –
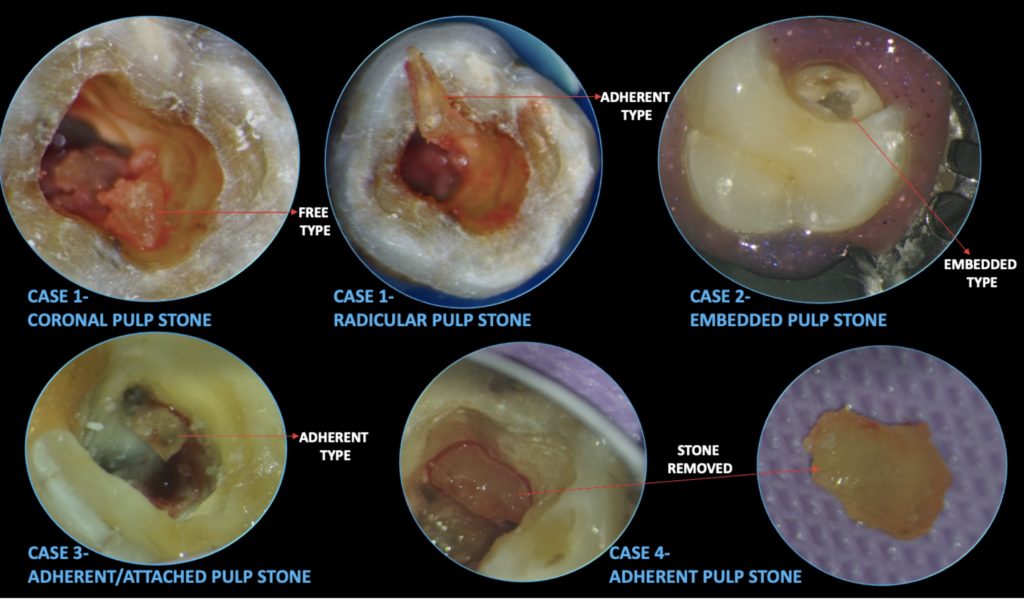
- Free- which lie freely within the pulp.
- Adherent- adhere to the walls of the chamber.
- Embedded- stones which are embedded in dentine.
Pulp stones have calcium- phosphorus ratios almost comparable to that of dentin. A tooth may have single or multiple stones, the sizes of which varies, ranging from small to big masses (Johnson and Bevelander 1956). The occurrence of pulp stones is observed more frequently in coronal region but they have also been reported in radicular pulp (Arys et al. 1993).
Etiology-
The exact etiology of denticle formation in not very clear. Pulp stones can be present in diseased or even healthy teeth. They have also been observed in unerupted or impacted teeth.
Some factors which might be contributing to pulp stone formation are- Ageing, periodontal disease, orthodontic tooth movement, caries, restored teeth and genetic predilection.
Prevalence-
There have been multiple studies about pulp stones and its prevalence, but range according to those reports varies from 8% to 90 %, as the technique and type of study design differs.
Clinical relevance-
The presence of a pulp stone, in case of absence of any other symptoms, should not be translated as a disorder needing a root canal treatment.
The calcifications within the pulp chamber might block access to the canals, and may cause hinderance while instrumenting the canals. Pulp stones when obstructing the canal orifices, fend off easy passage of instruments down the canal, and thus may lead to substandard outcome of an endodontic treatment. (Pashley et al. 2002).
So, removal of pulp stones aids in better visualization of canal orifices and chances of missing out a canal is reduced. It also facilitates smooth instrumentation of canals which might have been prevented in case of presence of denticles within the pulp chamber.
Magnification, Ultrasonics, good access preparation and use of appropriate instruments have made management of cases with pulp stones easier than before.
This article, describes 4 cases where, pulp stones of different sizes and types were located and removed during the root canal treatment.
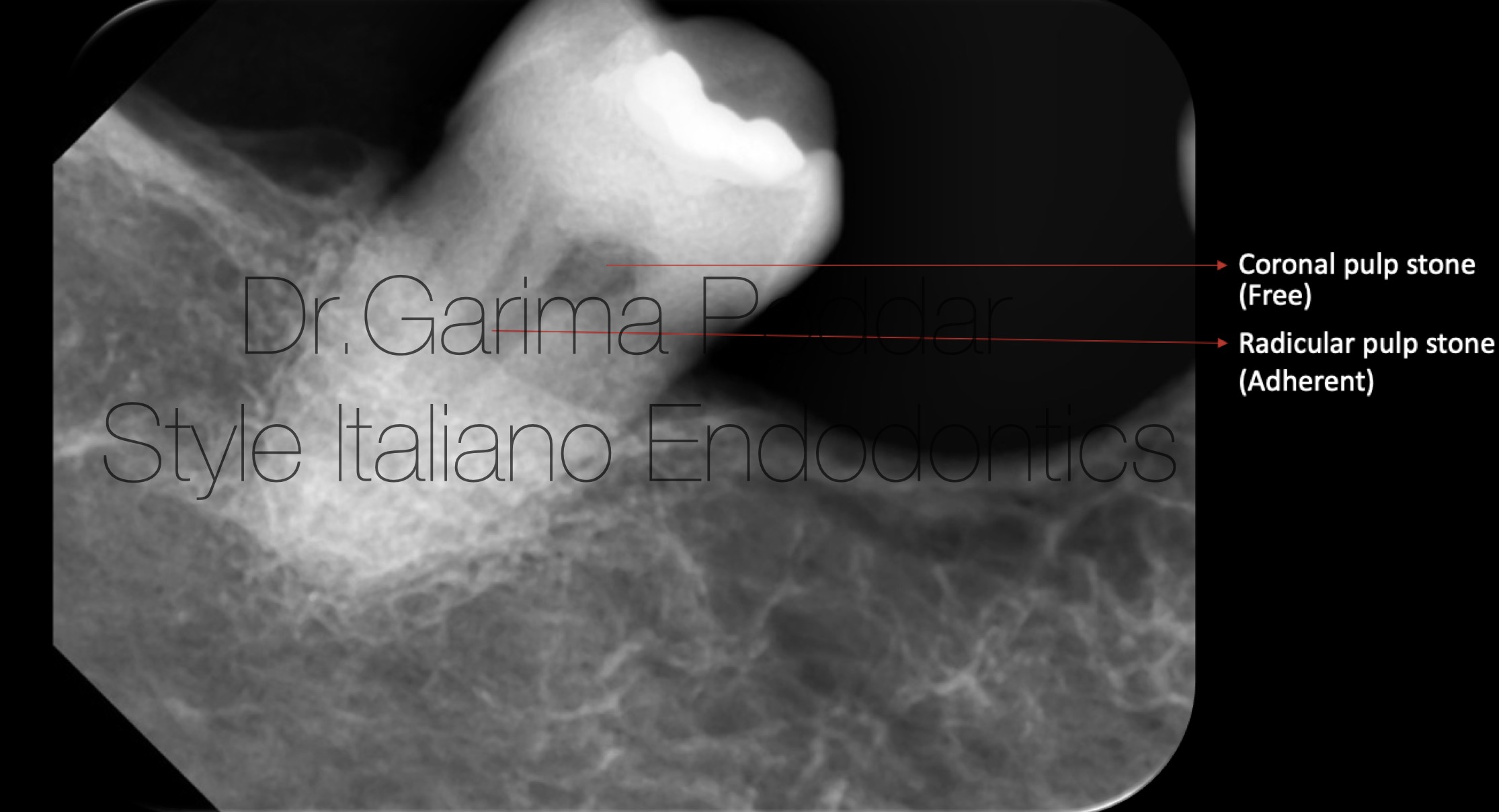
Fig. 1
Case report 1-
A 75 years old female patient reported with pain and tenderness mandibular right posterior region.
On clinical examination, it was observed that tooth number 47, which had history of restoration was symptomatic. The tooth was tender to percussion.
Radiographic evaluation-
Pre-operative radiograph revealed two pulp stones- one appeared to be free in the pulp chamber and the other one occupied the canal space till coronal third of the root length.
A highly radio-opaque restoration could also be appreciated.
Diagnosis of chronic irreversible pulpitis was made with the help of pulp tests, clinical and radiographic evaluation.
