Calcified canal unblocking
19/02/2025
Shadi Nagi
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Diagnosis and Decision-Making in severe calcification and perforation during root canal treatment of anterior incisors pose significant challenges and require a thorough understanding of tooth anatomy and careful assessment to avoid the iatrogenic damage. Calcified canals obstruct access to the pulp, while perforations threaten tooth integrity. Effective treatment planning utilizes advanced diagnostic tools, including CBCT imaging, magnification, and ultrasonic techniques, to evaluate calcification , detect and clean perforations. The decision-making process must focus on tooth preservation, ensuring comprehensive canal debridement and sealing while minimizing iatrogenic errors in both initial and re-treatment procedures. This article explores strategies for managing calcified canals and perforations in anterior incisors.

Fig. 1
Case No. 1
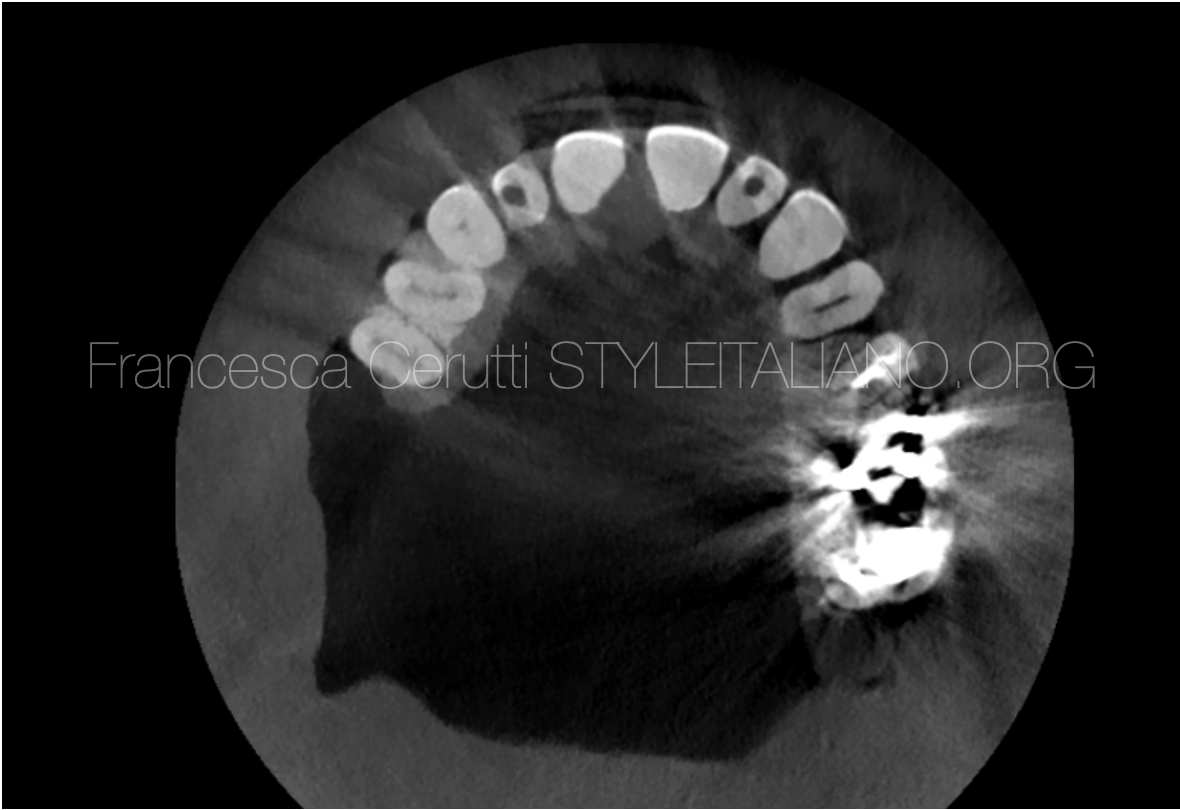
A 59-year-old patient was referred to the clinic with severe pain on biting, associated with tooth number 2.2.
Upon clinical and radiographic examination of the maxillary left lateral incisor, discoloration was noted, and the tooth was symptomatic. Additionally, there was significant calcification observed within the canal.
