Conservative Retreatment Challenges and Solutions
23/03/2026
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Endodontic Retreatment is primarily a biologic procedure aimed at eliminating persistent or secondary intraradicular infection while preserving tooth structure. Failure is always associated with residual infection , missed anatomy and inadequate chemo-mechanical debridement. ( Nair, 2006; Siqueira & Rocas, 2014). By Regaining Access to inadequately debrided anatomical complexities we are enabled to renegotiate and target the source of persistent infection ( Gomes et al.,2015) as well as Using Sodium Hypochlorite, EDTA and activation systems is essential for success. ( plotino et al., 2016)

Fig. 1
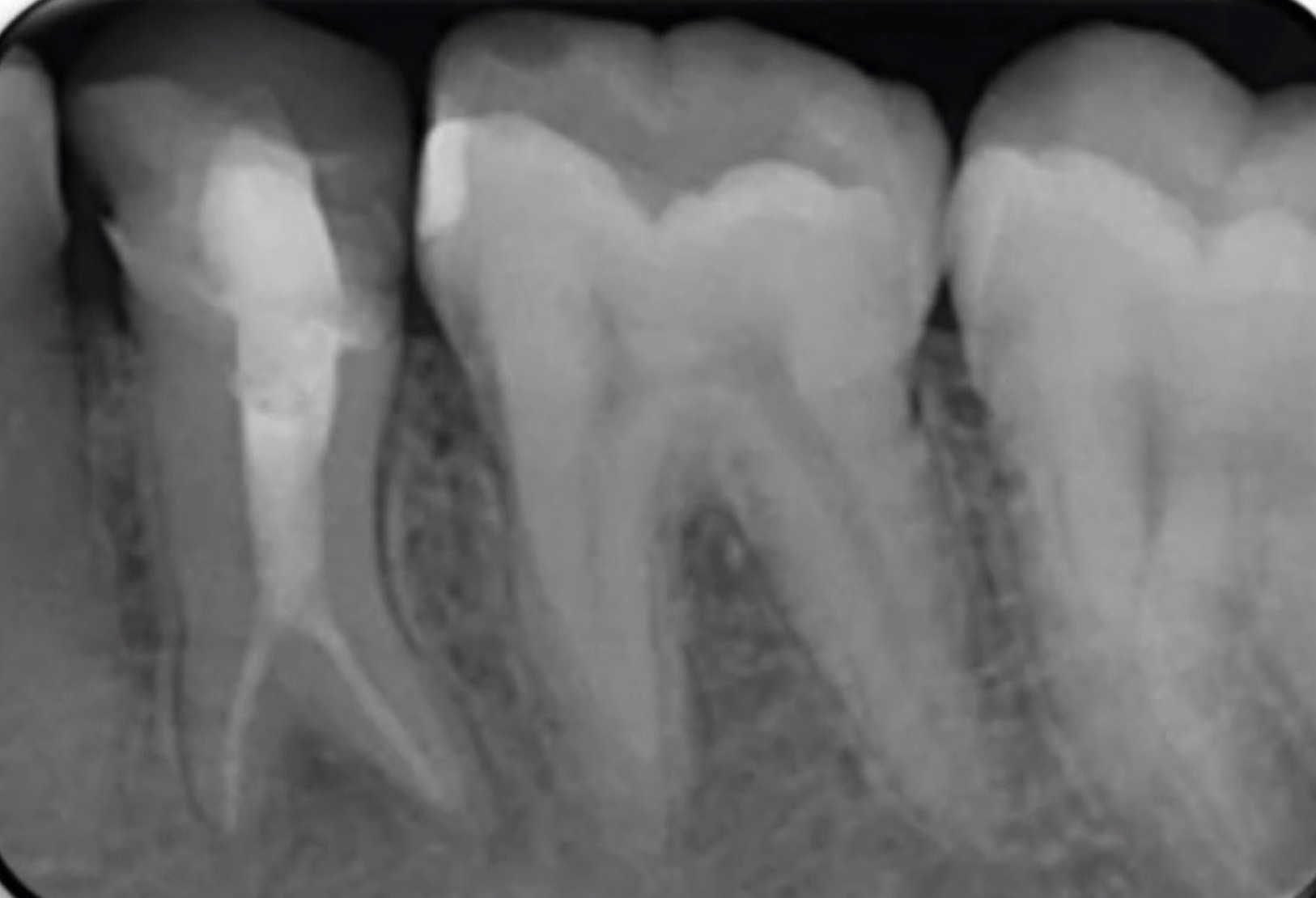
Case: Referred 25 years old patient came to our clinic with pain on Biting related to lower right first molar , stating a previous endodontic treatment done a year ago with pain on biting ever since. A Periapical Radiographic Xray ( fig1 ) showed obvious widening in lamina dura around mesial and distal root and mild abscesses related to mesial and distal roots .
Two Broken files are also noticed:
One in Mesiobuccal Canal (Middle zone )
And One in Distal Canal (apical zone )
As well as over obturation from ML canal
Cone Beam CT was requested to further locate the broken files

