Calcification management in the MIE era
11/04/2026
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
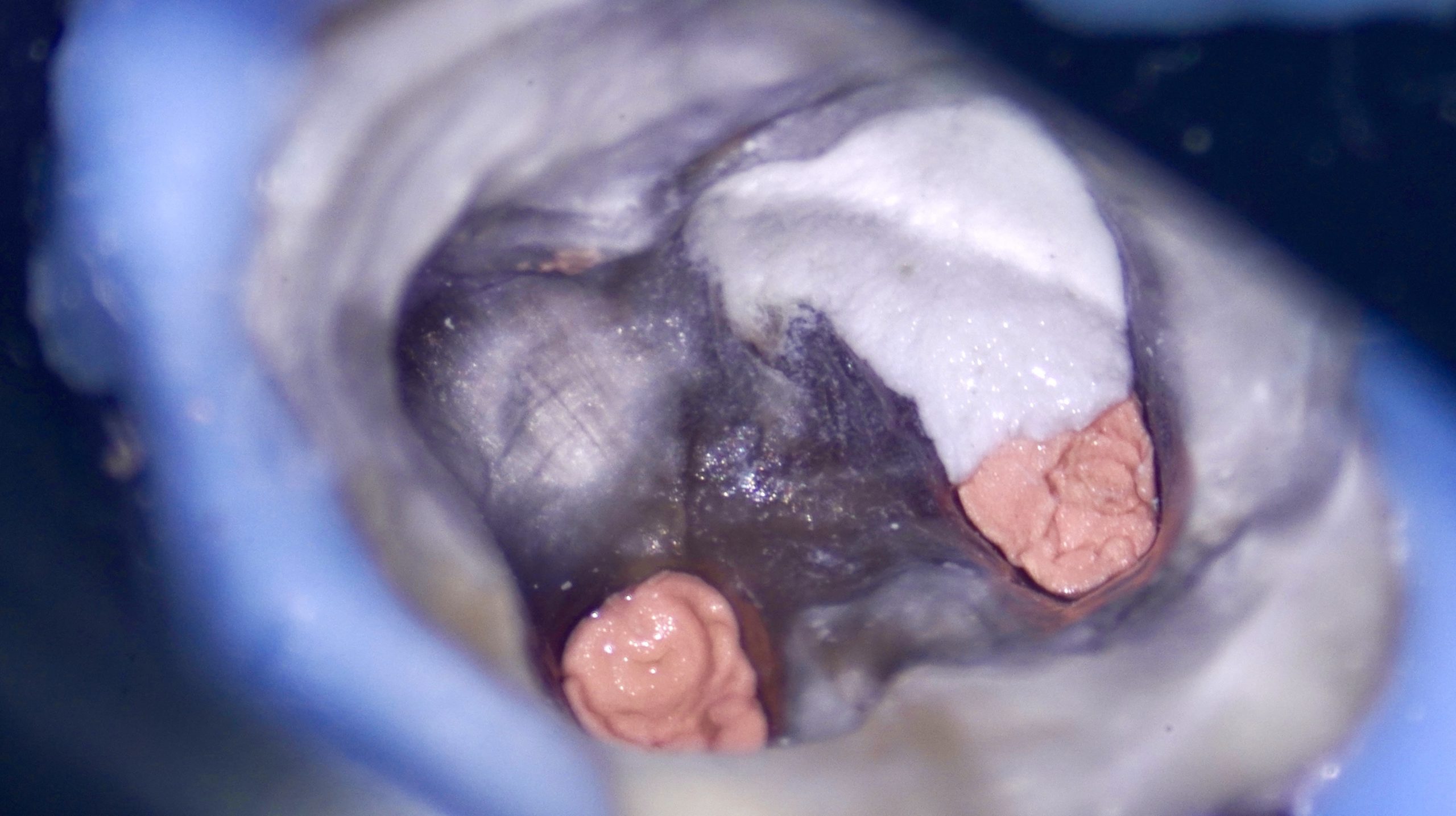
Pulp canal calcification represents a significant clinical negotiation, shaping and disinfection challenge. These cases demand a high level of clinical expertise, precise diagnosis, and a strategic approach to maintain the original canal anatomy while minimizing iatrogenic errors.
The prevalence of pulp canal calcification varies widely in. The literature, with studies reporting occurrence rates ranging from 8% to 40% in the general population. The incidence increases significantly with age, history of dental trauma, deep caries, and restorative procedures.
