Clinical Tips for Managing Calcified Canals
21/09/2023
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
One of the causes of endodontic treatment failure is calcification in the canal pathway, which prevents complete access to proper working length.
In some cases, the dentist is unable to open the calcified canal and an extraction might be suggested then.
Therefore, once calcified canals are identified, the clinician should keep in mind the following fundamental protocols, suggested in this article, pertaining to instrumentation.

Fig. 1
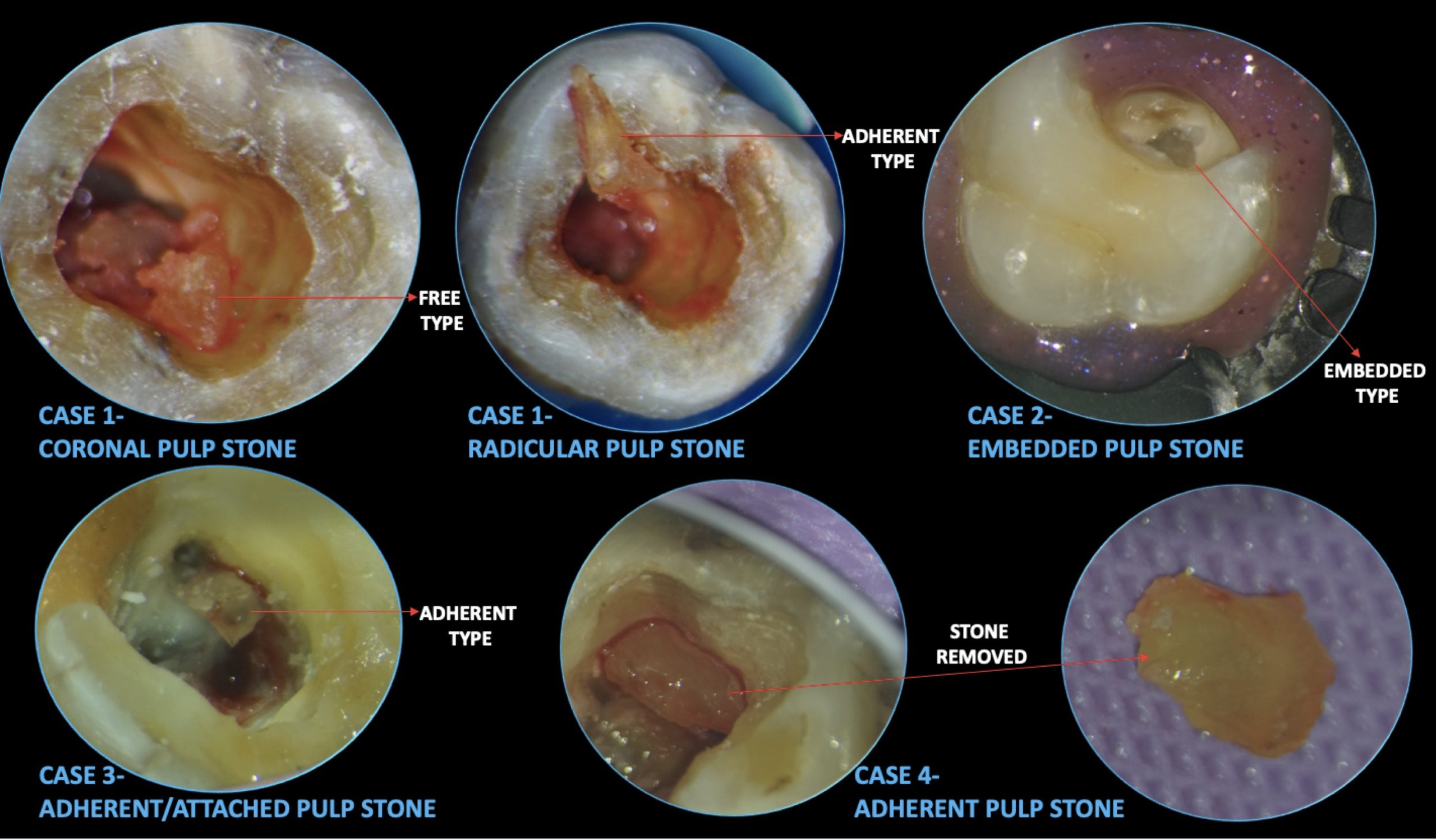
A 38-year-old, generally healthy patient visited my office complaining of hypersensitivity to cold in the lower teeth on the right side. Tooth 46 was the most sensitive to a cold stimulus (ethyl chloride). Initial periapical radiograph shows an extensive filling on the lingual wall, a homogenous radiopaque contrast within the pulp chamber (Pulp stone), and a periapical lesion on this tooth.
Pulp stones formation may be associated with long standing irritants such as caries, deep fillings, and chronic inflammation. Some authors suggest that pulp stones are a feature of an irritated pulp, attempting to repair itself (Goga et al,2008).
Pulpal pain is one of the frequent symptoms associated with pulp stones. The pain may vary from mild to severe (Goga et al,2008).
They can even cause obstruction of the root canals which leads to endodontic failure.