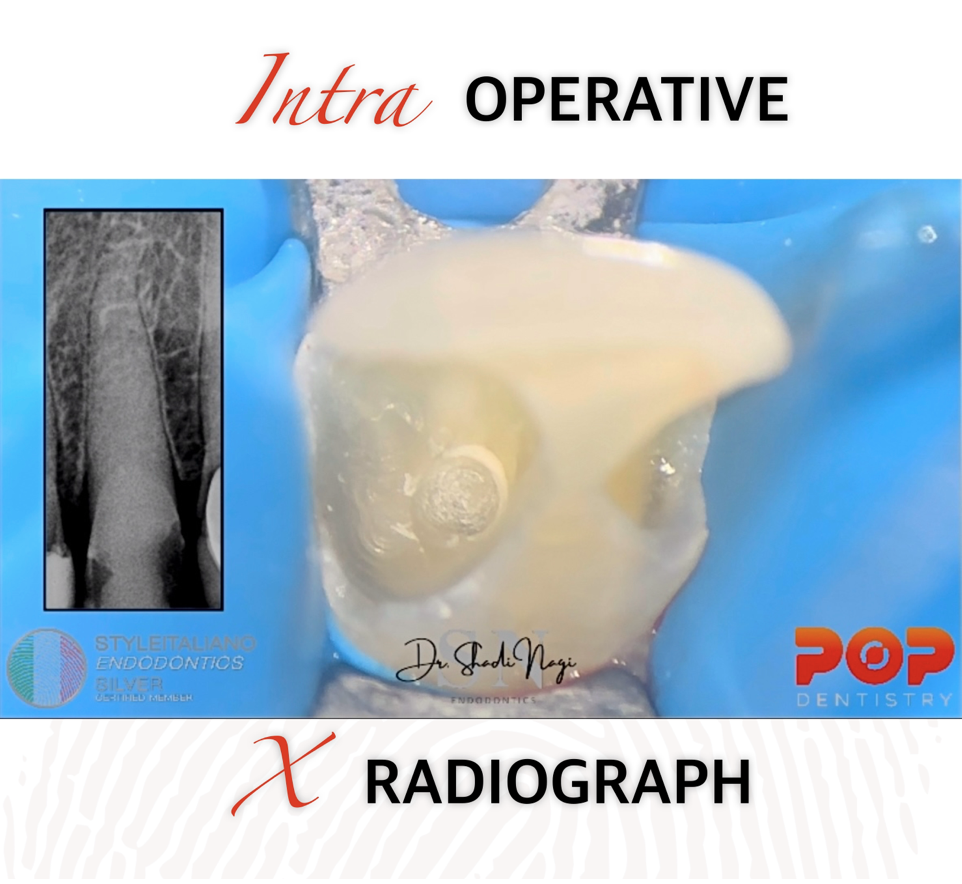
Fig. 2
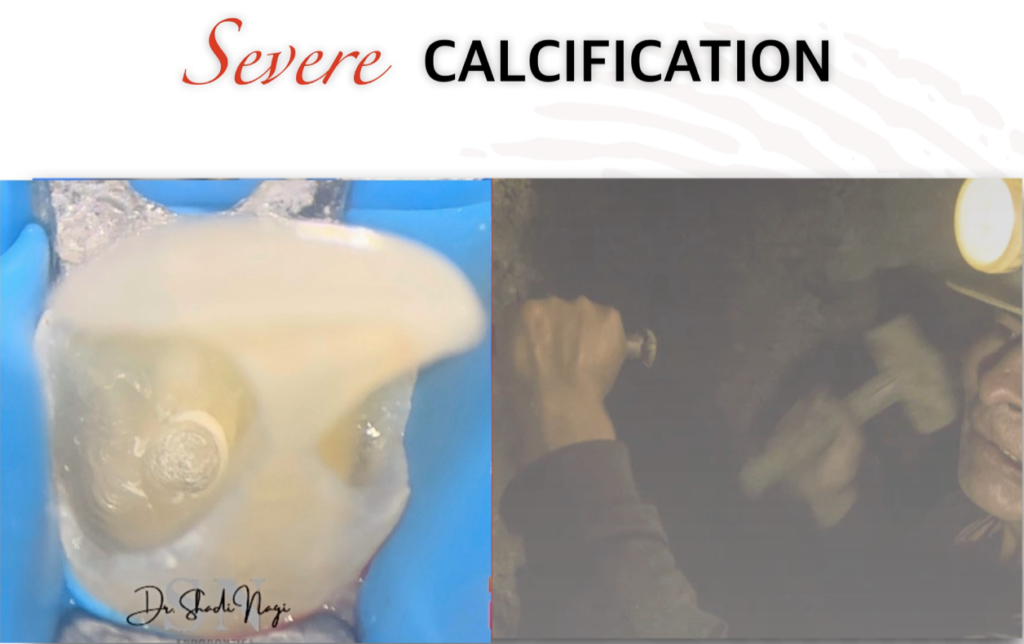
How to find the canals orifice ?
