Dens Evaginatus - A case report
12/09/2023
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Dens evaginatus (DE) is a relatively rare developmental anomaly that occurs more often in people of Asian descent than European descent. DE appears as a cusplike elevation of enamel, referred to as a tubercle, and is located in the central groove or on the buccal or lingual cusps of premolars or molars and the palatal or lingual surfaces of anterior teeth.DE is now the most common term, but many other terms have been used such as interstitial cusp, central cusp, supernumerary cusp, occlusal enamel pearl.
This case report is about a 14 years old female patient.
Chief complaint:The left lower premolar was swollen and painful for 3 days.
Present illness: chronic gingivitis. 3 days before, the patient felt pain on the left lower premolar, with swelling of the gingiva. There was not night pain but the patient was unable to chew.
Past history: Respiratory system: No history of respiratory disease.
Infectious history :No history of severe infectious disease.
Allergic history :She was not allergic to penicillin.
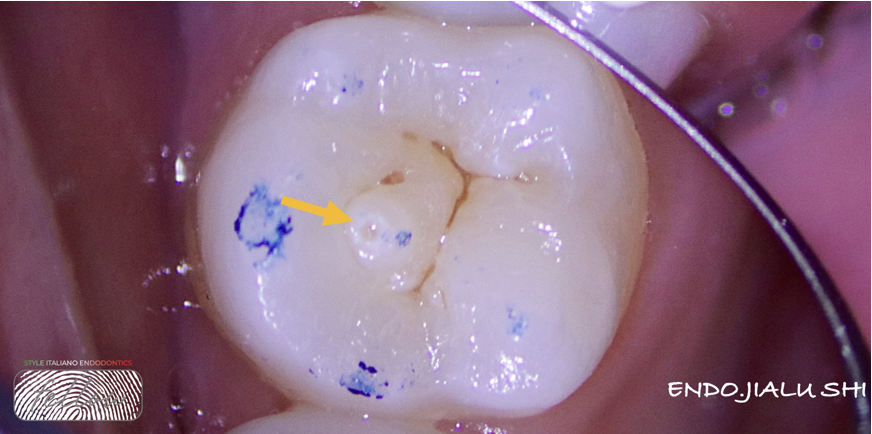
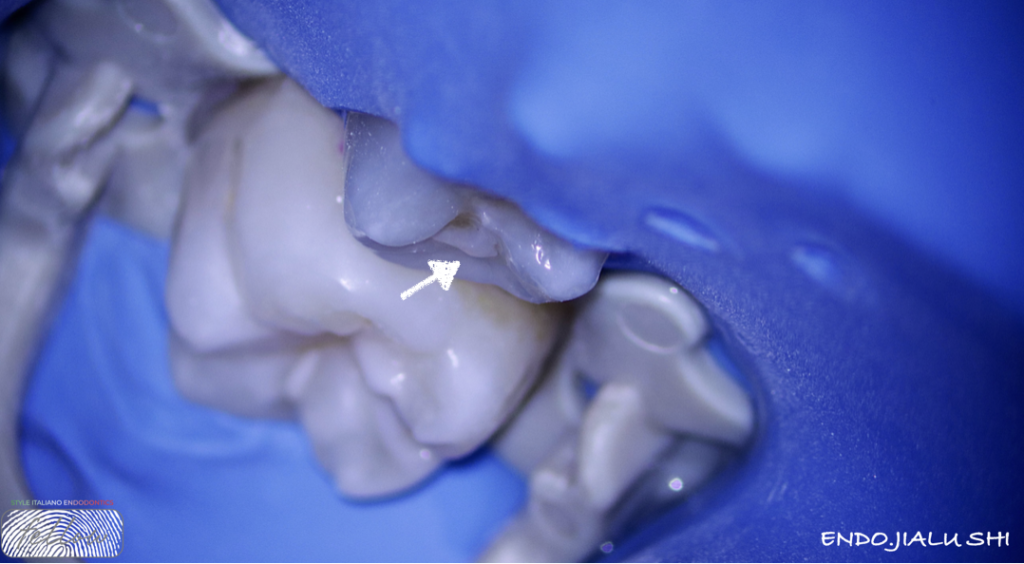
Fig. 1
The Occlusal tubercle (arrow) of the broken deformity can be seen on the occlusal surface。The tooth 3.5 was not responsive to cold testing and was tender to pressure. Not checked deep periodontal pocketing. No excessive mobility and fluctuant buccal swelling.