Fig. 2
The preparation of the pulp cavity and the removal of the pulp stone were carried out with the use of Acteon Satelec Tip No ET20.

Fig. 3
After removing the pulp stone, which filled the pulp chamber 3 canal orifices were detected: distal; mesio-buccal and mesio-lingual.

Fig. 4
Without sufficient visualization and illumination into that little endodontic access, the clinician will likely be spending too much time looking for a calcified canal and/or may not be able to locate it at all. Worse yet, you’ll be more likely to perforate the tooth in the process of drilling!
Moreover, piezoelectric ultrasonics are efficient in breaking through calcifications that covers canal orifices and removing precious dentine precisely while searching for those orifices.

Fig. 5
After all calcified canals were identified, one needs to have the right files to negotiate them.
One of all instrumentation fundamentals that has never changed over time is “ the need to begin all canal instrumentations with small stainless steel hand files” (Patino et al,2005). So I started negotiating the distal canal with a pre-curved K file 8 with a watch winding motion and after it reached the full working length I switched to Kfile10. The practice of pre-curving and watch winding the SS hand files is possibly the most important part of managing calcified root canals. If you do not do this correctly, you would easily end up with a tiny apical ledge or block that will only get worse once you use NiTi rotary files. In addition, you may easily lose your apical patency in the process (Franco et Tosco,2013).
No matter what small and flexible rotary files come to market, there is absolutely no alternative for SS hand files in initial instrumentation. The small hand files are important in creating a “glide path”.
Same protocol was applied for the two mesial canals, with NaOCl irrigation (5.25%) between instruments till I reached the full working length. At apex, I switched the motion to push pull to make the files looser in the canal.