Fig. 2
CBCT Sagittal cuts shows a more defined abscess and precise location of the broken files. First file separated in mesio buccal canal above the curve , and the second file separated in Distal Canal almost at the end of apical foramen and the low contrast predicts it to be a 10 or 15 k file.
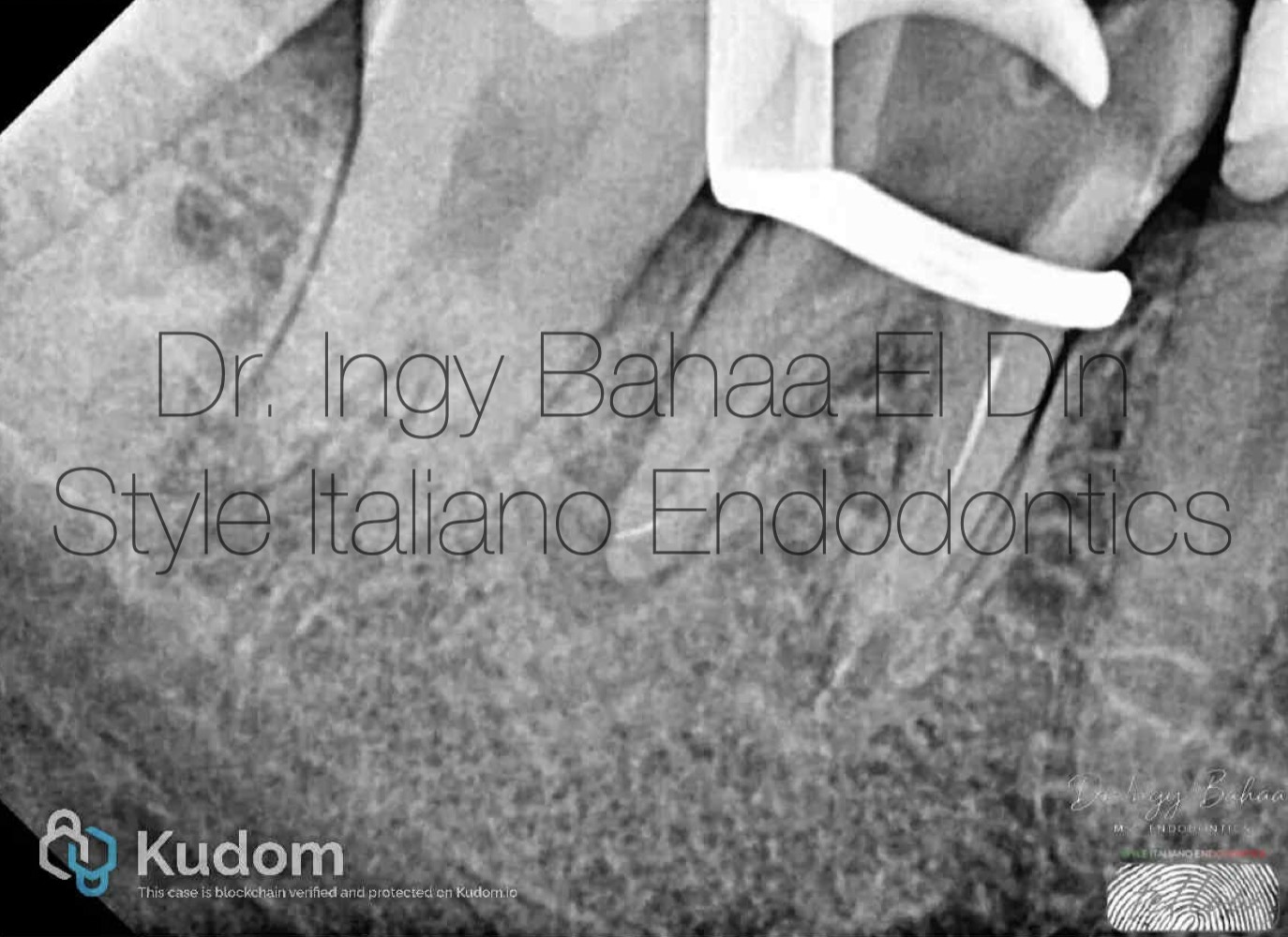
Fig. 3
Removal of old GP was done sequentially using Retreatment rotary files and copious irrigation using NAOCL 5.25% , after achieving success in removing all remnants we have a more clear vision of the broken files

