

Ultrasonics in Endodontics: Part 2
17/06/2016
The Community
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Having reviewed the history of ultrasound and ultrasonic tips in "Ultrasonic in Endodontics: Part 1" (http://styleitaliano.hime.host/ultrasonics-in-endodontics-part-1) in this second part will be highlighted the clinical applications of these tools, that has today become fundamental in almost every phase of the endodontic therapy.
In fact, if they assist the execution of a minimal invasive cavity access, on the other they increase the effectiveness of ultrasound, also allowing the removal of intracanal obstacles and have a key role in the retrograde cavity preparation in endodontic surgery.
The following is a list of the most frequent applications of ultrasound in endodontics, which will be reviewed in detail in the current article:
1. Access refinement, finding calcified canals, and removal of attached pulp stones
2. Removal of intra-canal obstructions (separated instruments, root canal posts, silver points, and fractured metallic posts)
3. Increased action of irrigating solutions
4. Ultrasonic condensation of gutta-percha
5. Placement of mineral trioxide aggregate (MTA)
6. Surgical endodontics: root-end cavity preparation and refinement and placement of root-end obturation material
7. Root canal preparation

Fig. 1
This is the second part of a series of two articles written by Enrico Cassai and Paolo Generali.
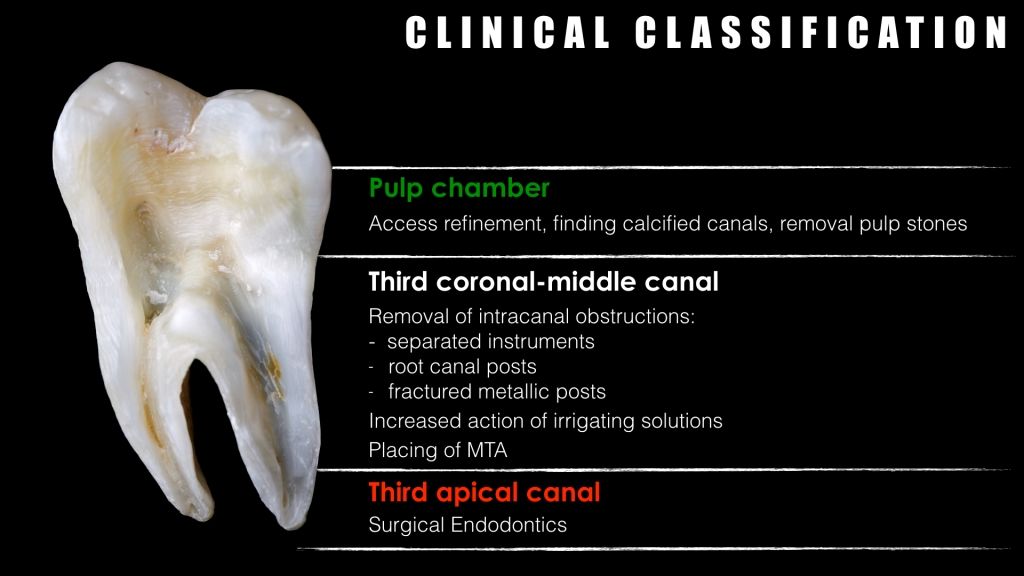
Fig. 2
As for the root canal instruments, also for the use of the ultrasonic instruments, it is appropriate to make a clinical classification according to the tooth section in which they must operate. Therefore the choice of each tip type (active/non active, smooth/milled), the intensity of use, the use with or without water will be in close relationship with the area in which it will have to work.
PULP CHAMBER

Fig. 3
Access Refinement
The current modern endodontic guidelines aim towards the execution of a minimally invasive access cavity allowing one hand the operator a straight access to the canal entrances, but also sparing as much of the tooth structure.
In this respect, the realization of a modern access concept which in the past almost exclusively involved diamond burs on high-speed handpicks and rose-head burs on blue ring micro-motor - consists of a first phase of penetration and coarse enlargement but refinement and extension of the cavity are performed in full with ultrasonic tips.
The main advantages of the ultrasound technique at this stage are the cutting effectiveness and precision towards dentin and visibility allowed by the absence of the head of the micro-motor. This allows a good control without damaging the floor of the pulp chamber, especially in those situations in which this is very sclerotic or almost absent.