Fig. 6
Then I used a thin nickel-titanium file with a 0.16 tip/ .2 , progressive taper made of M-Wire, allowing a certain rigidity of the file to secure the pathway of the canal and to remove restrictive dentin and other calcifications (Pullen,2023)
In this case, where I am negotiating constricted canals, the rotary file did not advance down to estimated working length as per the manufacturer instructions, therefore, I did the negotiation to full working length the traditional way, with ss K files ( 8 & 10) as describes previously.
Then I moved to a shaper file.
Irrigation to remove the debris during instrumentation with sodium hypochlorite, recapitulation and patency were always ensured after each step of shaping.
Moreover, to enhance the disinfection of canal system, I activated the NaOCl with passive ultrasonic irrigation by using an ultrasonic tip.
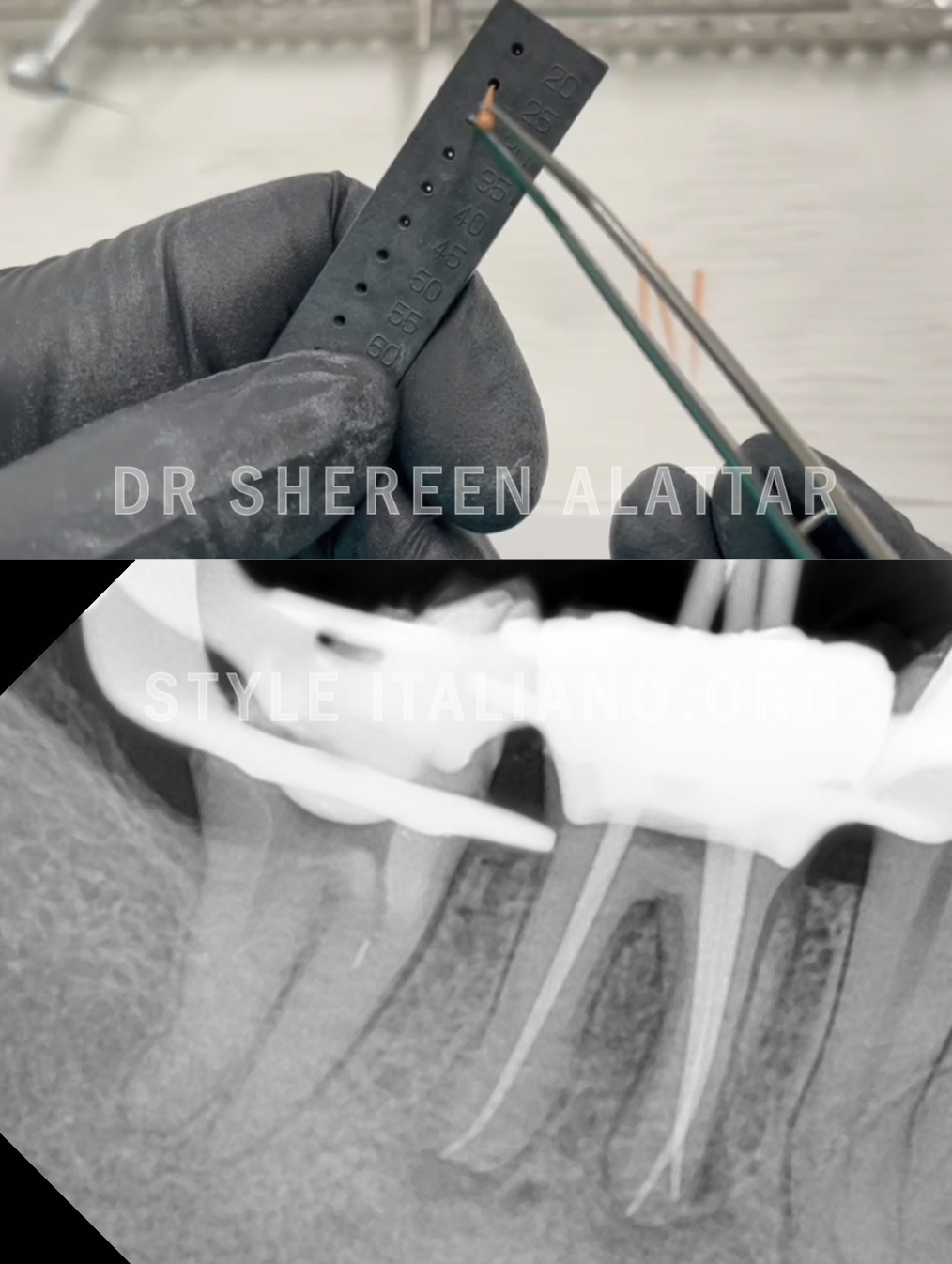
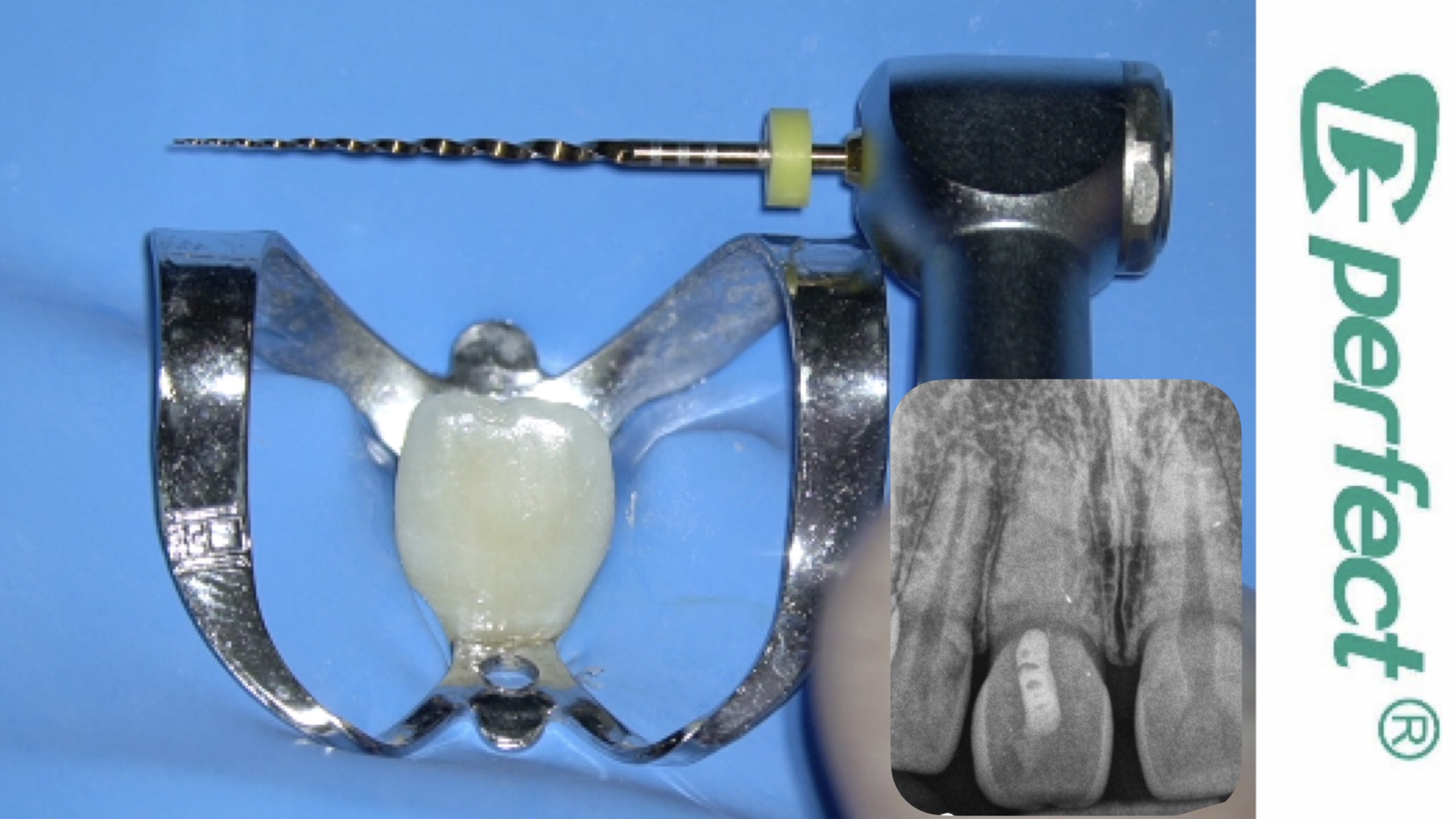
Fig. 7
Fine medium gutta percha cones were customised using the perforated ruler and a master Cone fit radiograph was taken

Fig. 8
Obturation was performed using warm vertical compaction technique where System B was used with the Buchanan fine plugger and the temperature was set at 200°C.

Fig. 9
Dr Shereen Alattar (DDS, MSc) has graduated from Saint Joseph University in Beirut, Lebanon, where she received her Master’s Degrees in the specialisation of Endodontics. She works in a referral-based practice limited to endodontics in Amman, Jordan.
She is a fellow member in Style Italiano Endodontic Group and an active member in the Jordanian Scientific Committee of the Jordanian Dental Association and in the Jordanian endodontic society
Conclusions
To sum up, the need to manage calcified canals is absolutely important. Thanks to enhanced magnification and instrumentation. Having the proper armamentaria and following basic clinical protocols is extremely crucial when instrumenting calcified canals.
I would like also to highlight the need to always think about our limits. Even with the proper armamentaria and protocols, you may realise it is still difficult to manage some calcified canals. There is nothing wrong with stopping in the middle of your procedure. The key is to know when to stop and refer. If you try instrumenting too much while getting nowhere, you may worsen the case by a ledge, zip, or perforation.
Bibliography