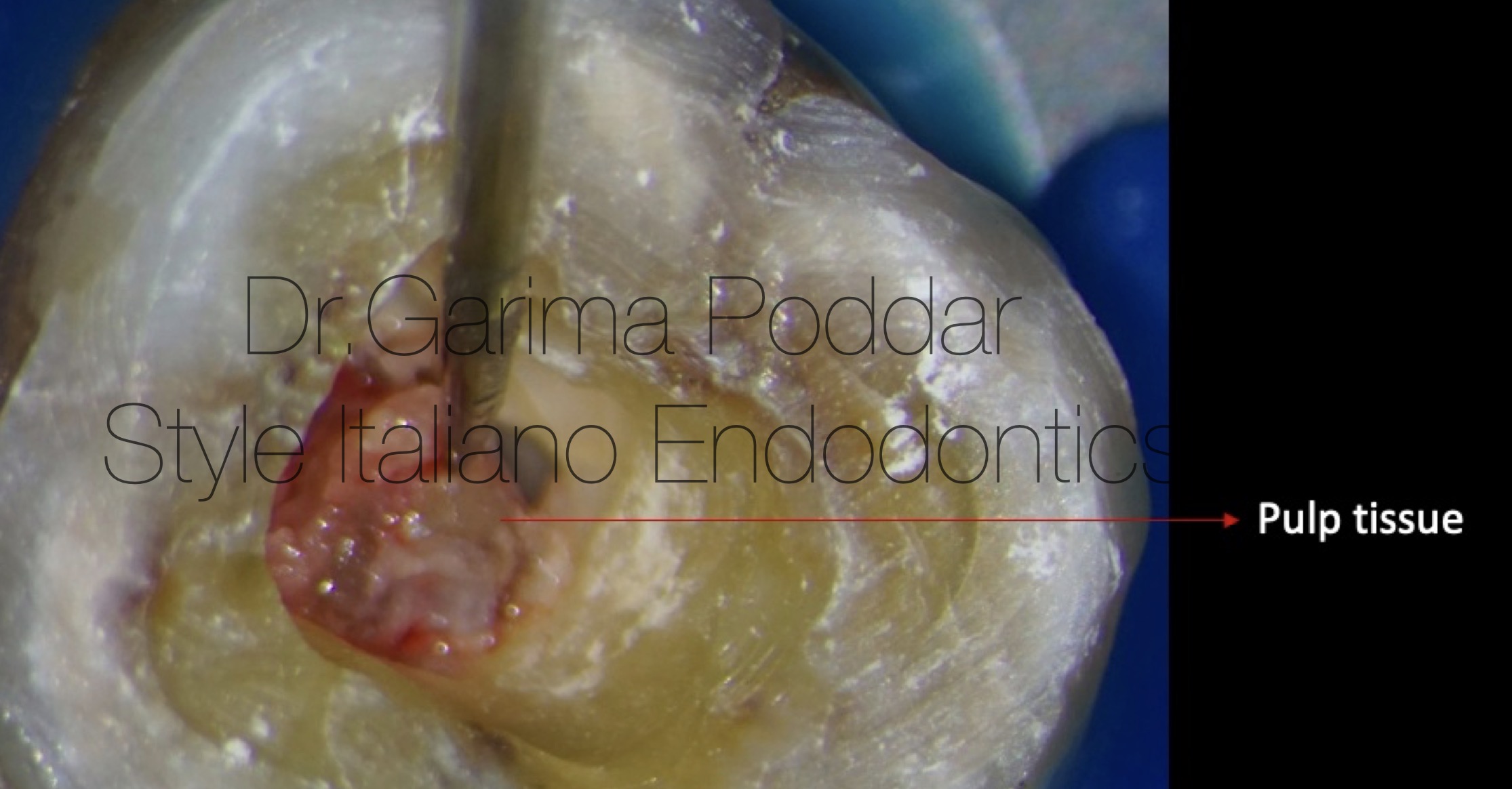
Fig. 2
Local anesthesia was administered. Inferior alveolar block was given using 2% lignocaine with adrenaline.
The tooth was isolated with rubber dam and access preparation was done.
Masses of pulp were pulled out of the pulp chamber.
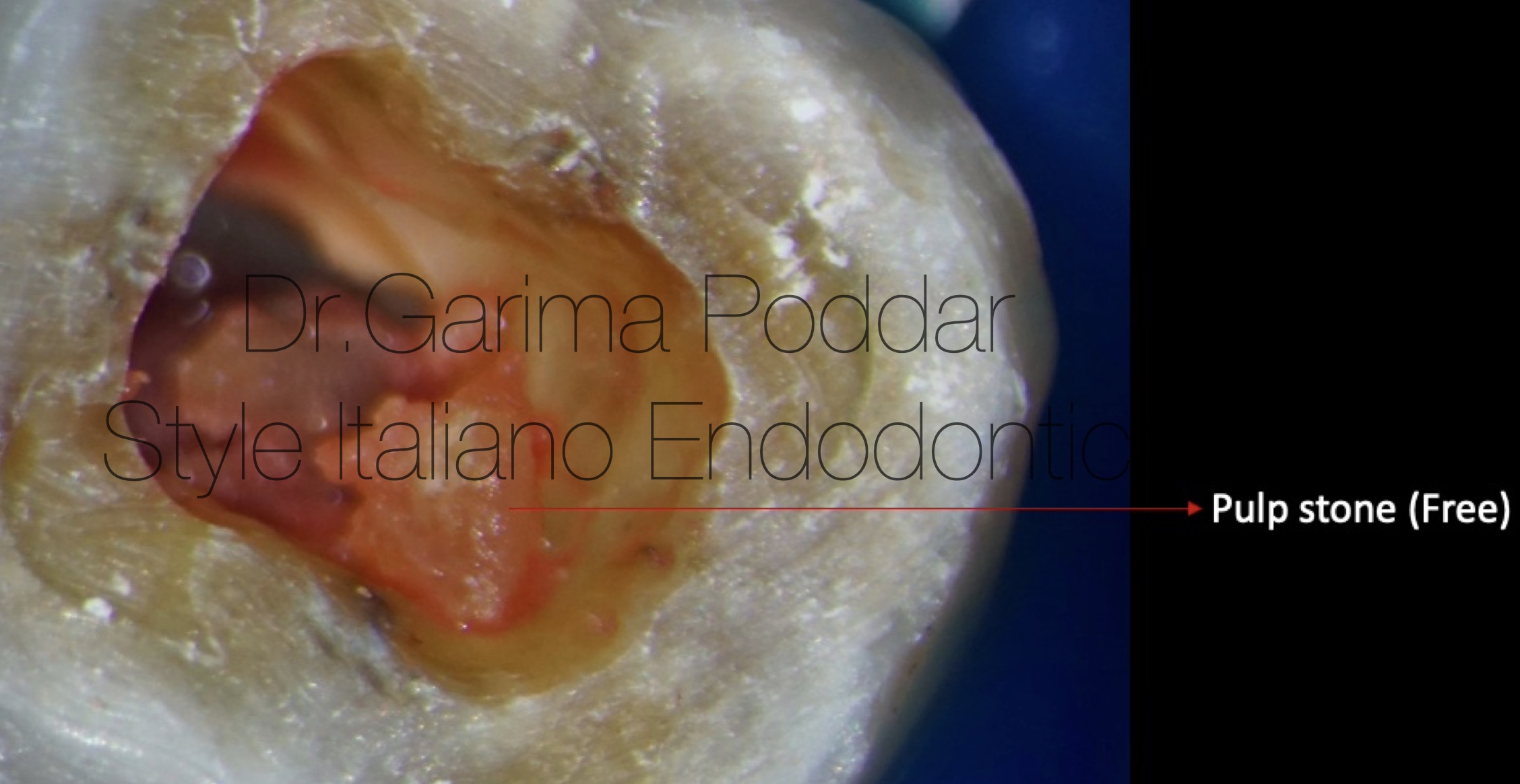
Fig. 3
Along with the pulp tissue, a coronal pulp stone was also removed.
For such a pulp stone which is present freely and is not attached to the walls, even a sharp spoon excavator serves to be helpful to extract it out of the cavity.
Followed by this, irrigation with 5.25% sodium hypochlorite was done.
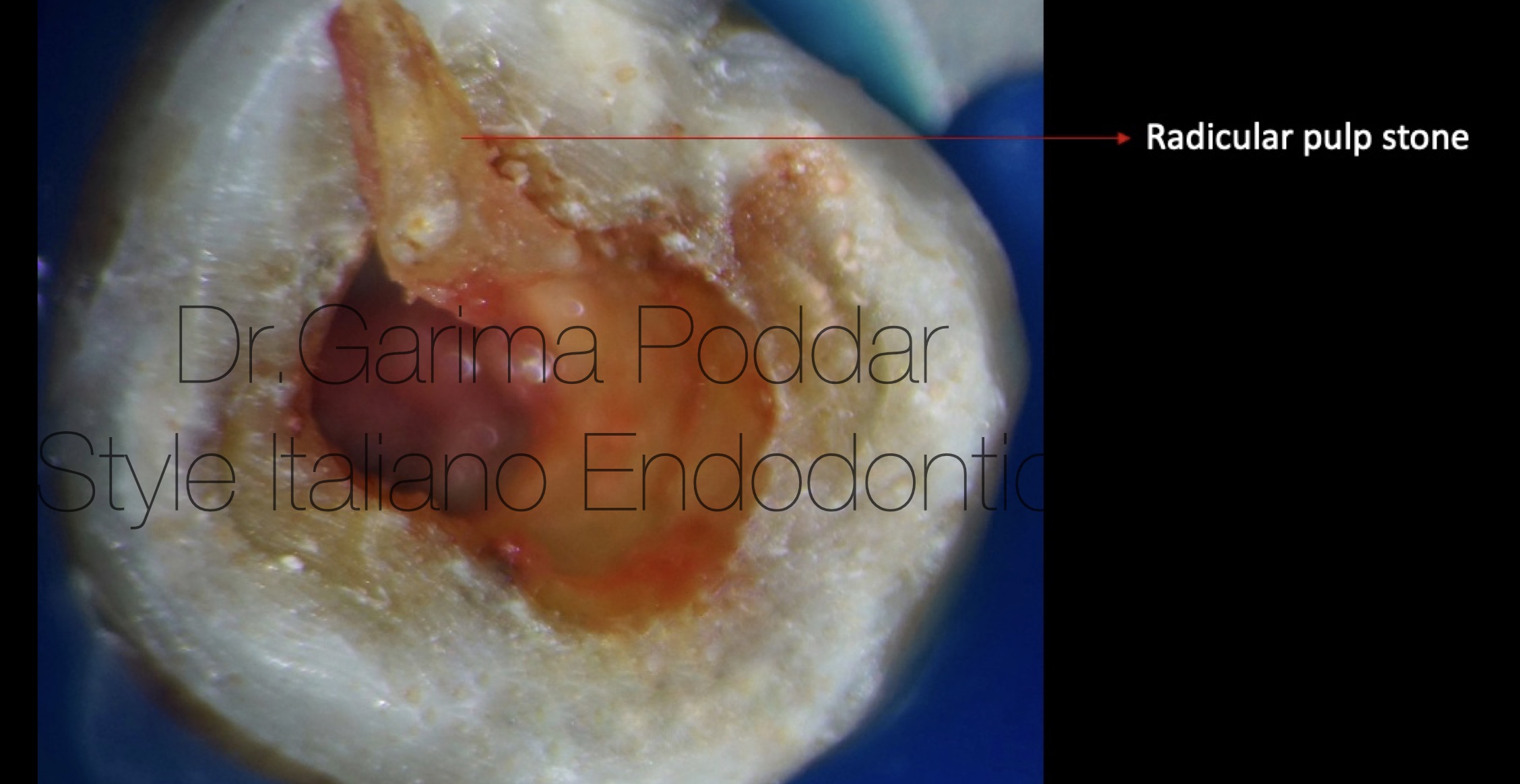
Fig. 4
The radicular pulp stone was attached to the walls. For its removal, ultrasonic tips ( E5D and E6) were used.