The pulp chamber floor is typically darker than the surrounding dentinal walls, creating a distinct junction. The root canal orifices are located at the angles of this junction. Developmental root fusion lines appear darker than the floor, while reparative dentin or calcifications, which are lighter, can obscure both the floor and the canal orifices.
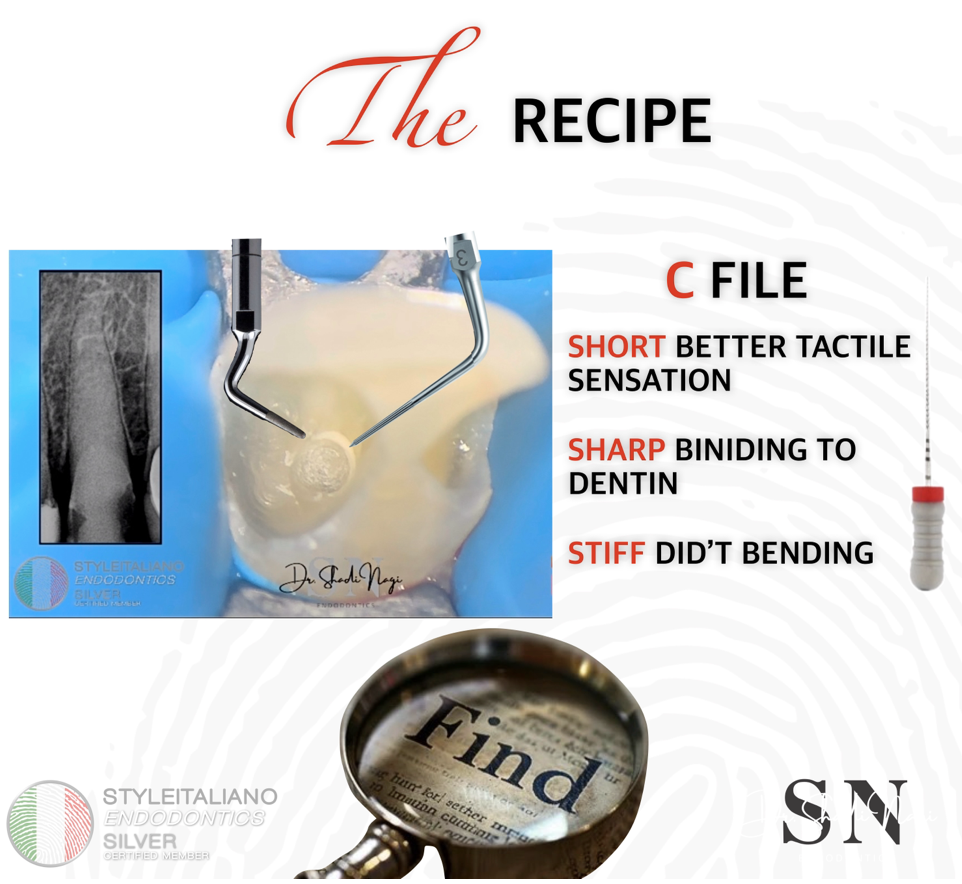
Fig. 3
The tools commonly used in managing calcified canals and perforations include magnification, ultrasonic instruments, and C-files.