Fig. 4
Successful dis-engagement of the separated instrument was achieved. Using E9 Ultrasonic tip from Eighteeth; Troughing around the visible portion of the file in a half turn motion directed towards the inner wall and without touching the file to avoid secondary fracture. with regards to cooling between troughing to avoid over heating of dentin.

Fig. 5
Once file starts dancing, we trough with an open copious coolant activated to push out the file
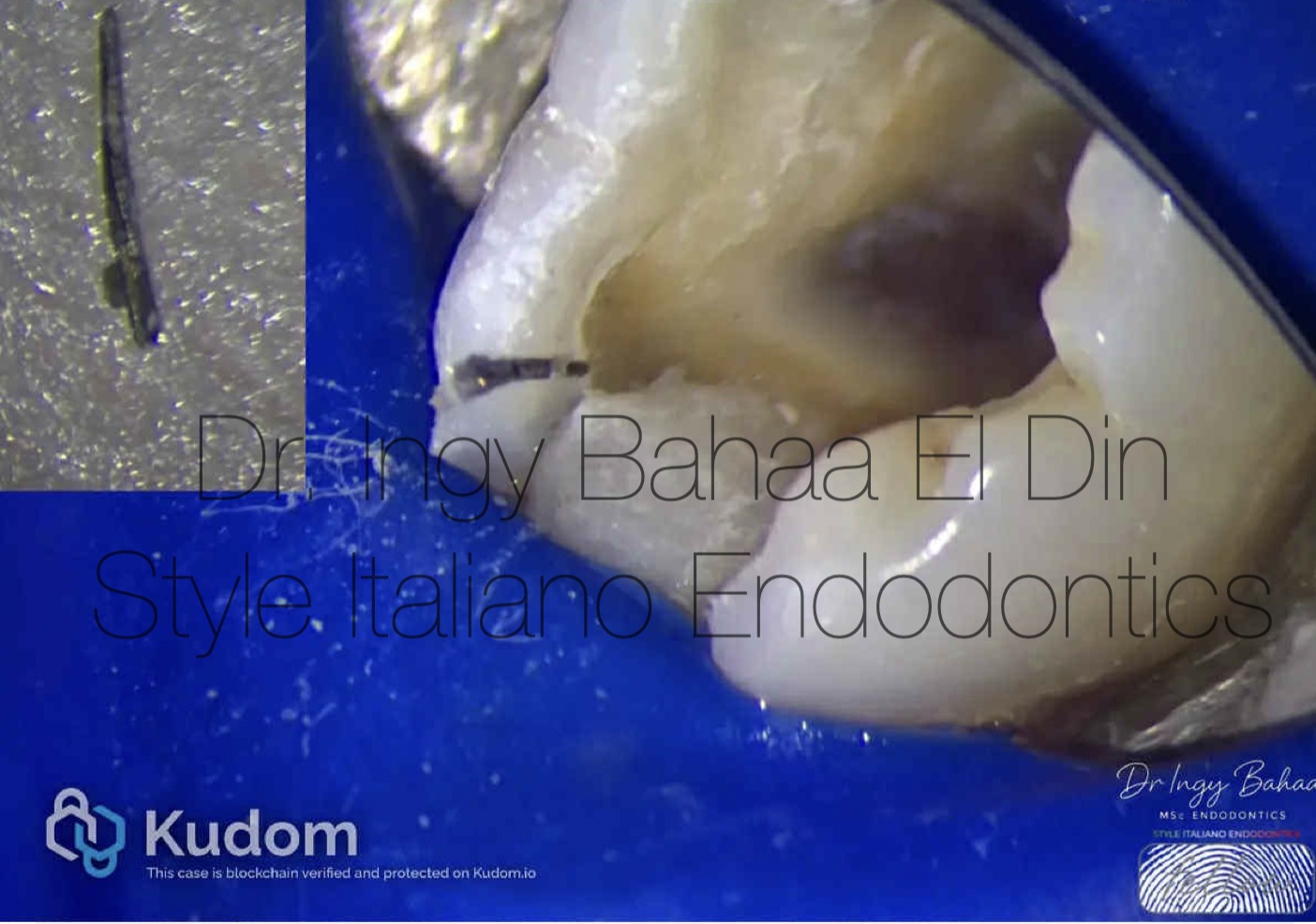
Fig. 6
And after flushing with ultrasonic and coolant activation its out.