Ultrasonic tips helped in conservative removal of the radicular pulp.
Shaping protocol-
There was a single large canal, which was shaped using a combination of manual( 15k, 20k) and rotary files (Hero gold, Micromega, France).
Irrigation protocol-
5.25% sodium hypochlorite, distilled water and 17% EDTA were used for thorough irrigation and the solutions were ultrasonically activated.
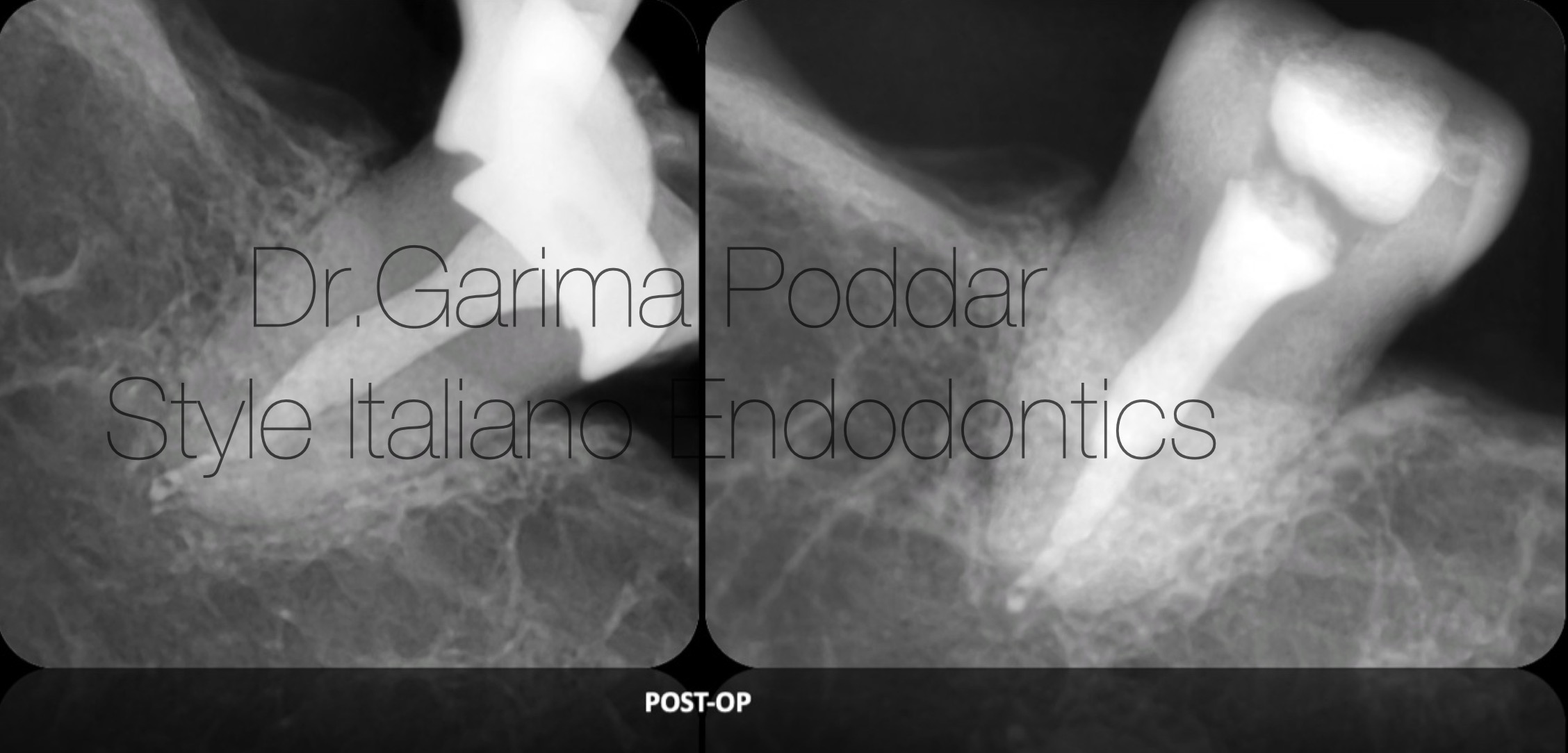
Fig. 5
Obturation protocol-
Since the canal was a single large one, with irregular cross section, squirting technique was chosen as the technique of choice. The backfill unit of obturation device (EQ-V, meta biomed) was used to introduce thermo-plasticized gutta percha in the canal till its working length.

Fig. 6
Case report 2–
A 26 year old, male patient was referred to our hospital by a dentist colleague. He reported with caries and intermittent pain in maxillary right posterior region.
He gave history of pain during chewing food.
Clinical examination-
Deep mesio-proximal carious lesion was observed on clinical evaluation.
The tooth had slight tenderness to percussion.
Cold vitality test showed response which lingered on for 10 seconds.
Radiographic evaluation-
- Deep carious lesion, mesio-proximally, involving pulp could be appreciated on the radiograph.
- Peri-apically, radiolucency could be observed in relation with the palatal root.
- The entire pulp chamber, appeared to be obliterated with denticle. Outline of the pulp stone, appeared to be merged with the dentin walls, indicative of an embedded type of pulp stone.
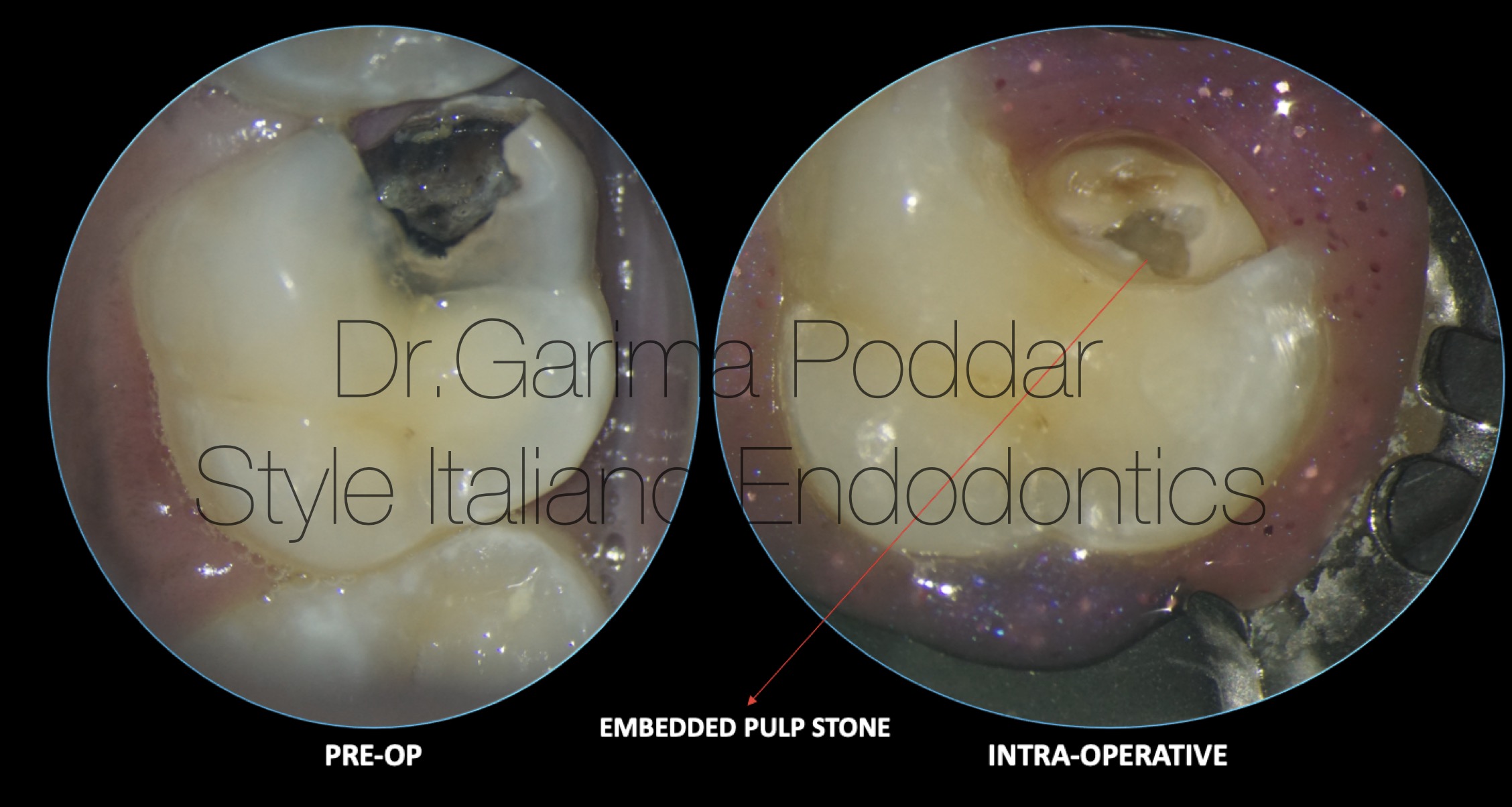
Fig. 7
Local anesthesia was administered, rubber dam isolation was done and access preparation was commenced.