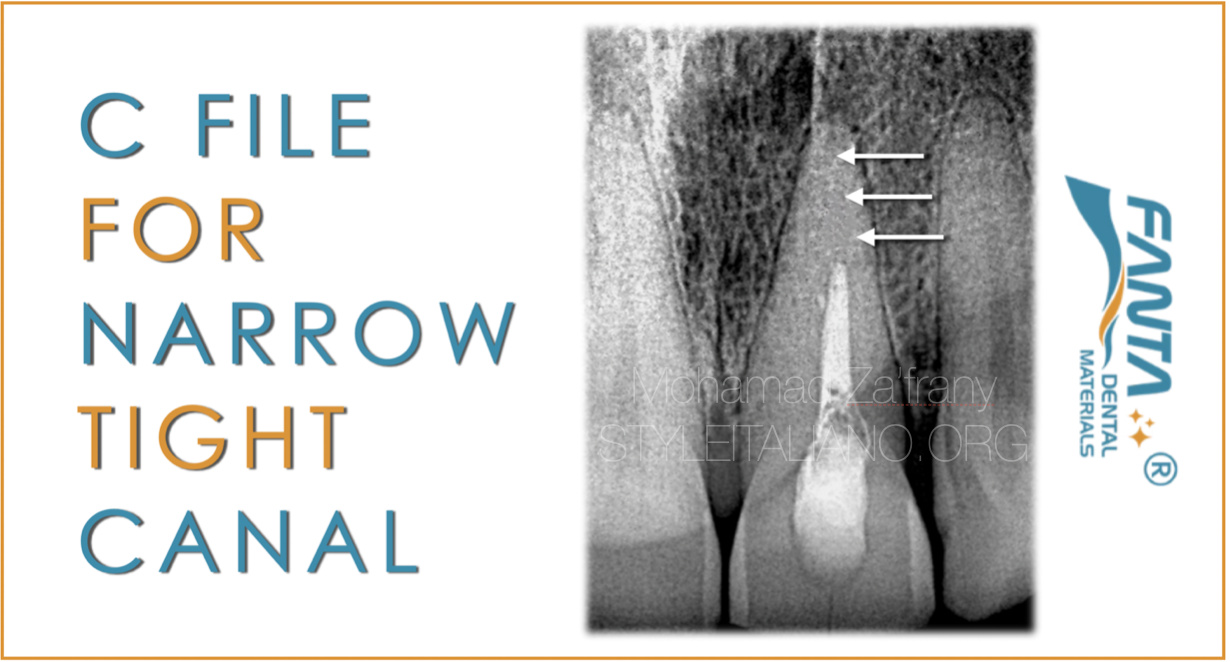
Why C-files?
C-files are preferred because their design provides enhanced tactile sensation, allowing for more precise manipulation within the canal. The short length of C-files ensures better control, while their sharp cutting edges allow for effective binding to dentin. Additionally, their