The selection of the tip to use depends upon the task to be performed. For the gross removal of dentin in an access preparation, an ultrasonic tip with a length suitable for most access preparations with strong tip that is less prone to fracture and an abrasive grit along half of its length is recommended
For this purpose the tips having to work in an effective way must be set from a maximum to average intensity value, alternating the irrigation phase to that dry to avoid an excessive overheating.
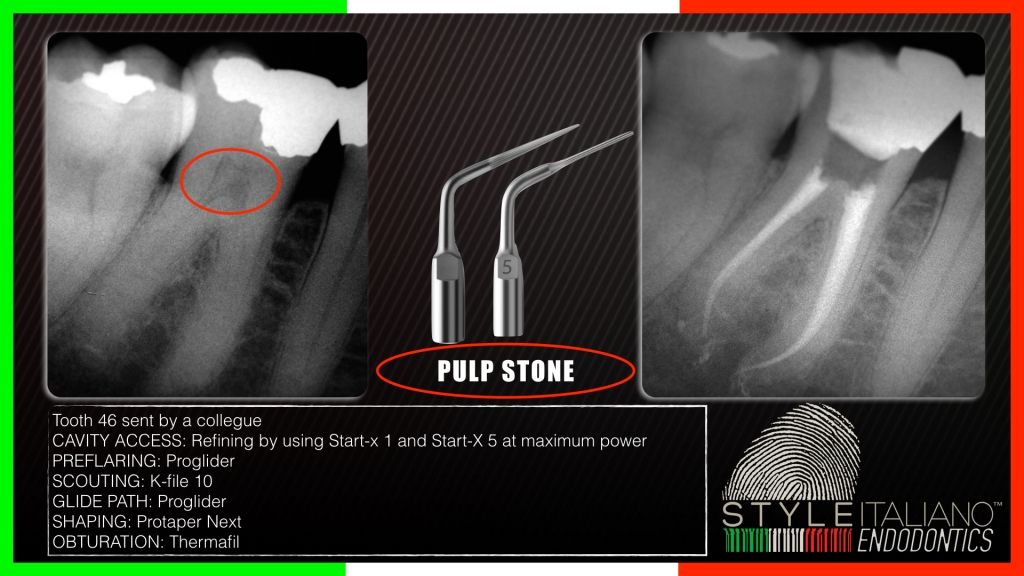
Fig. 4
Pulp Stone
When a pulp stone occludes the entrance to a canal orifice, the ultrasonic tip can be used to carefully smooth the pulp stone away. Use of ultrasonic tips that have a disc-like working part is recommended, due to their ability in erosion of attached pulp stones when used with a brush-like motion without gauging the floor, and are thus good alternatives to ultrasonic tips with a pointy end or a smaller working diameter.
It is very important to use, at this stage, inserts that would not interfere with the floor of the pulp chamber not only to prevent iatrogenic damage (perforations), but also not to miss important references dictated by the floor itself on the position of the root canals.
The tips for this type of operation should be used in an effective way and set from a maximum to average intensity value, alternating the irrigation phase to that dry to avoid an excessive overheating.
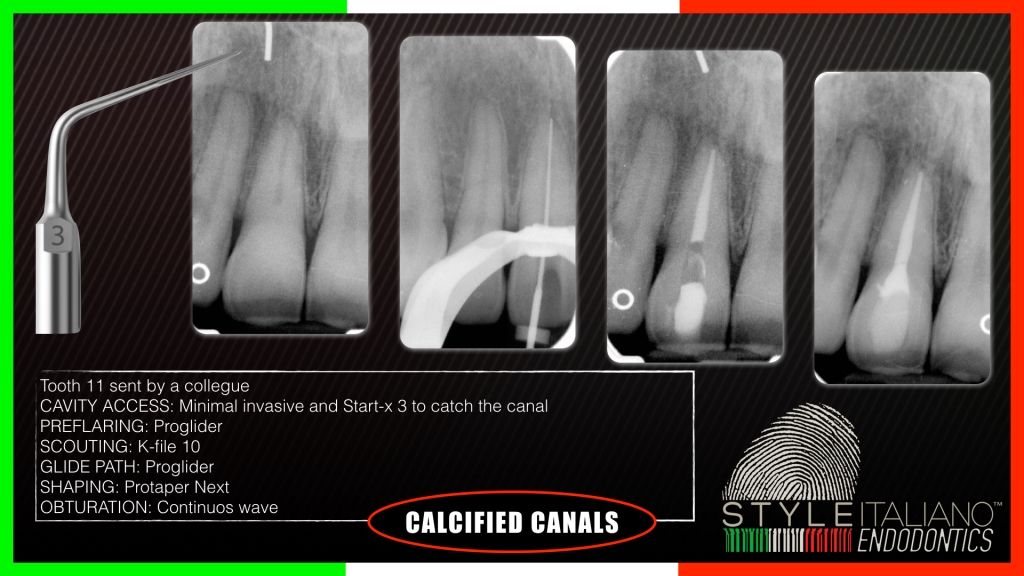
Fig. 5
Calcified Canals
ln all the circumstances in which it is required to explore grooves and isthmuses to find hidden and calcified canals such as MB2 in the maxillary molars or sclerotic canals in traumatic teeth the use of dedicated ultrasonic tips is well recommended. In fact untreated root canal anatomy is likely related to long-term failure of endodontic treatment.