The entire floor appreared to be obliterated with pulp stone.
Ultrasonic tips number E12D and E5D were used to enlarge the cavity outline in a controlled manner.
This pulp stone was of embedded type, so it was more challenging to detach the entire pulp stone.
With the help of ultrasonics, the stone was broken into pieces and in some regions, the pulp stone which was completely embedded in the tooth had to be crushed.
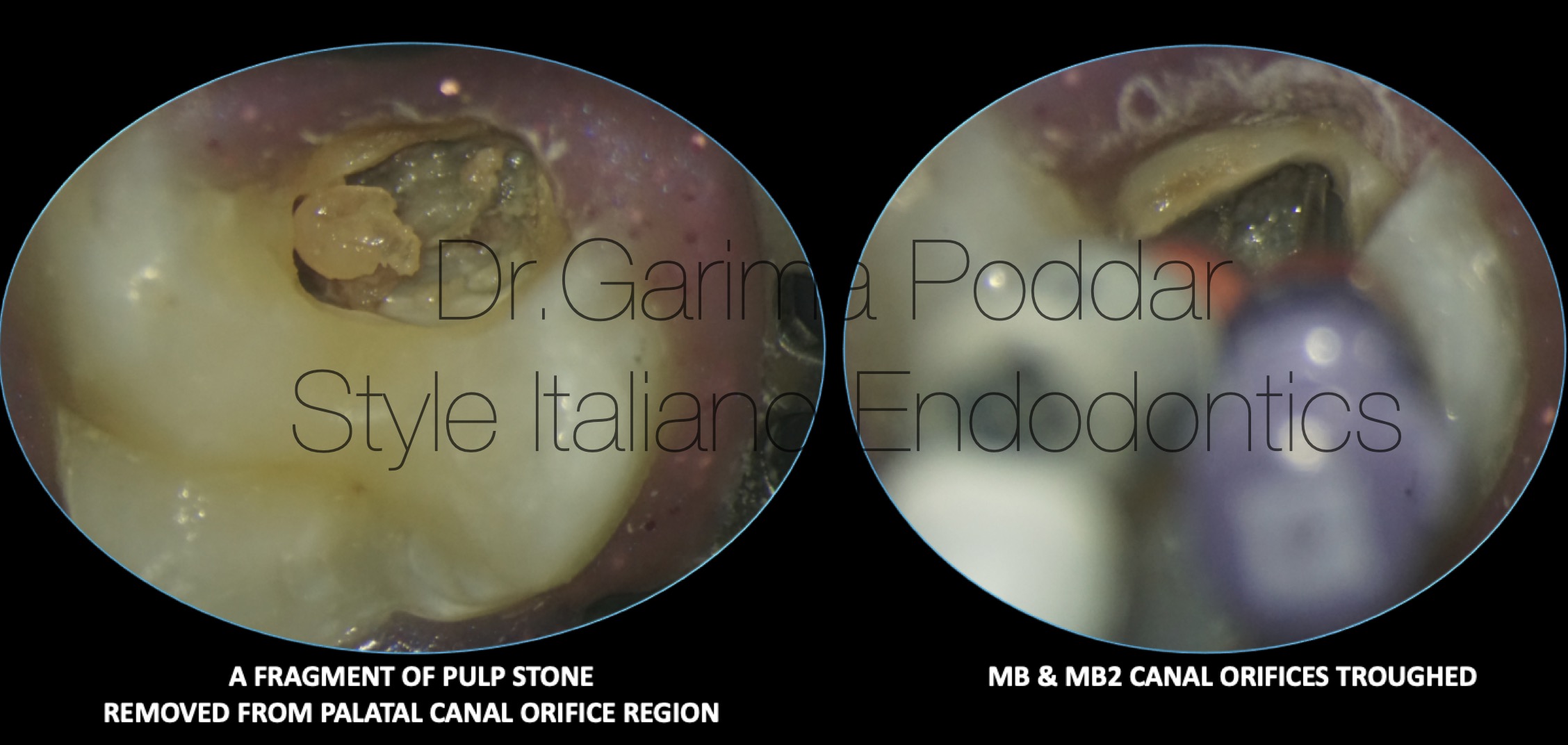
Fig. 8
MB2 canal orifice was troughed using ultrasonics in a conservative manner.
Ultrasonics, helped in attaining good access to the canals and removing all hinderances, without any aggressive cutting of dentin.
Shaping protocol-
Coronal flaring was done with one flare file(Micromega, France).
10K file was used to negotiate palatal, distobuccal and mesiobuccal canals, while 8K file was used to explore the MB2 till working length.
Working length was determined using electronic apex locator.
Irrigation protocol-
5.25% sodium hypochlorite, distilled water and 17% EDTA were used for thorough irrigation and the solutions were ultrasonically activated.
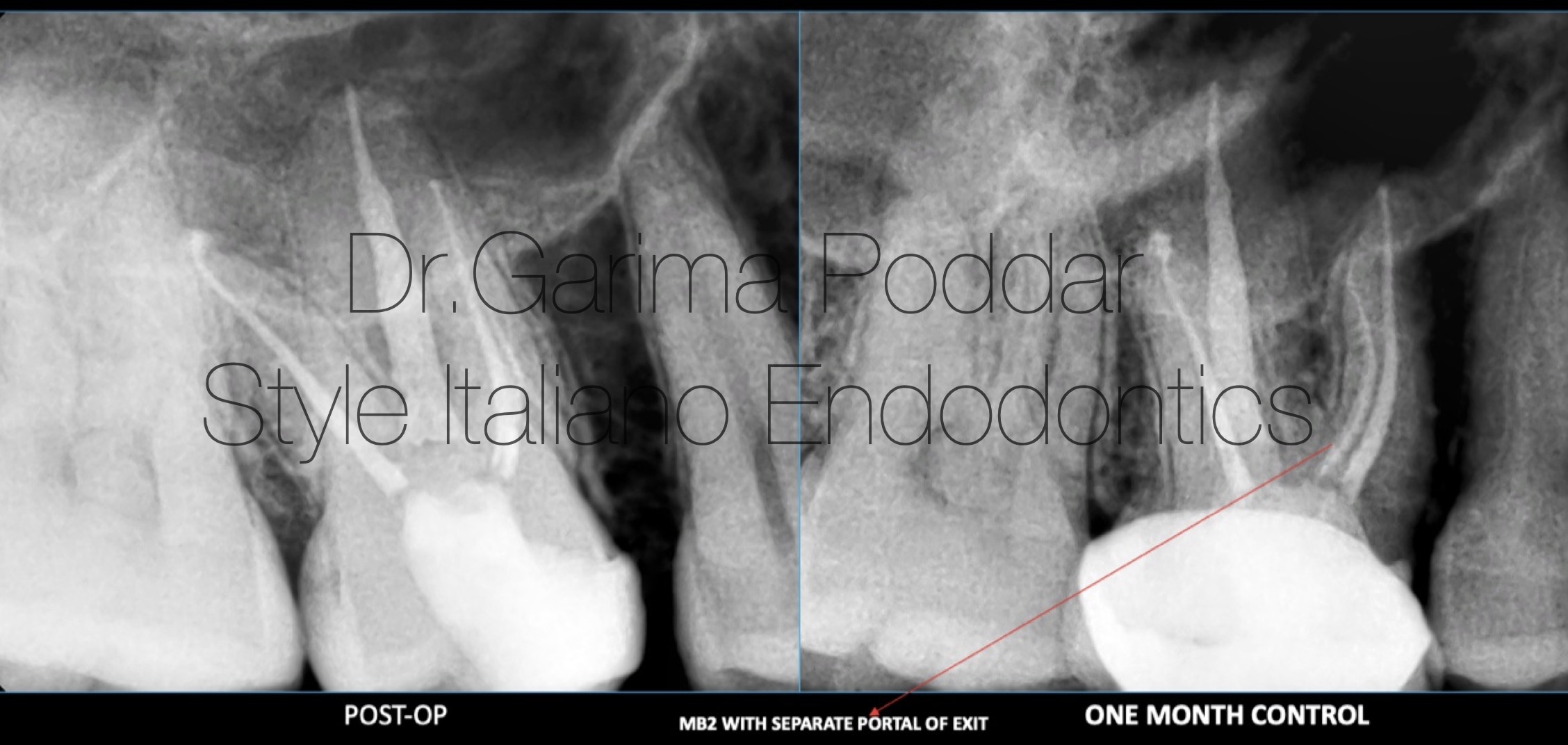
Fig. 9
Obturation protocol-
Canals were obturated with single cones and bioceramic sealer ( Ceraseal- Meta biomed, Korea).
