Dental Diagnosis Dilemma
04/08/2024
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Referred case for a patient that has been treated for 2 months for trigeminal neuralgia and the pain she had did not go away.
This patient has past 4 experiences with dentists that did not find anything at all and it ended up extracting tooth number 7.
Trigeminal neuralgia has symptoms close to sharp shooting pain with inability to touch the face in her case it was near tooth number 6 and 7 lower mandibular molars.
Unfortunately she came to me already with a tooth extracted but it our mission is to improve patient’s quality of life and getting to the root of the problem.
Careful diagnosis is the key by examining all upper and lower teeth with x-rays, percussion, palpation, tooth sloth and Endo-Ice.
Last clue I had is to send her for a CBCT to tooth number 6 which had “proper root canal treatment” on preoperative x-ray but we should always think 3D.
And here was the culprit, missed split middle half distal canal and short defective obturation mesial canal.
This case demonstrates the importance of diagnosis to make patient’s life better.
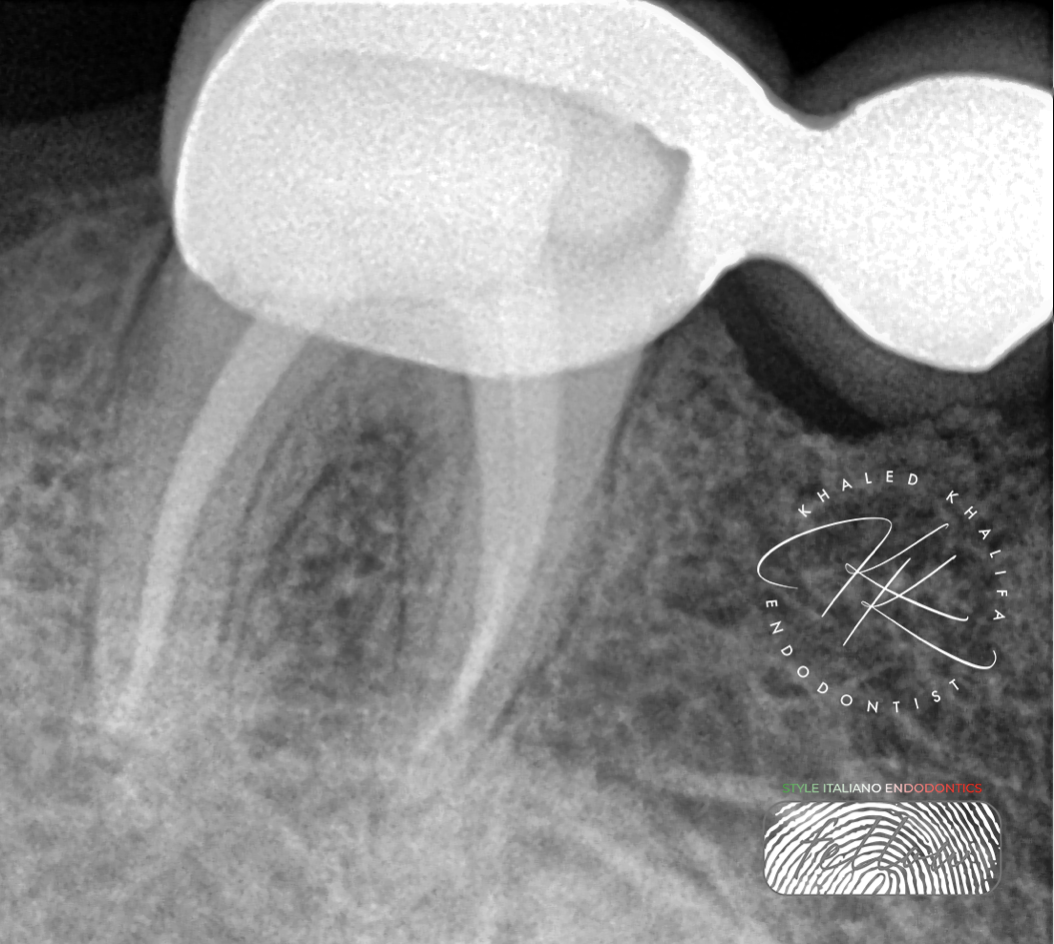
Fig. 1
Preoperative X-Ray not showing enough data and the x-ray looked fine.
Sending patient to CBCT is a must to determine if there is actually a problem or not.