In all this clinical situations roughing bigger tips with a limited diamond-coated extension should be used during the initial phase of removing calcification, interferences, materials, and secondary dentin, as they offer maximum cutting efficiency and enhance control while working in the pulp chamber.
The subsequent phase of finding canal orifices should be carried out with thinner and longer tips that facilitate working in deeper areas while maintaining clear vision and do not create iatrogenic injury such as coronal-middle perforations.
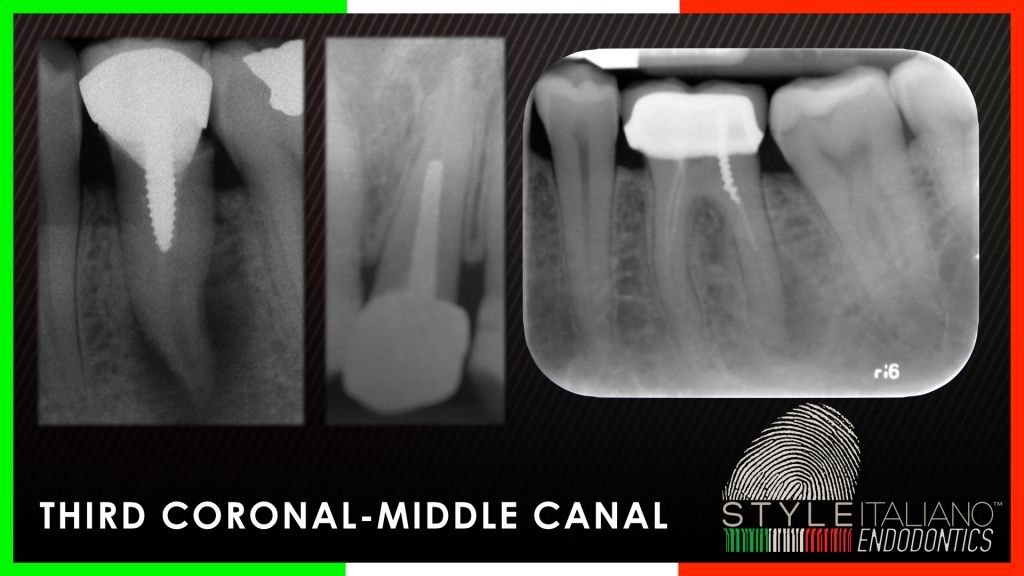
Fig. 6
CORONAL-MIDDLE THIRD OF THE CANAL
Ultrasonic tips are useful to remove foreign objects in the upper and middle portion of the root canal, like posts, hard cement, silver points, separated instruments. A diamond- or abrasive-coated tip can be used for gross dentin removal, to obtain a straight-line access under magnification and coaxial illumination; smooth surface tips are less aggressive and can be used in the deeper portions of the root canal. Ultrasonic tips should be used with a light touch and be kept moving during use, starting with lowest power setting, and increased if needed. Overheating of the tip and of the tooth structure is prevented with intermittent activation of ultrasonics, and with copious air coolant; water can be used to cool the tip and remove debris, but impairs the clear vision of the operating field. Some tips have a water port for cooling, while other dont, being designed to work dry.