Post endodontic restoration-
Access cavity was restored using bulk fill flowable and warm bulk fill packable composites.
Case was referred back to referring dentist, who delivered a porcelain fused to metal crown for tooth number 16.
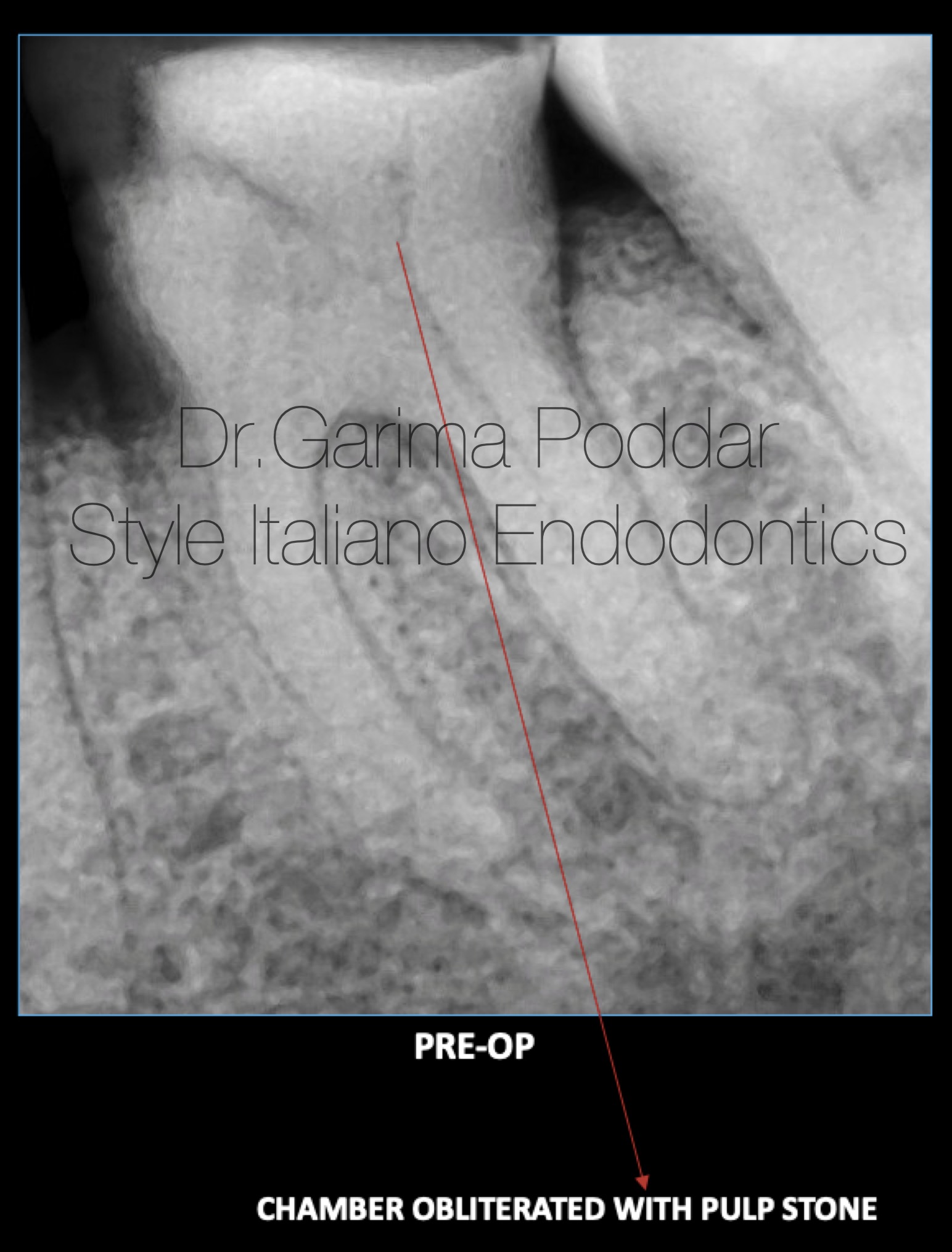
Fig. 10
Case report 3-
A 66 year old female reported to our hospital with pain in mandibular left posterior region.
Patient complaint of pain extending till her left ear.
Clinical evaluation revealed deep proximal caries in tooth number 36 which was tender to percussion.
Radiographic examination-
- Deep mesio-proximal decay, approaching pulp, in relation with tooth number 36 could be appreciated on the radiograph.
- The coronal pulp chamber appeared covered with a radio-opaque mass in 36, suggestive of a pulp stone. The outline of the stone appeared attached with the dentine walls of the tooth.
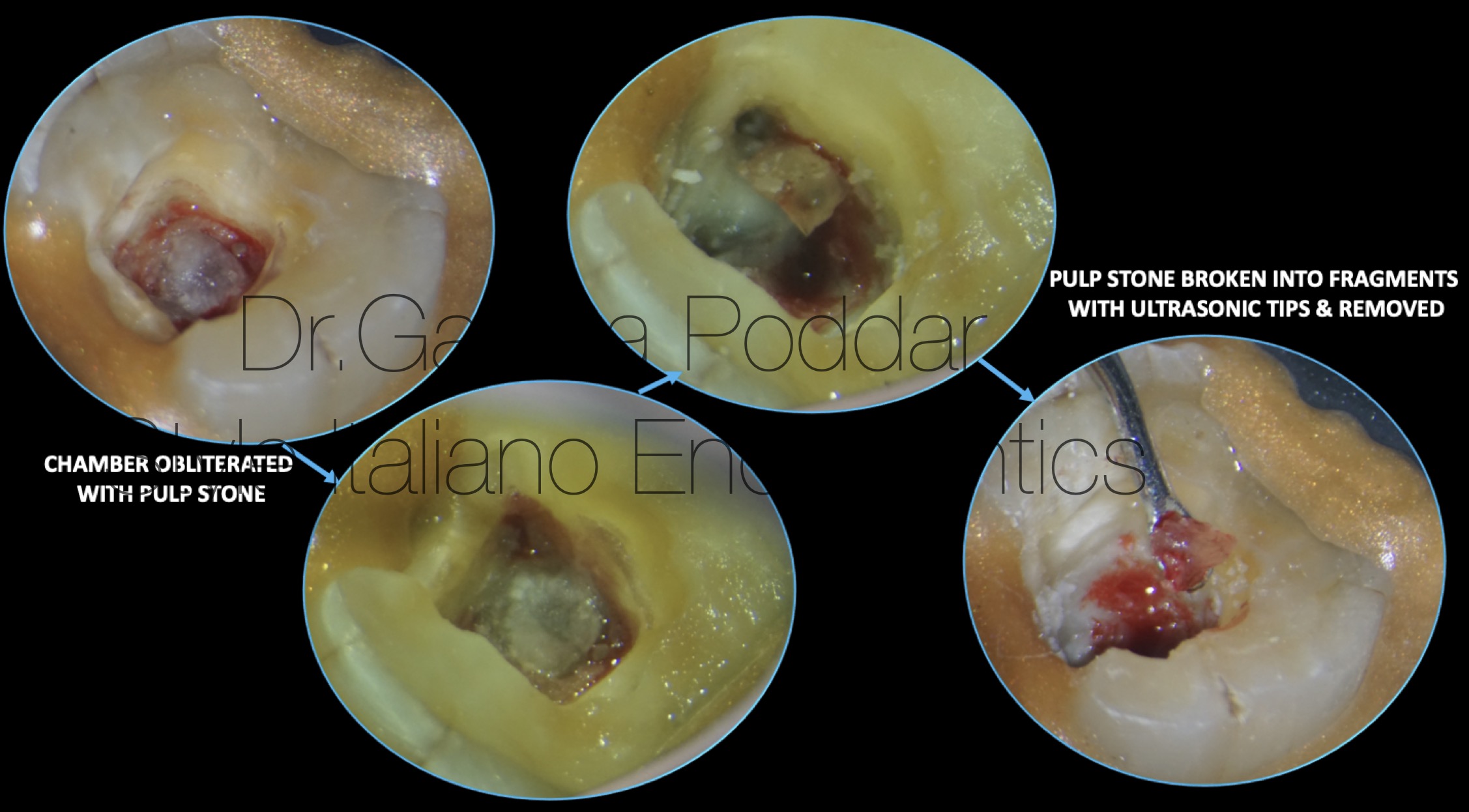
Fig. 11
Local anesthesia was administered.