Mandibular first molars are particularly susceptible due to their early eruption time and prolonged exposure to irritants. Calcification may affect one or multiple canals, often leading to partial or complete obliteration.
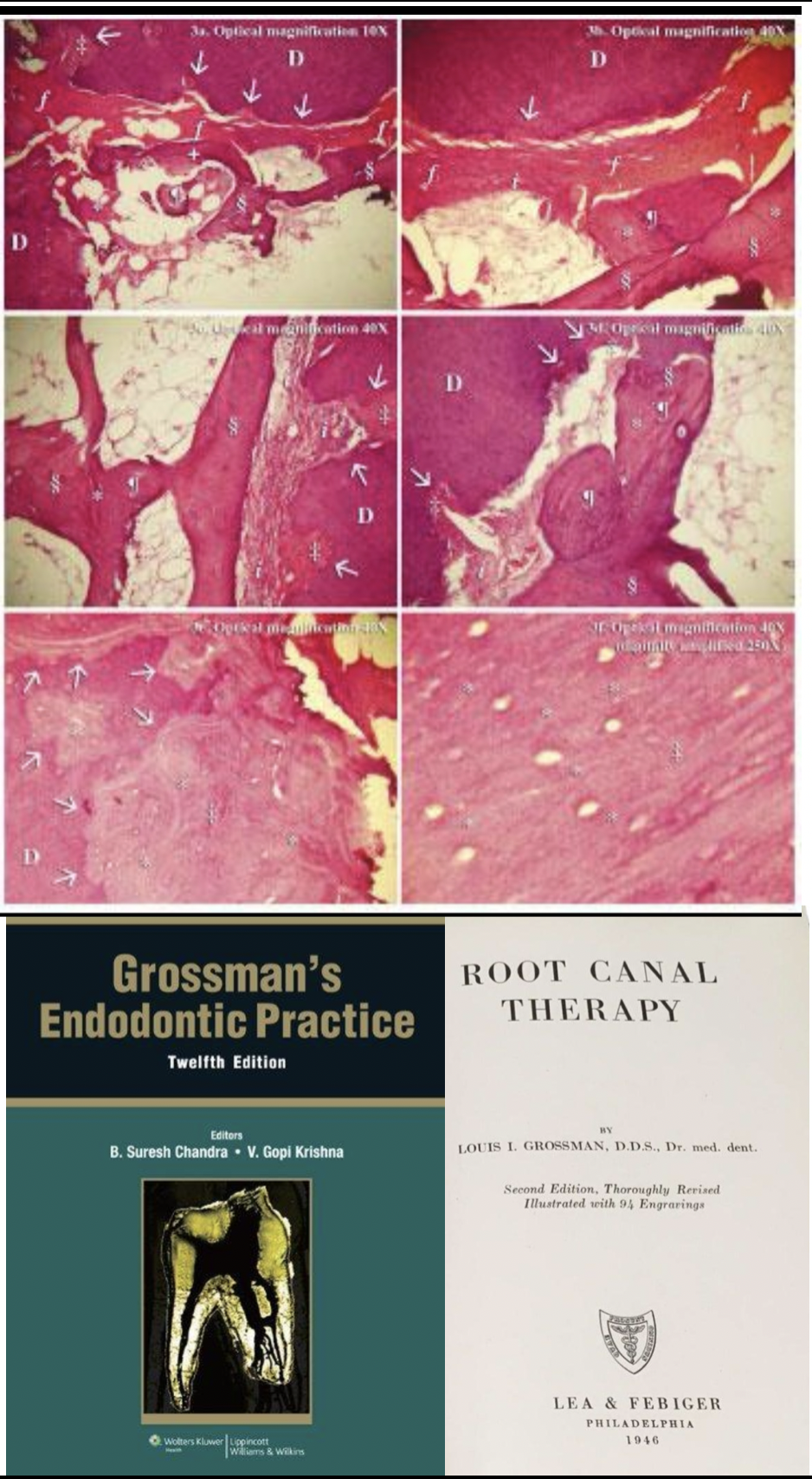
Fig. 1
Historical background
The first formal recognition and standardized terminology describing root canals can be traced back to the mid-20th century with the work of Louis I. Grossman in his seminal textbook, root canal therapy, Grossman systematically documented cases of pulp canal obliteration and calcific metamorphosis, particularly in relation of dental trauma.
Prior to this, calcification of the pulp space had been observed sporadically in anatomical and histological studies , but lacked their terminology or clinical classification. Grossman’s contribution was pivotal, as he correlated these findings with clinical and radiographic features, transforming them from isolated observations into a defined endodontic condition.