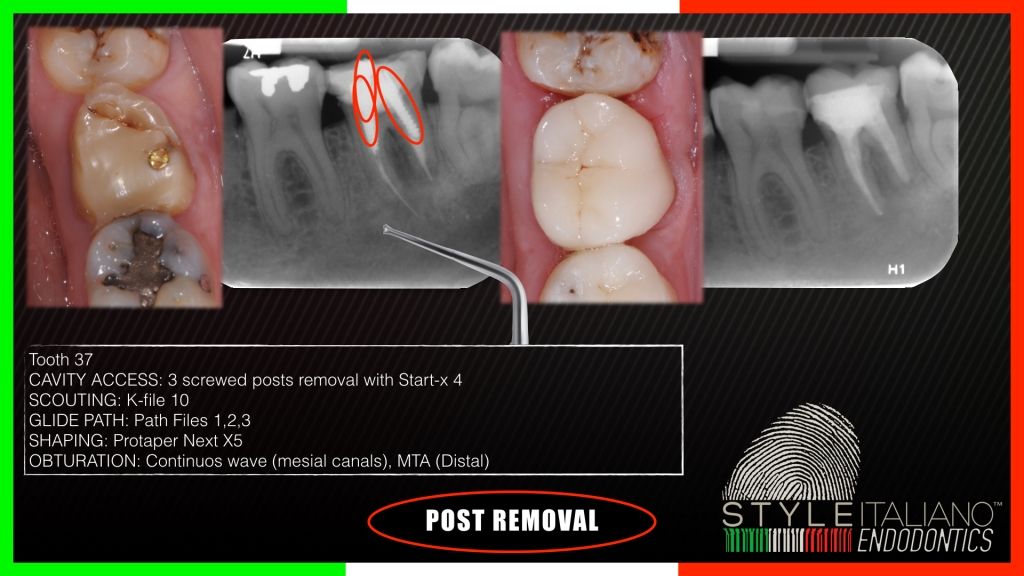
Fig. 7
Post Removal
The efficacy and effectiveness of post removal can be dependent upon several factors, such as the depth of embedment of the post into the root; the type, design, and material of post fabrication; the type of tooth in which the post is cemented; as well as the luting agent used to cement the post. Dedicated tips have been designed for post removal. These are generally shorter and larger than usual, and are intended to be placed directly on the post and moved circumferentially for 5-10 minutes without water, after exposing the head of the post from the material for restoration / cementation with traditional diamond burs. This can loosen the bond between post and cement. If the post cant be removed with this technique, a smaller and longer tip should be used to ditch around post. It has been recommended to reduce the extraradicular portion of the post to the same diameter as the intraradicular portion to reduce the necessary tension to remove it.As an alternative, a large tip can be used with the so-called indirect technique, making it vibrate a small explorer.
Ultrasonics can break up the structure of brick-hard cements, making their removal easier.
The tip should not be too thin, because small-diameter ultrasonic instruments are weak and more predisposed to breakage, especially when they are used for a long time on a resistant material. On the other hand, the tip should not be too large, because it must be kept in intimate contact with the post when it is moved counterclock- wise around the post. Usually, the ultrasonic unit is set to the maximum power level.

Fig. 8
Fiber Post
Fiber post can be disrupted using ultrasonic tips. This topic has extensively been treated in this article by Riccardo Tonini: http://styleitaliano.hime.host/fiber-post-removal-tips-tricks-rules

Fig. 9
Silver Points and Separated Files
Silver tips were used as a filling material some time ago; their removal can be easy when a portion of the tip is reachable by a dedicated plier, named Stieglitz forceps, but can be very demanding when deeply buried in the canal. A thin ultrasonic tip can be helpful for silver point removal, but we must keep in mind that silver points are very fragile, so the ultrasound tip should be used at very low power, with light pressure and should work more on dentin than on the silver point itself. The elimination of broken instruments can be accomplished with a similar technique. First of all, the broken file must be exposed to allow a thin ultrasonic tip to work around the file, eventually vibrating it out. Tips made of a new alloy, Titanium-Niobium, have recently been marketed for retrieval of broken instruments.