Rubber dam isolation was done, followed by which, access preparation was done.
The mesio-proximal wall was built up using liquid dam, to get satisfactory, water-tight isolation.
A big pulp stone could be seen covering the floor of the access cavity.
Ultrasonics was used to detach this big mass from the walls, and to break into two piece, and then removed.
For this purpose, tip numbers – E12D and E5D were used.
With the help of ultrasonics, removal of the stone was possible in a conservative manner, without losing substantial amount of dentin of the walls of the access cavity.
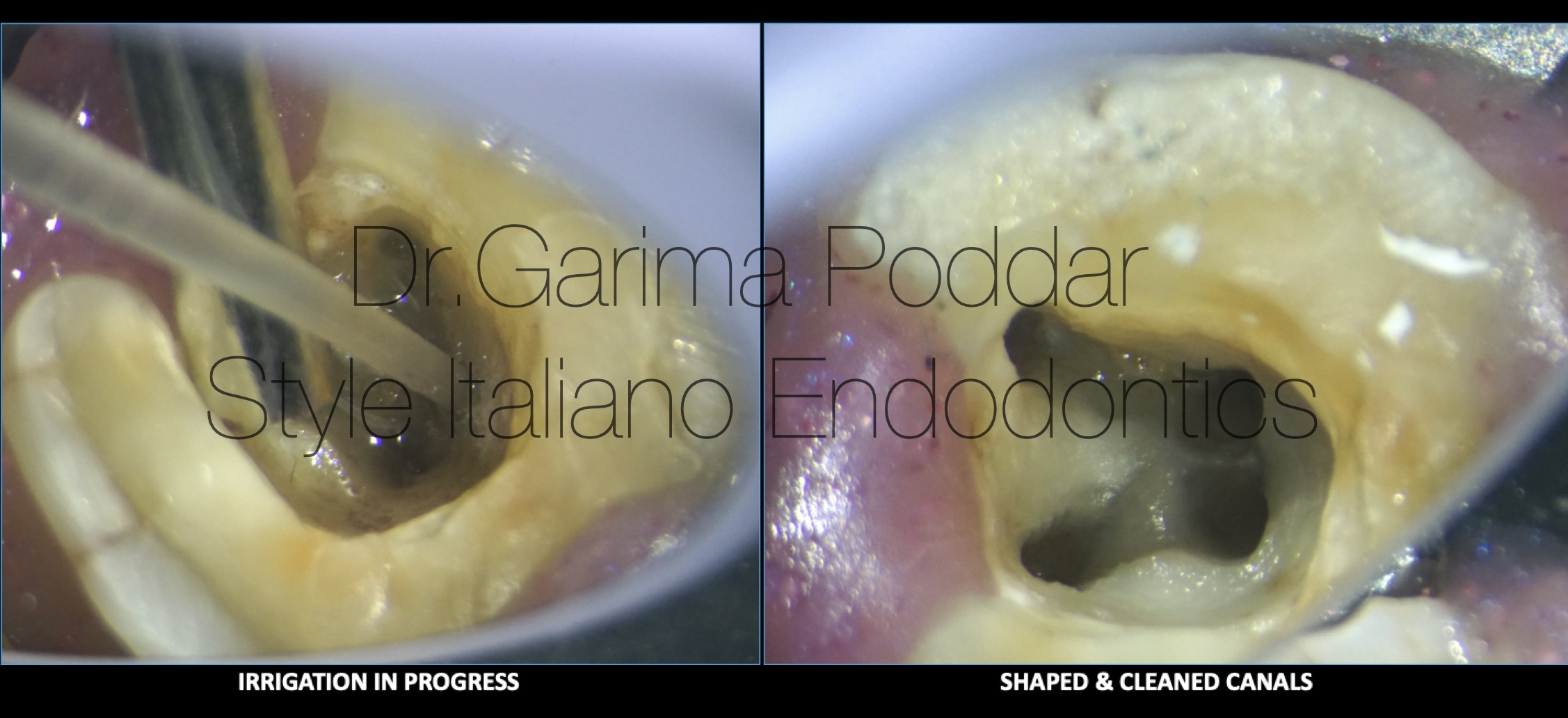
Fig. 12
Once the pulp stone was removed, the canal orifices could be visualized clearly which made the shaping, irrigation and obturation protocols to be performed without any hinderance.
Shaping protocol-
Canals were pre-flared till coronal third, with one flare files (Micromega, France) size 25-09%.
6 and 8 number K files were used to negotiate the canals till working length.
While shaping thinned out canals with steep curvature, recapitulation and irrigation play an important role.
Glide path was then prepared with one G files and shaping was done with 2 shape files (Micromega, France).
Irrigation protocol-
5.25% sodium hypochlorite, distilled water and 17% EDTA were used for thorough irrigation and the solutions were ultrasonically activated.
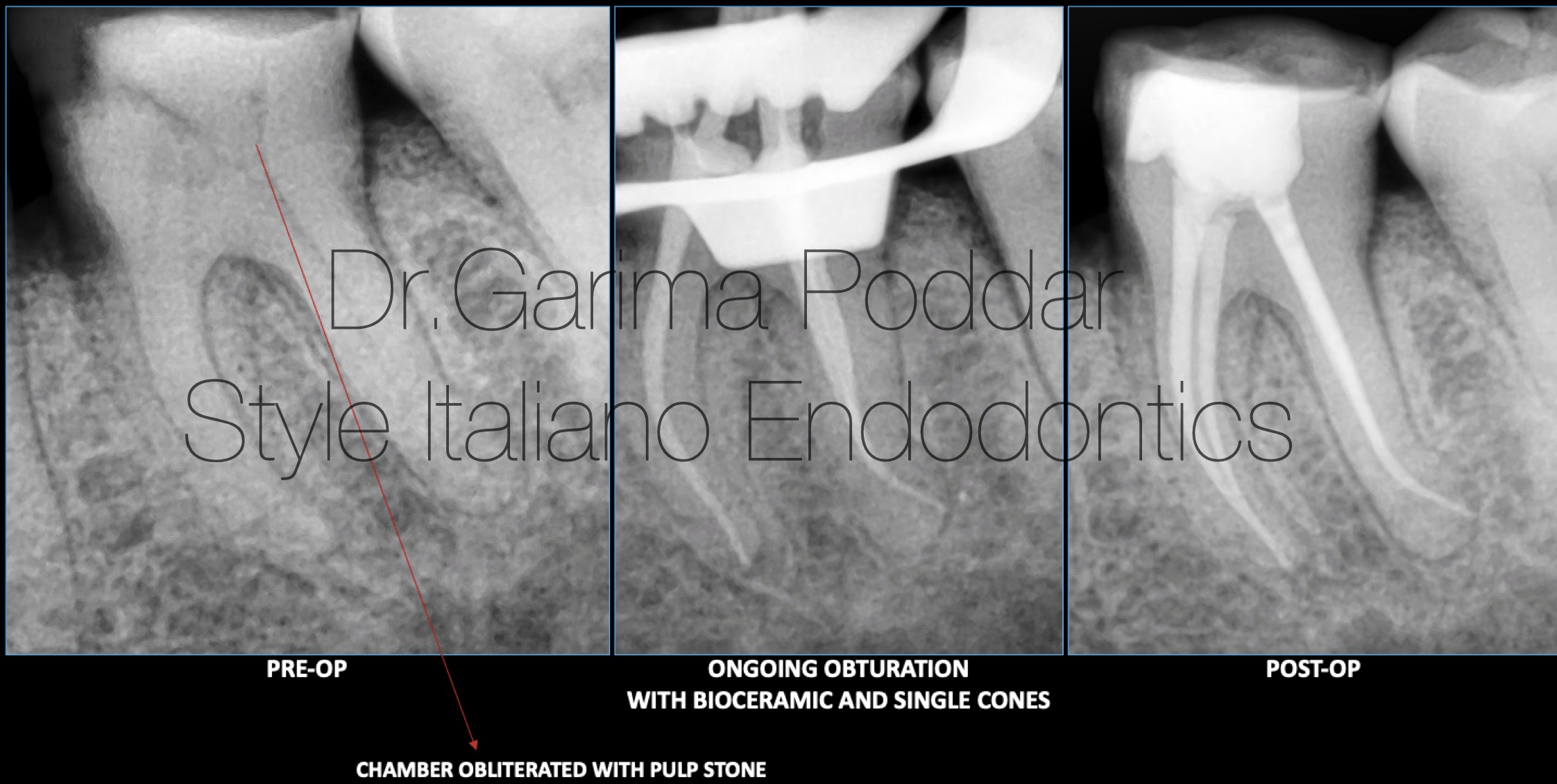
Fig. 13
Obturation protocol-
Master cones were selected for all the canals and tug back was determined.
The technique employed for obturation was single cone with bioceramic sealer ( Ceraseal- Meta biomed, Korea).