rigidity prevents bending during use, ensuring stability and accurate preparation of the canal.

Fig. 4
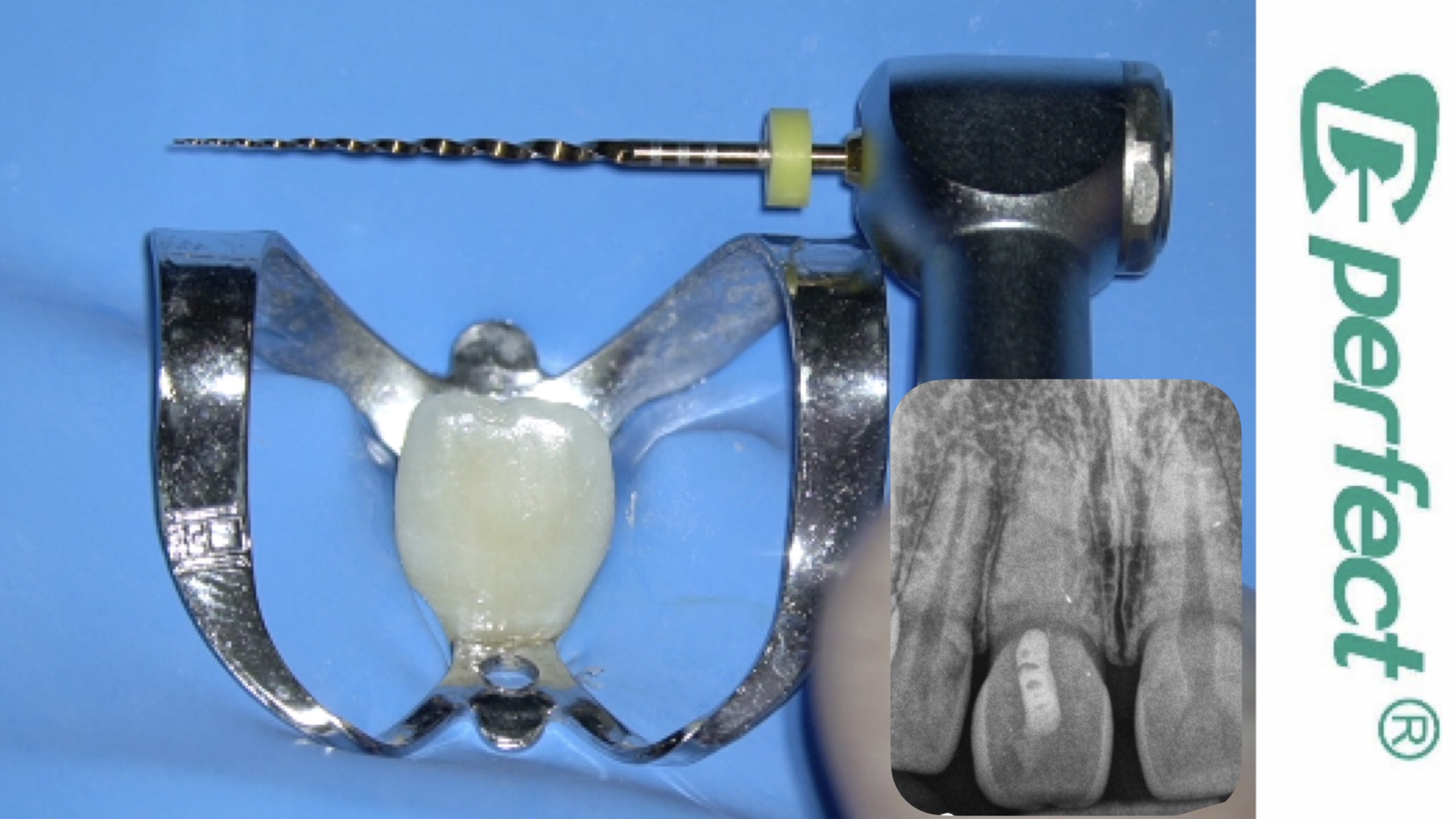
Catching the Canal and Working length determination radiograph !
Management of the case
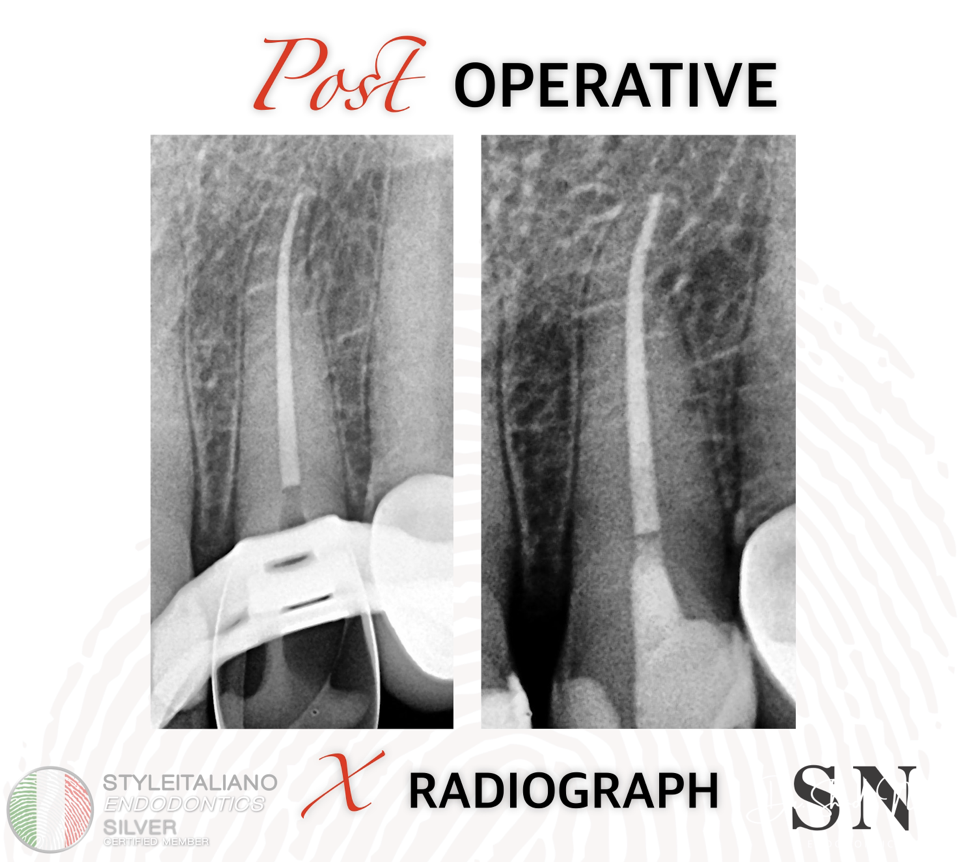
Fig. 5
The post operative radiograph