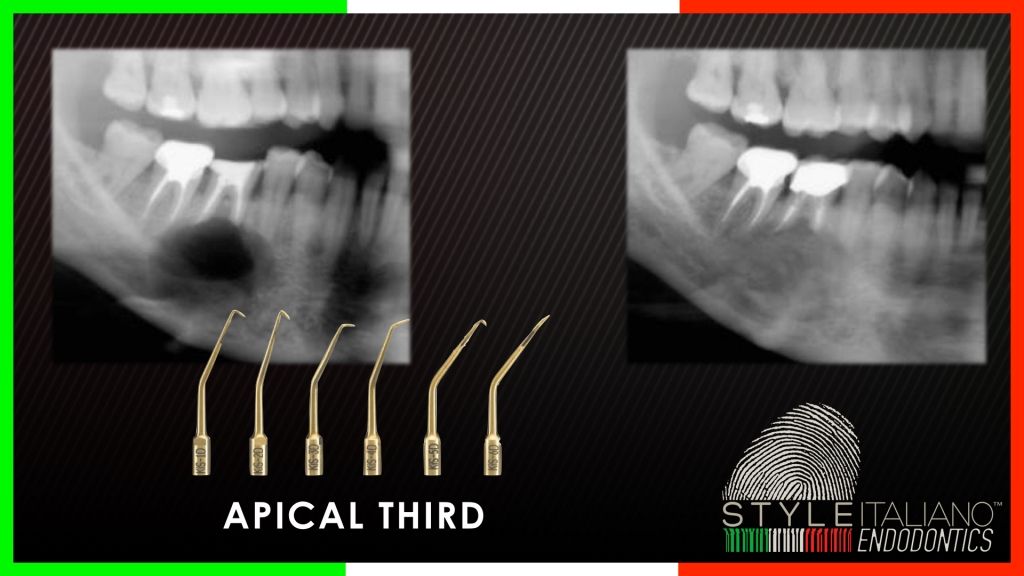
Fig. 10
APICAL THIRD OF THE CANAL
In the apical portion of the canal, dedicated tips should be used. Besides the Titanium-Niobium tips cited above, titanium alloys are often used for this application, and the tips are smooth, non-coated. These tips can also be bended; these must be used at low power setting and with very light pressure. An excessive force or power can easily fracture these instruments. These tips can be used for any of the purposes listed above and also, at minimal power, for vibrating MTA cement. This task can be also accomplished with the indirect technique, applying a bigger ultrasonic tip to an endodontic plugger.
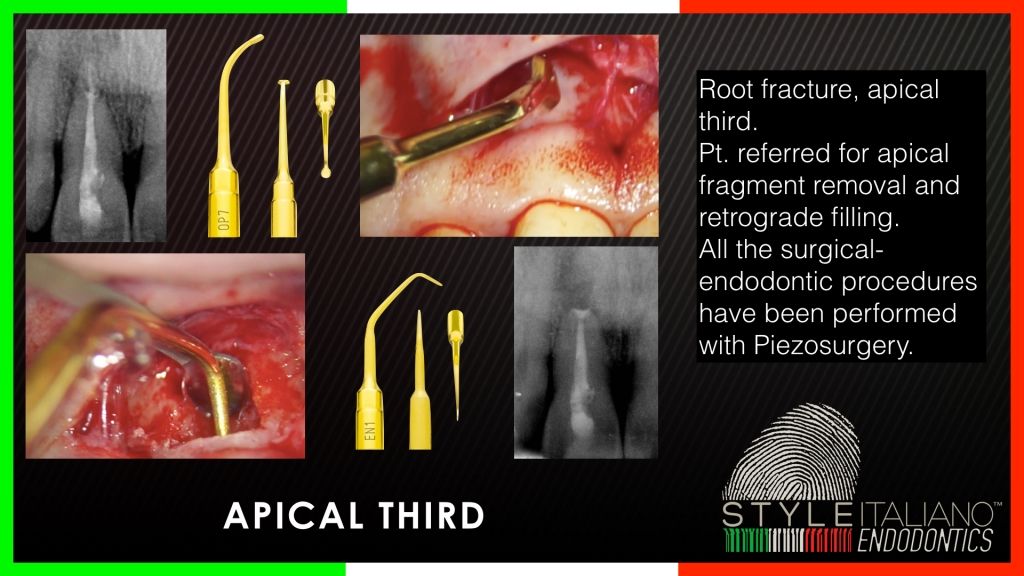
Fig. 11
Ultrasonic devices have changed the practice of surgical endodontics. Dedicated tips for apical retropreparation allow the access for 3 mm or more in the apical portion of the canal, including histmuses, and deep placement of filling material in the canal, thus enhancing the predictability of the procedure. Powerful endodontic devices, such as Piezosurgery®, can be used for bone access and for retropreparation.
Conclusions
Nowadays, the ultrasonic technique has become an needful aid in everyday endodontic practice and its use in combination with magnification and a coaxial light source made situations that until recently were difficult, simpler and more predictable for all.