Fig. 2
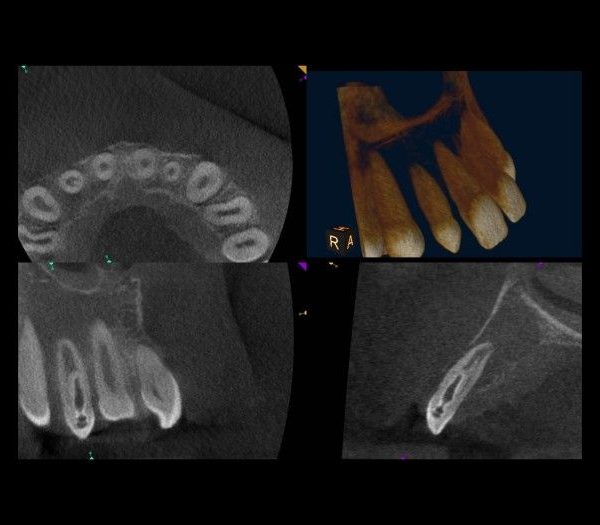
Careful examination of pre-operative CBCT to determine the degree of difficulty:
Pre-operative cbct
35#
CBCT shows that the root apex of the tooth was fully developed
Radiolucency around the root apex
The diagnosis of 35 Chronic apical periodontitis,Dens evaginatus

Fig. 3
the patient is only 14 years old, and we need to retain his natural teeth by Apexification
The patient was informed regarding the guarded overall prognosis of this tooth.
Adequate local anaesthesia was administered and rubber dam was placed.
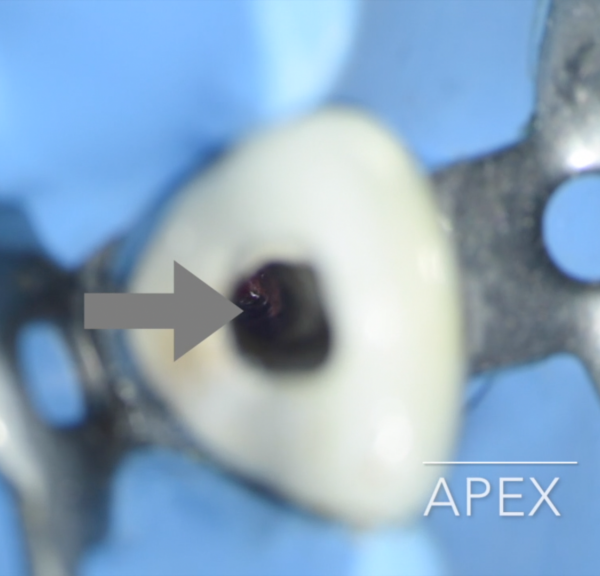
After preparation of the access cavity, a large number of Wells purulent blood from the root canal.
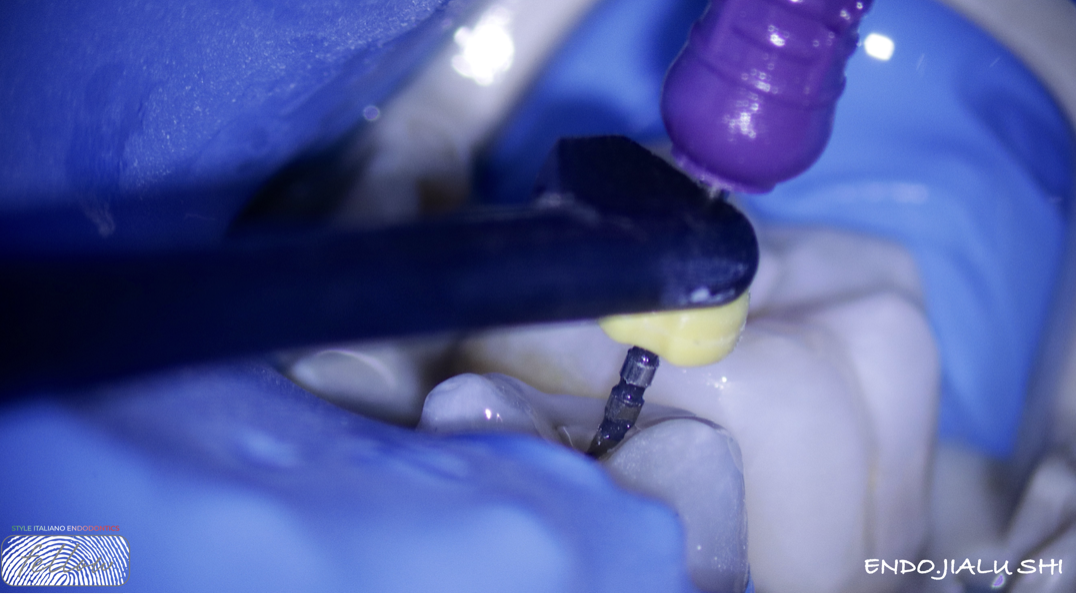
Fig. 4
Working length determination

Fig. 5
Preparation the root canal by rotary files (#30 Taper 4%) and irrigation by 3% NaOCl(40 ml)activated with a sonic system.