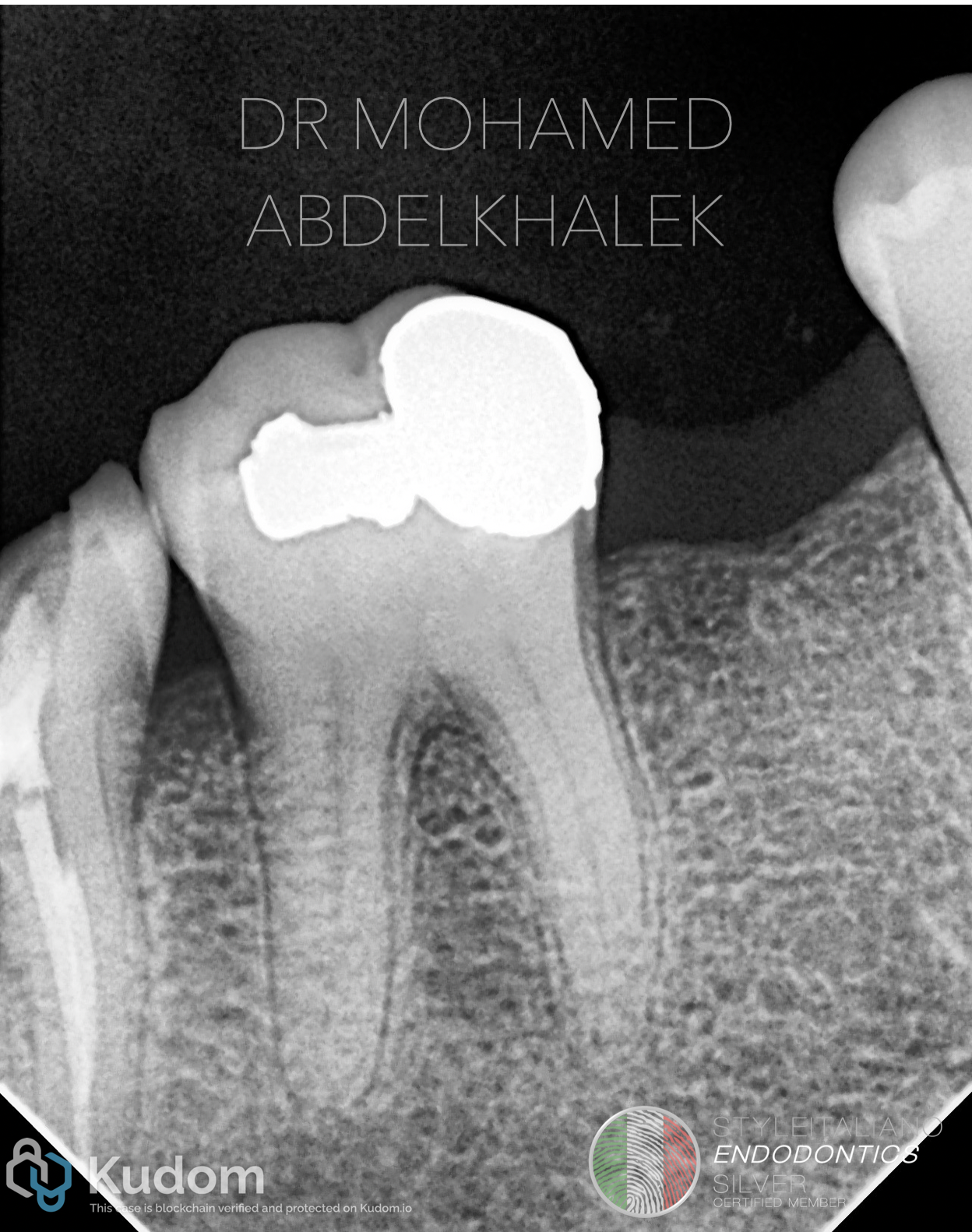
Fig. 2
Pulp canal obliteration is primarily a response to chronic irritation. The process is mediated by odontoblast-like cells that deposit tertiary dentin along the canal walls.
This reaction is triggered by :
- Long-standing caries progression
- Repeated restorative procedures
- Trauma ( orthodontic / occlusal )
- Aging
Over time, continuous dentin deposition leads to narrowing or complete calcification of the root canal system, making access and negotiation increasingly difficult

Fig. 3
The underlying mechanism of canal calcification is primarily attributed to the deposition of tertiary dentin as a response driven by the activity of odontoblasts and odontoblast-like cells within the pulp tissue.