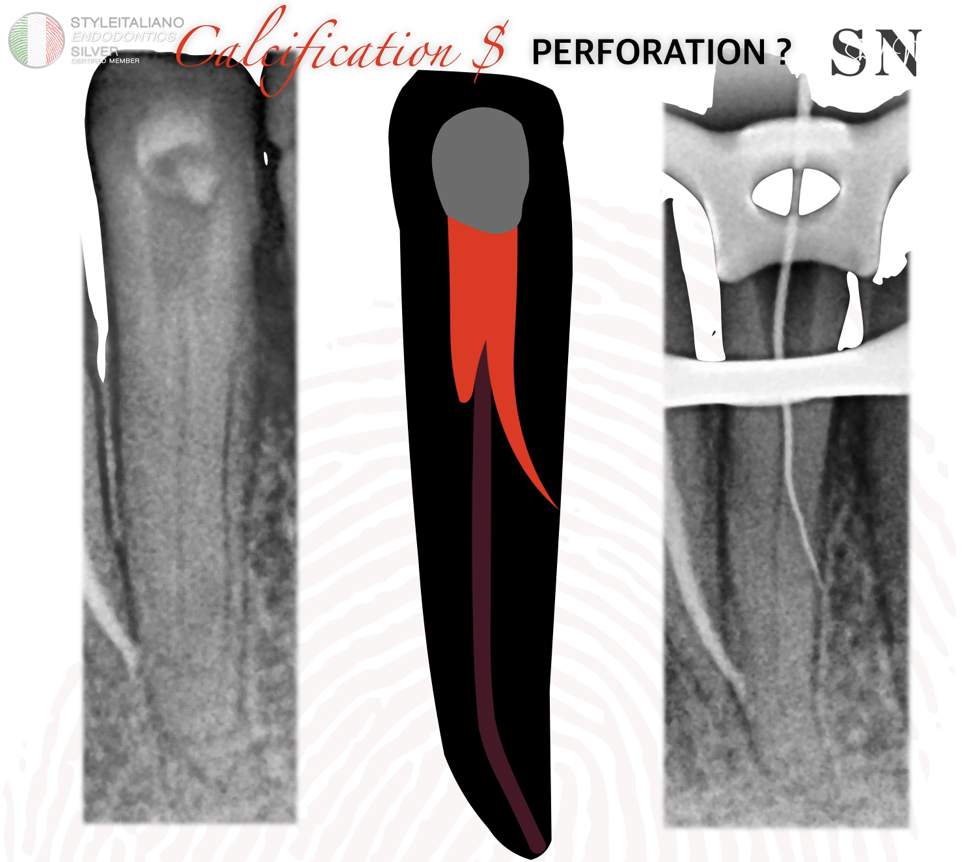
Fig. 6
CASE NO 2
A 55-year-old patient was referred to the clinic presenting with calcification, perforation, and a misdirected canal pathway. The referring dentist created an incorrect distal pathway and caused a mesial root perforation while attempting to locate the canal.