Fig. 7
Xray confirmation full removal of file with minimal dentin loss

Fig. 8
Moving on to separated instrument number two, we had two challenges Number 1 : Risk of extrusion due to file engagement apically. Number 2 : Separation of file is beyond the curve which doesn’t give much visibility for troughing , Thus: Conservative Bypass was decided. With a Pre-bent D finder file size 10 in picking motion, a catch was found. Proceeding with 10 k file in watch-winding motion until patency was achieved

Fig. 9
Master Cone Adjustments

Fig. 10
Immediate Post Operative, Obturation : warm vertical compaction and ideal usage of Bio ceramic Sealer in this case to properly fill in the spaces from the bypass and retrieval procedures.

Fig. 11
Coronal Seal done using Shofu Composite in snow plough technique

Fig. 12
Immediate Post Operative apical and coronal seal.
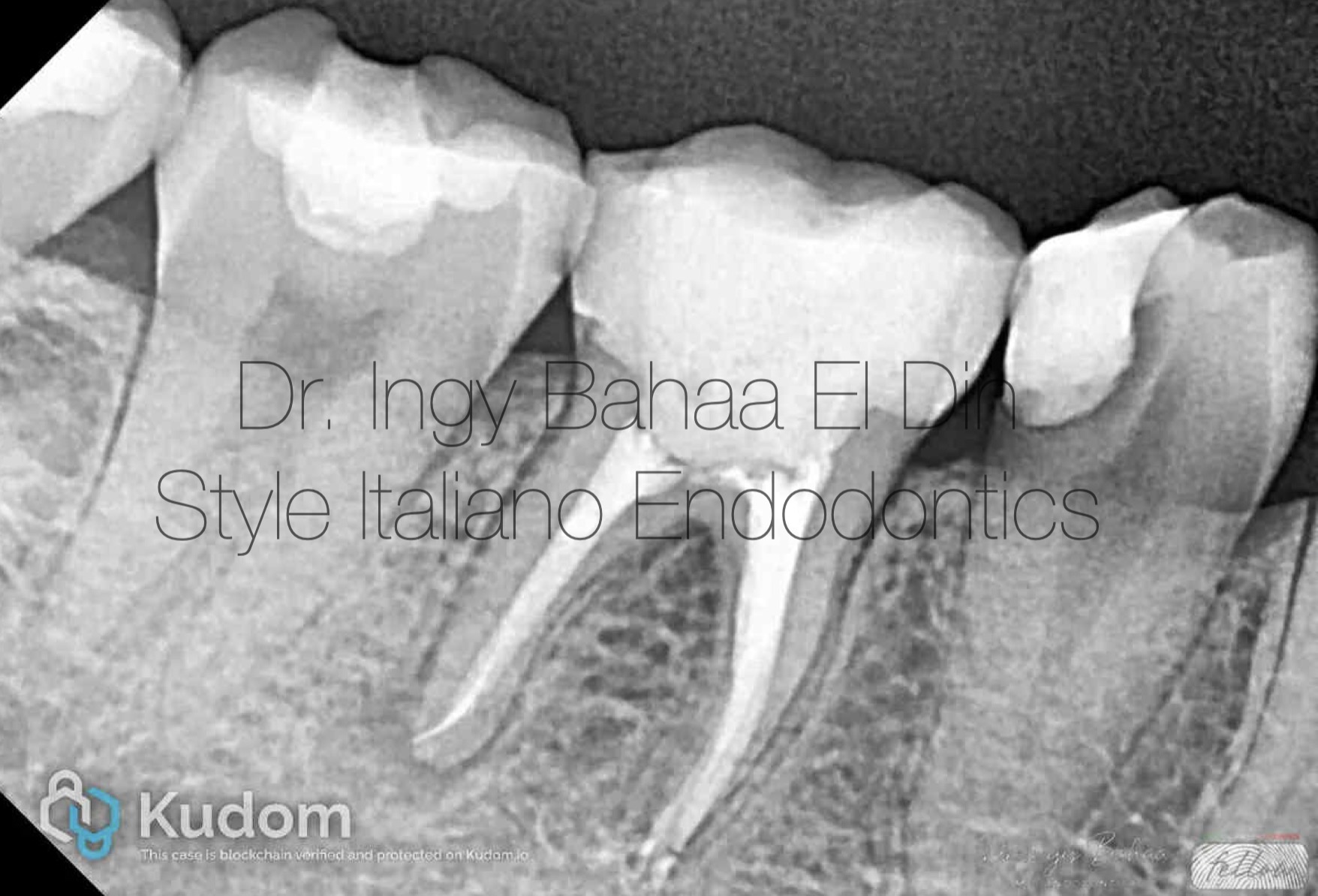
Fig. 13
Follow up xray :
After 6 Months , Follow up Xray was done showing almost complete healing in the mesial roots and a noticeable reduction in abscess size and contrast for the distal root
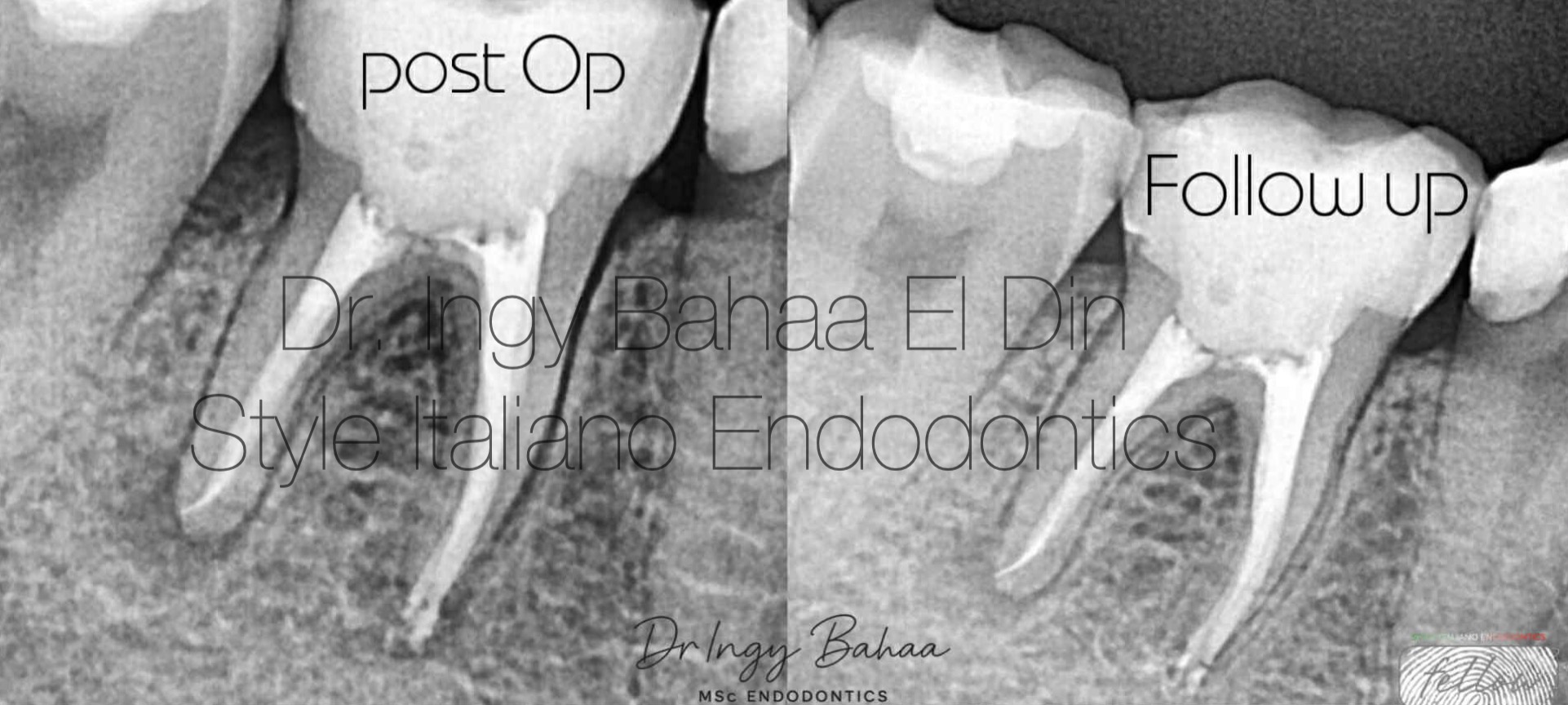
Fig. 14
Retreatment success : Asymptomatic Patient and Visible improvement of outcome in the radiograph such as minimal widening, intact lamina dura, normal pdl contour