Importantly, this calcification process is regulated than rather than chaotic. It starts from the pulp chamber to the coronal part then apically toward the apex till total obliteration. It is influenced by vascular supply, neural signaling and localized inflammatory mediators, which together determine the pattern and extent of dentin.
Minimally invasive endodontics concept
Modern endodontics emphasizes minimally invasive Endodontics (MIE), which focuses on preserving as much natural tooth structure as possible while ensuring effective cleaning and shaping.
In calcified cases, this concept becomes critical :
- Avoid excessive dentin removal
- Maintain structural integrity
- Reduce risk if perforation
- Enhance long-term prognosis
Glide path importance
Successful management of calcified canals relies heavily on establishing a secure and reproducible glide path.
In such cases, manual less kinematic strategies utilizing controlled rotary and reciprocating systems enhance precision and reduce iatrogenic errors
Gaining the glide path before enlarging the canal is crucial in such cases to prevent errors as canal transportation.
However, this approach requires advanced skills, good illumination and magnification associated with anatomical understanding. The dentin map and the color difference between the chamber walls and plural floor plays a decisive role in directing file insertion, enabling selective negotiation of the canal path without aggressive troughing or pre-flaring.

Fig. 4
Canal enlargement strategies
In this clinical case, shaping was preformed following a modern minimally invasive philosophy, aiming to preserve dentin while achieving adequate mechanical preparation.
The mesial canals were prepared up to size 20/.04 , while the distal system demonstrated.
The distal canal was enlarged up to 25/.04, in accordance with its degree of calcification and original morphology.
Notably, no pre-flaring was performed in selected segments , in order to preserve the peri-cervical dentin (PCD) and avoid unnecessary structural compromise. This reflects strict adherence to minimally invasive principles, where every micron of dentin is respected.
Such an approach particularly when executed in manual less manner demands a high level of expertise and refined kinematic execution.

Fig. 5
Obturation
Following the shaping, the canal system was obdurated using a bioceramic- based obturation technique, ensuring optimal sealing ability and biological compatibility.
Bioceramic materials offer superior flow, chemical bonding to dentin, and bioactivity making them particularly advantageous in complex and calcified anatomies where conventional sealing may be compromised

Fig. 6
A shifted angulation radiograph was taken to enhance anatomical interpretation. The mesial canals demonstrated a type II configuration, where two canals join into a single pathway apically. Similar, the distal communication between the distal canals.
The angulated view was essential in revealing the true canal anatomy, which was not clearly evident in the initial straight projection.
This video elaborates the clinical steps from the access cavity to the final obturation
Conclusions
Management of calcified canals represents the intersection of biology, technology and operator skill. From early recognition in the pat century to modern minimally invasive strategies, the evolution of this field highlights a continuous pursuit of precision with preservation.
This case demonstrates that, through careful planning, conservative shaping and advanced kinematics control, even highly calcified canals can be managed predictably without sacrificing the structural integrity of the tooth.
Bibliography
1. Management of calcified root canals
Siqueira JF Jr, Rôças IN. Management of calcified root canals. Endod Topics. 2014;29(1):96-111.
2.Pulp canal obliteration after trauma
Oginni AO, Adekoya-Sofowora CA, Kolawole KA. Pulp
canal obliteration after dental trauma: a review. Dent Traumatol. 2009;25(4): 389-394.
3.Reactionary and reparative dentin formation
Smith AJ, Cassidy N, Perry H, Bègue-Kirn C, Ruch JV, Lesot H. Reactionary dentinogenesis. Int J Dev Biol.
1995;39(1):273-280.
4.Minimally invasive endodontics concept
Clark D, Khademi J. Modern molar endodontic access and directed dentin conservation. Dent Clin North Am.
2010;54(2):249-273.
5.Glide path in endodontics
Berutti E, Paolino DS, Chiandussi G, et al. Root canal anatomy preservation using NiTi rotary instruments and glide path. Int Endod J. 2012;45(7):616-628.
6.Nickel titanium instruments review
Walia HM, Brantley WA, Gerstein H. An initial investigation of the bending and torsional properties of Nitinol root canal files. J Endod. 1988;14(7):346-351.
7.Bioceramic sealers review
Zhang W, Li Z, Peng B. Ex vivo cytotoxicity of a new calcium silicate-based canal filling material. Int Endod J. 2010;43(9):769-774.