As shown in the preoperative X-ray, there is no need to continue searching within the floor of pulp chamber for the original canal pathway, as the canal orifice is located at the floor level. Therefore, the search will be redirected along the walls in the buccal or lingual direction.

Fig. 7
Initially, I began by cleaning the perforation site using ultrasonics and passive chemical disinfection. Then, cover the site with Teflon tape to prevent contamination during shaping and obturation. Afterward, remove the Teflon tape and repair the perforation with MTA.
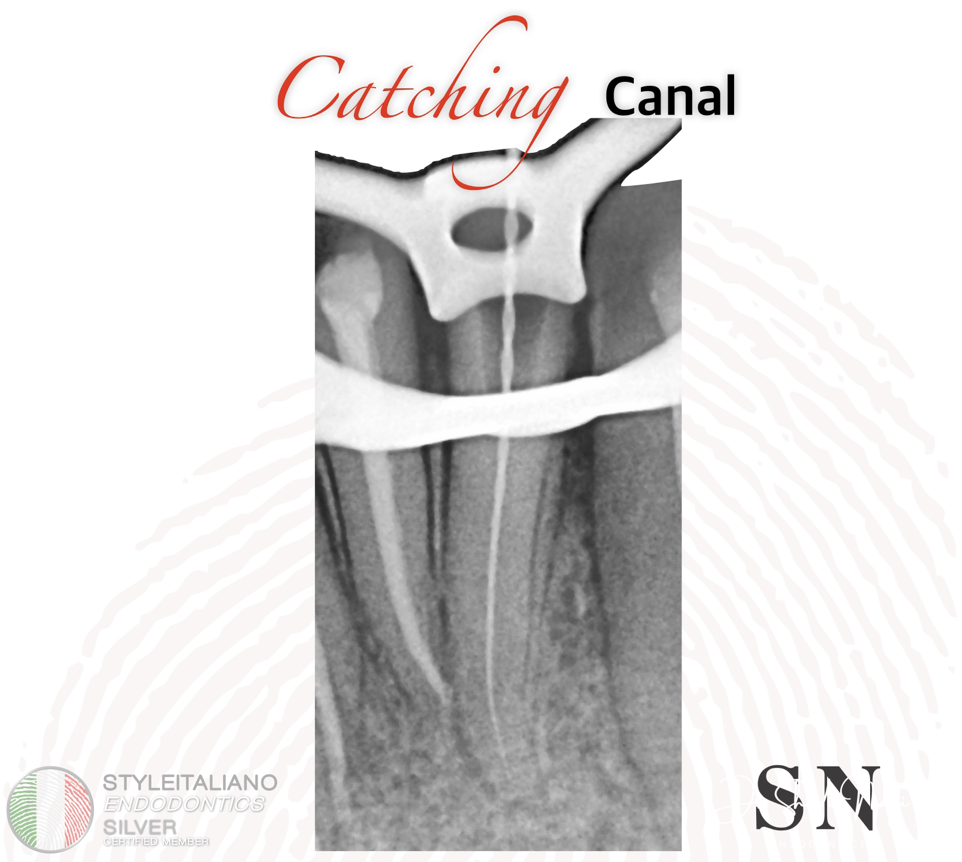
Fig. 8
Catching the original canal pathway and working length determination .
Management of the case

Fig. 9
The post operative radiograph
Conclusions
The management of calcification and perforations in endodontics requires precision, advanced diagnostic tools, Magnification and specialized techniques. With proper planning, ultrasonic guidance, and modern technology, clinicians can effectively manage these challenging cases, preserving tooth structure and ensuring long-term success.
Bibliography
1-Endodontic Treatment of Two Calcified Mandibular Central Incisors: A Case Report , https://doi.org/10.7759/cureus.53066 He , Liu , Ya Shen
2-Negotiation of Calcified Canals Antonis Chaniotis , Hugo Sausa , Anastasia https://doi.org/10.3390/jcm13092703
3-Guided endodontics in managing severely calcified teeth: A review , Georges, Ishak; Rita, Ghaleb1; Zogheib, Carla1 DOI: 10.4103/endo.endo_16_23
4-Management of Calcified Canals with a New Type of Endodontic Static Guide: A Case Report , Roberto Fornara ,Massimo Pisano https://doi.org/10.3390/dj12060166