Fig. 15
About The Author Dr. Ingy Bahaa El Din
Passion for Endodontics and Aesthetic Dentistry . Graduated with Bds from Future University in Egypt, 2011. Masters Degree Holder of Endodontics from Ain-shams University in Cairo, 2022. Co,owner and Head Operator of Beyond Dental Clinic in Cairo since 2015. Endodontic instructor at Future University in Egypt. Conducting many One to One Endodontic Courses and Speaker in Multiple National and International Conferences.
Conclusions
Retreatment can be technically challenging, often involving complications such as separated instruments, where retrieval or bypassing must be performed conservatively to avoid excessive dentin removal and structural weakening. ( shemesh at al., 2011) Ultimately, Predictable Retreatment outcomes depend on achieving maximal disinfection while preserving dentin integrity supported by modern technologies ( Dereyko at al., 2024) such as Microscopic Magnification, CBCT, Convenient Ultrasonics and niti rotary instruments. A second chance to redefine the outcome and restore biological balance required for true healing.
Bibliography
1. Nair PNR. 2006. On the causes of persistent apical periodontitis: a review. International Endodontic Journal.
2. Siqueira JF Jr, Rôças IN. 2014. Causes and management of post-treatment apical periodontitis. British Dental Journal.
3. Gomes BPFA, Pinheiro ET, Jacinto RC, et al. 2005. Enterococcus faecalis in dental root canals detected by culture and PCR analysis. Journal of Endodontics.
4. Plotino G, Cortese T, Grande NM, et al. 2016. New technologies to improve root canal disinfection. International Endodontic Journal.
5. Shemesh H, Bier CA, Wu MK, Wesselink PR. 2011. The effects of canal preparation and filling on the incidence of dentinal defects. Journal of Endodontics.
7. Hülsmann M. 1993. Methods for removing metal obstructions from the root canal. International Endodontic Journal.
8. Dereyko L, et al. 2024. Comparative analysis of CBCT and microscopy in endodontics..