Once again, it is the diagnosis that plays a key role in understanding what type of ultrasonic tip to use, at what level, how and especially if the operator has the means, the techniques and knowledge to manage certain clinical cases.
Also, vice versa, a simple case can become incredibly difficult when an inaccurate diagnosis or an inappropriate choice of instruments have been done. Ultrasonic tips for endodontic use are differen in size, shape and material, and doesn't exist a single tip for all the tasks; so, a series of tips are needed. Compatibility between tips and handpieces can be an issue, and the producer's instruction must be followed to avoid the risk of instrument breakage and other failures. It is wise to start with the lower power setting, and then increase the power if needed. Pressure should be always light. An air blow is enough for avoiding overheating at low power; some tips have also a water port, as water is more effective in cooling the tip, but this reduces visibility. More, vented tips are anecdotically reported as less durable that non-vented types, designed to work dry.
As a matter of fact, visibility of the working tip is the biggest advantage of ultrasonic devices upon rotary instruments; in the former, the power source doesn't impair vision, while in the latter, the head of the handpiece, being on the long axis of the working instrument, can be on the sight line. This great advantage means also that US tips must always be used with good visibility ao the operating field, never trying to use them blindly, since this can be dangerous.
Bibliography
- Plotino G, Pameijer CH, Grand NM, Somma F. Ultrasonics in Endodontics: a review of the literature. J Endod 2007;33:81-95.
- Park E. Ultrasonics in endodontics, Endod Topics 2013;29:125-159
- Glassman G, Kratchman S: Ultrasonic in Endodontics: Luxury or Necessity. Dent Today. 2011 Sep;30(9):114, 116-9.
- Sempira HN, Hartwell GR. Frequency of second mesiobuccal canals in maxillary
molars as determined by use of an operating microscope: a clinical study. J Endod
2000;26:673 4. - Gorduysus MO, Gorduysus M, Friedman S. Operating microscope improves negotiation of second mesiobuccal canals in maxillary molars. J Endod 2001;27:683 6.
- Rampado ME, Tjaderhane L, Friedman S, Hamstra SJ.The benefit of the operating microscope for access cavity preparation by undergraduate students. J Endod 2004;30:8637.
- Lin YH, Mickel AK, Jones JJ, Montagnese TA, Gonzalez AF. Evaluation of cutting efficiency of ultrasonic tips used in orthograde endodontic treatment. J Endod
2006;32:359 61. - Paz E, Satovsky J, Moldauer I. Comparison of the cutting efficiency of two ultrasonic units utilizing two different tips at two different power settings. J Endod 2005;31:8246.
- Ruddle CJ. Nonsurgical endodontic retreatment. J Calif Dent Assoc 2004;32:
474 84. - Johnson WB, Beatty RG. Clinical technique for the removal of the root canal ob- structions. J Am Dent Assoc 1988;117:473 6.
- Hulsmann M. Methods for removing metal obstructions from the root canal. Endod Dent Traumatol 1993;9:22337.
- Fors UGH, Berg JO. Endodontic treatment of root canals obstructed by foreign objects. Int Endod J 1986;19:210.
- Hulsmann M. The removal of silver cones using different techniques. Int Endod J
1990;23:298 303. - Sprigs K, Gettleman B, Messer H. Evaluation of a new method for silver points
removal. J Endod 1990;16:335 8. - Gettleman BH, Springs KA, Messer HH, El Deeb ME. Removal of canal obstructions
with the Endo Extractor. J Endod 1991;17:608 11. - Nehme WB. Elimination of intracanal metallic obstructions by abrasion using an
operational microscope and ultrasonics. J Endod 2001;27:3657. - Ward JR, Parashos P, Messer HH. Evaluation of an ultrasonic technique to remove fractured rotary nickel-titanium endodontic instruments from root canals: clinical cases. J Endod 2003;29:764 7.
- Ruddle CJ. Nonsurgical retreatment. In: Cohen S, Burns RC, eds. Pathways of the
pulp, 8th ed. St Louis: Mosby; 2002:875930. - Ward JR, Parashos P, Messer HH. Evaluation of an ultrasonic technique to remove fractured rotary nickel-titanium endodontic instruments from root canals: an experimental study. J Endod 2003;29:756 63.
- Navarre S, Steiman H. Root-end fracture during retropreparation: a comparison between zirconium nitride-coated and stainless-steel microsurgical ultrasonic instruments. J Endod 2002