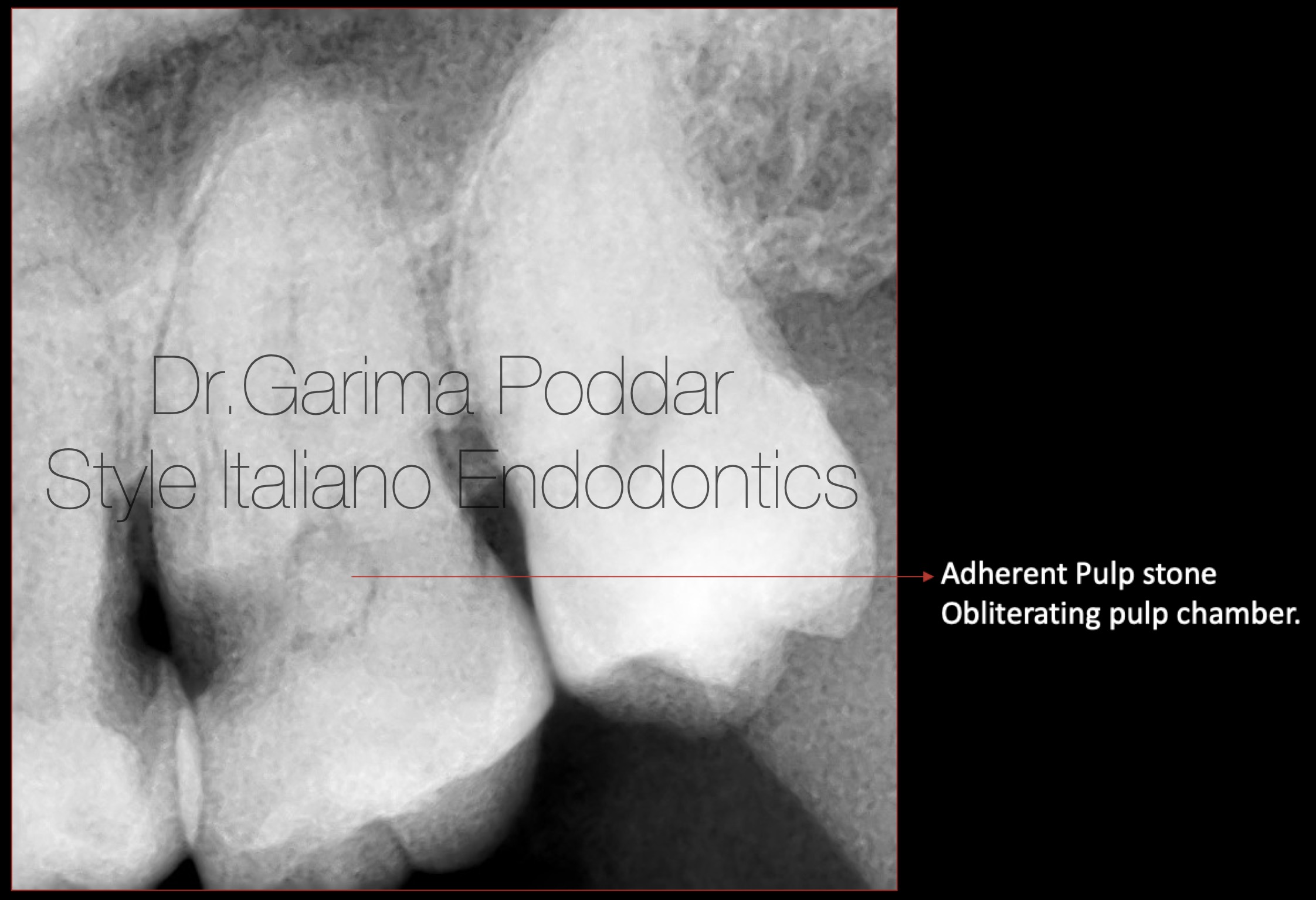
Fig. 14
Case report 4-
A 57 year old male patient reported with pain in maxillary left posterior region. He complaint of onset of pain since last 4-5 days of visiting our centre. The pain was continuous in nature.
Clinical evaluation-
Tooth number 27 was tender to percussion. Caries was observed interproximally, the extent of which was decided to be examined with the help of a pre-operative radiograph.
Radiographic examination-
- Deep mesio-proximal caries was observed in relation with tooth number 27.
- Caries was also noted disto-proximally with respect to tooth number 26. It’s extent was limited to dentin.
- The entire pulp chamber was seen to be obliterated with radio-opaque pulp stone.
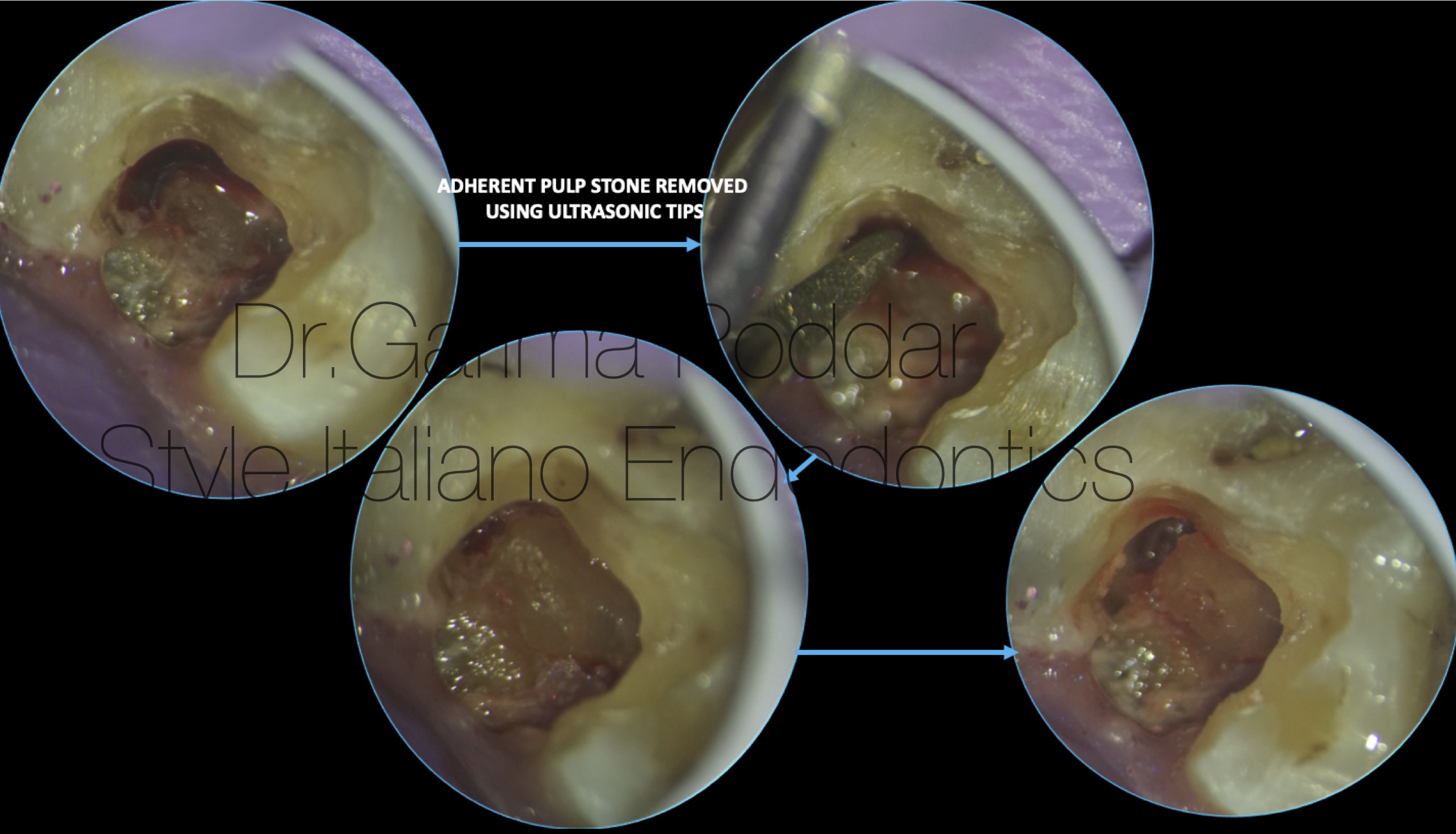
Fig. 15
Local anesthesia was administered, and tooth was isolated with rubber dam.
Ultrasonic tips number E5D (Woodpecker, China) was used to modify and enlarge the canal walls to reveal the stone.
Since water source is switched off while using ultrasonics, irrigation of the chamber after each usage of ultrasonics, helps in clearing out the debris and increases the visibility of the structures well.