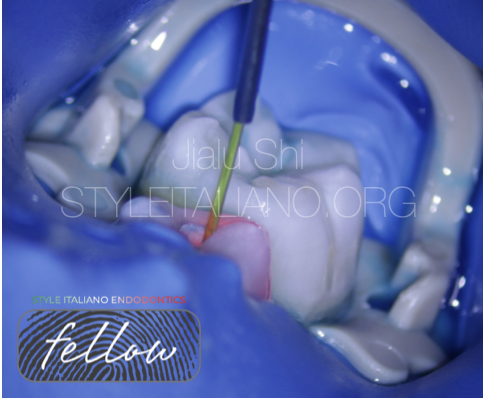
Fig. 6
Root canal disinfection with the PDT(Photodynamic Technology

Fig. 7
Irrigation was done with 40 mL of NaOCl, activated by a sonic device.
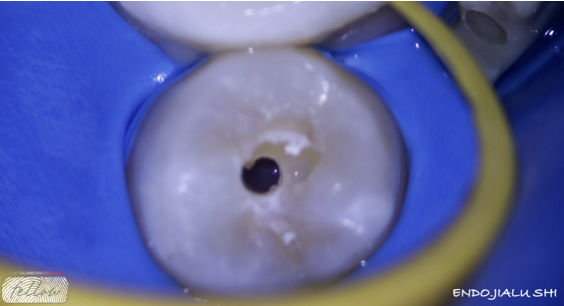
Fig. 8
The inside of the root canal was observed under a microscope at 20 × magnification, no traces of pulp and pus residues in root canal.
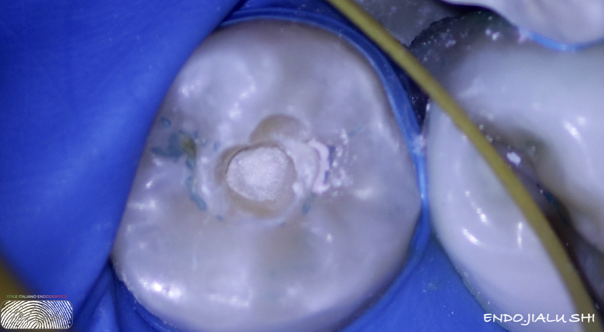
Fig. 9
Finished the root canal filling by bio ceramic putty that was inserted into the root canal using the NITI-File rotated at 150rpm in the opposite direction and the working length was reduced by 3mm
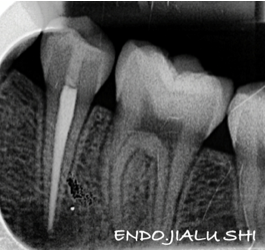
Fig. 10
post-operative x-ray
Conclusions
Treatment options for DE have included intermittent grinding of tubercles before any pulpal involvement, tubercle protection with composite resin, coronal pulpotomies, apexification combined with root canal filling, root canal therapy in teeth with mature roots, apical surgery, and extraction in cases of orthodontic treatment.Whether the root apex is fully developed or not is an important factor in the selection of treatment options.
Bibliography
1,Jung-Wei Chen, DDS, MS, PhD; George T.-J. Huang, DDS, MSD, DSc; Leif K. Bakland, DDS(2020,May Dens Evaginatus: Current treatment options.
2, Eitan Dankner, DMD, MSc, a Doron Harari, DMD, b and Ilan Rotstein, CD, Jerusalem, Israel(1996 Apr) Dens evaginatus of anterior teeth Literature review and radiographic survey of 15,000 teeth
3,Lerdrungroj K, Banomyong D, Songtrakul K, Porkaew P, Nakornchai S(2023 Jul)Current Management of Dens Evaginatus Teeth Based on Pulpal Diagnosis
4, Uyeno DS, Lugo A(1996 Sep-Oct)Dens evaginatus: a review.
5.Ponnambalam Y, Love RM(2006 Jun)Dens evaginatus: case reports and review of the literature.
6.Levitan ME, Himel VT. Dens evaginatus: literature review, pathophysiology, and comprehensive treatment regimen. J Endod. 2006;32(1):1–9.