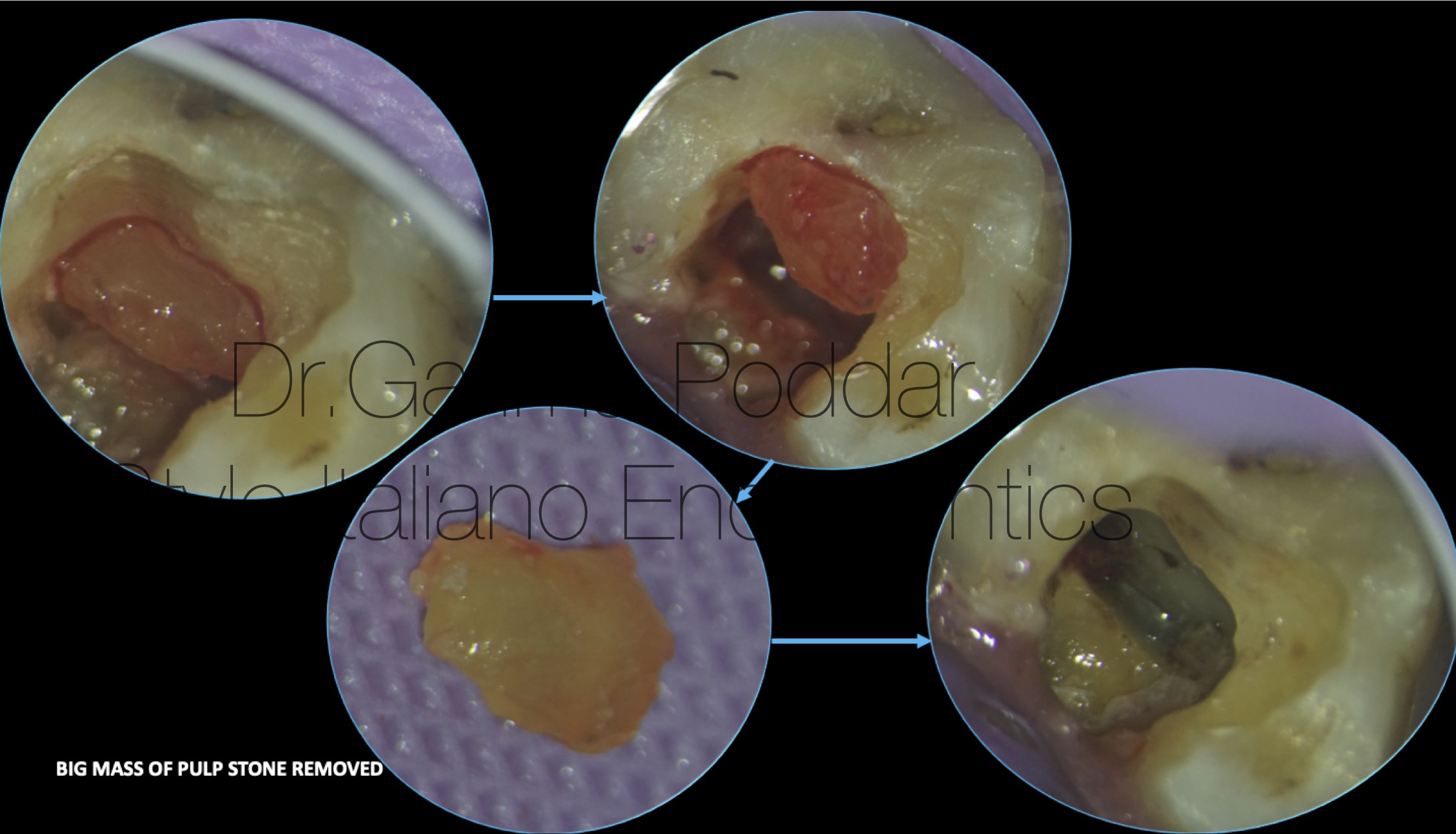
Fig. 16
The pulp stone was of adherent type, and could be loosened effectively with the use of ultrasonics.
The large calcified mass was then removed with ease from the pulp chamber.
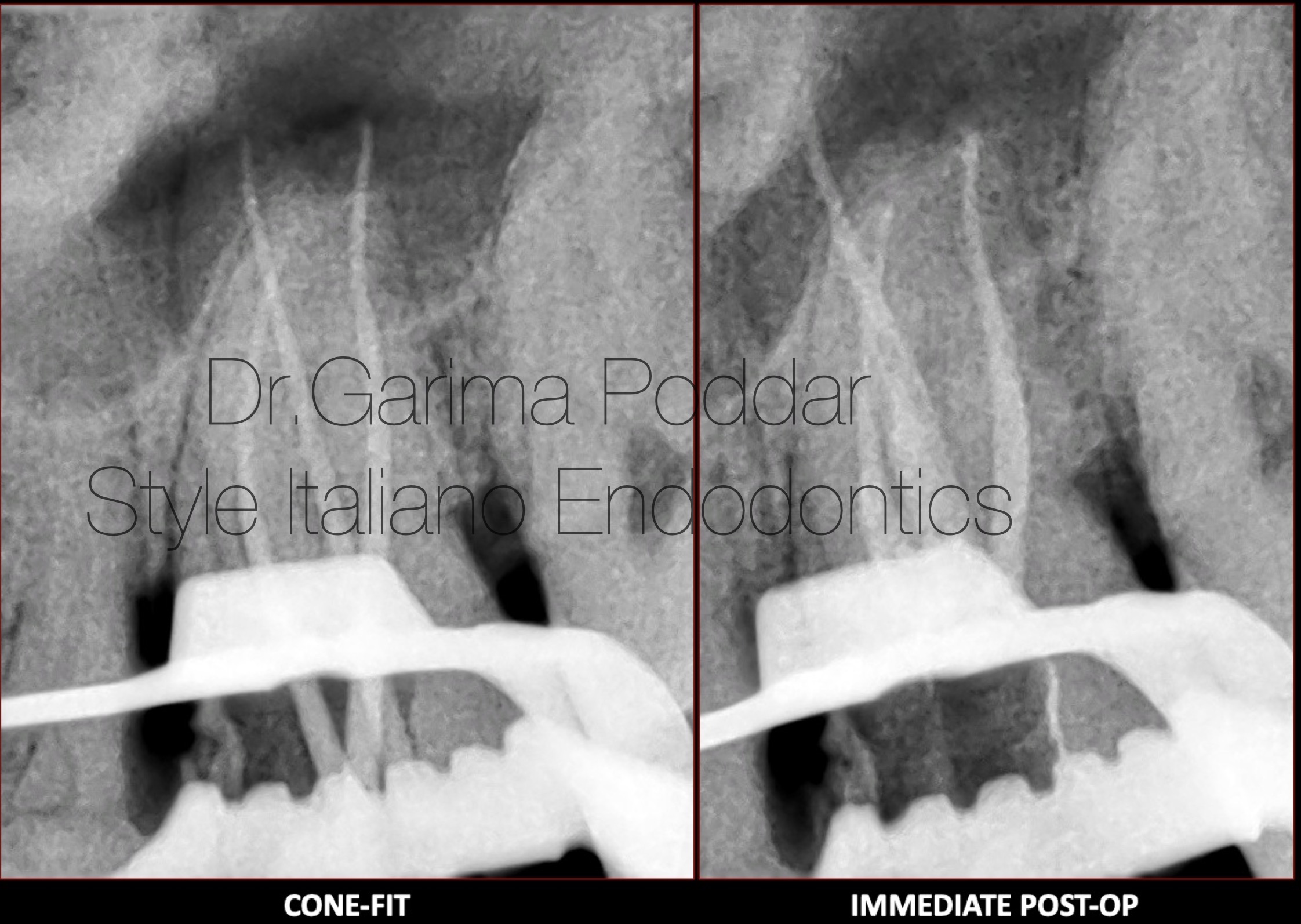
Fig. 17
Shaping protocol-
Coronal flaring was done using one flare files( Micromega, France).
The canals were negotiated with 8 and 10 number K files.
Glidepath was prepared wit one G file ( Micromega, France).
Shaping was done with Hero gold files( Micromega).
Irrigation protocol-
5.25% sodium hypochlorite, distilled water and 17% EDTA were used for thorough irrigation and the solutions were ultrasonically activated.
Obturation protocol-
Cone Fit of gutta percha cones was confirmed.
Warm vertical compaction technique was used to obturate the canals. A resin based sealer- AH plus ( Dentsply Maillefer) was used for this procedure.
Conclusions
Based on various studies as well as clinical observations, it appears that pulp stones are usually physiological manifestations. Their presence might be more frequently seen in case presence of a pathology, but the etiology is not fully clear till date. The presence of a denticle could cause hinderance during an endodontic treatment. Removal of these obstruction causing foci, helps in smooth workflow and better treatment outcomes during a root canal treatment. Developing proper skill to manage a case with pulp stones serves to be helpful to endodontists and general dentists.
Magnification and ultrasonics have been a boon in the procedure of pulp stone removal in a controlled and less aggressive manner.
Bibliography
1.Ten Cate’s Oral Histology (Eighth Edition), 2013
2.Brad W. Neville DDS, Angela C. Chi DMD- Color atlas of oral and maxillofacial diseases, 2019.
3.Goga R, Chandler NP, Oginni AO. Pulp stones: A review. Int Endod J. 2 0 0 8 ; 41( 6 ) : 4 5 7– 4 6 8 .
4.Schaffner, M.; Stich, H.; Lussi, A. Denticles: Dental pulp calculi. Swiss Dent. J. 2014, 124, 416–417
5.Jannati, R.; Afshari, M.; Moosazadeh, M.; Allahgholipour, S.Z.; Eidy, M.; Hajihoseini, M. Prevalence of pulp stones: A systematic review and meta-analysis. J. Evid. Based Med. 2019, 12, 133–139
6.Kronfeld R, Boyle PE. Histopathology of the Teeth and Their Surround- ing Structures. 4th ed. London, UK: Henry Kimpton; 1955.