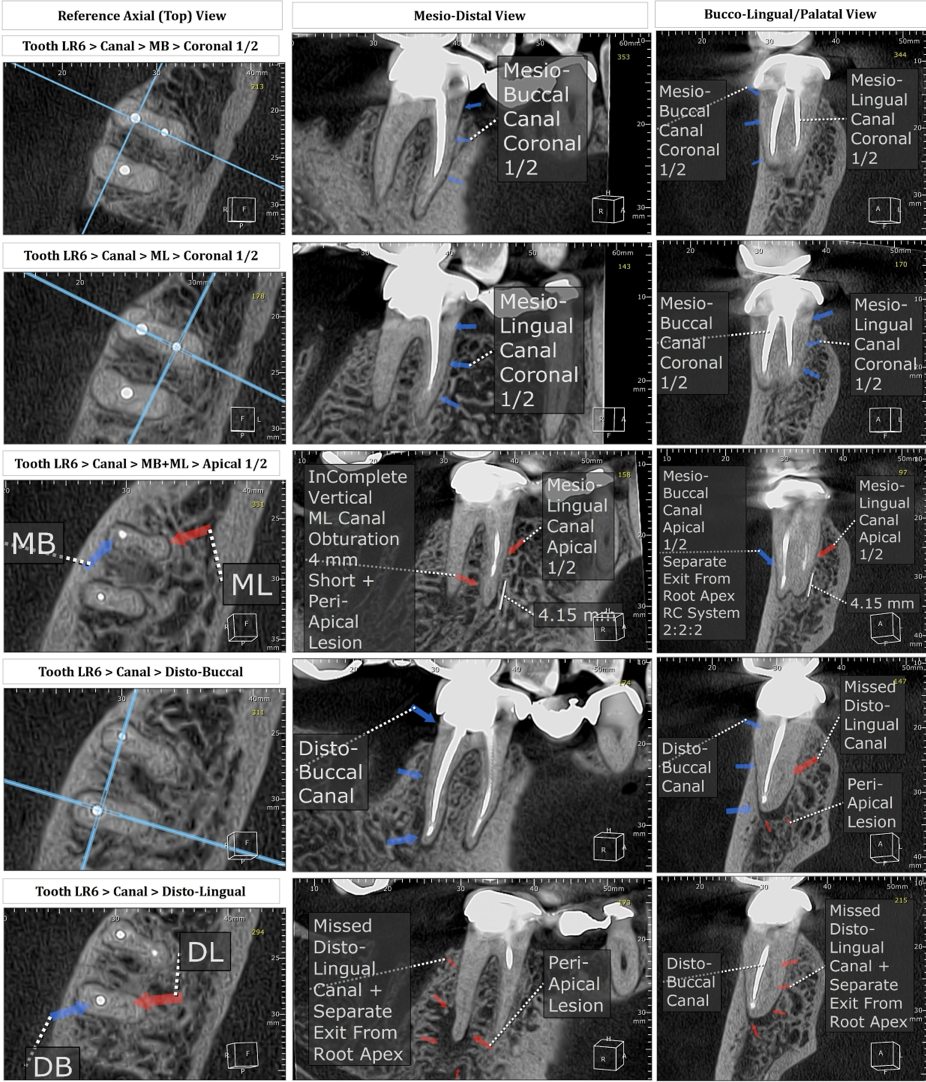
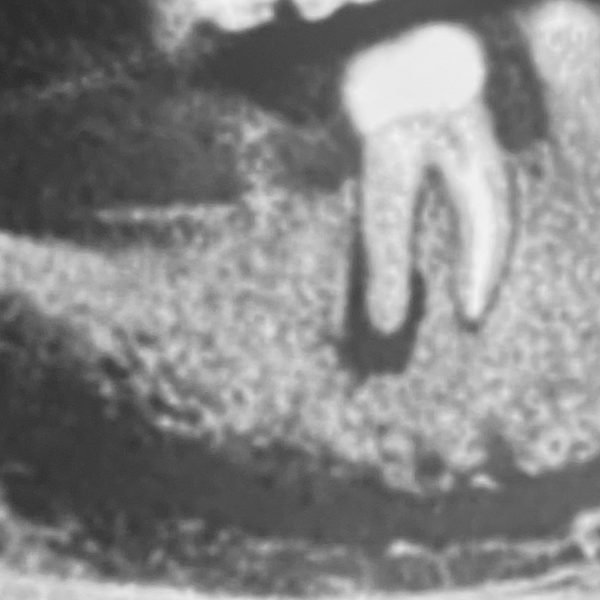
Fig. 2
CBCT Examination showed:
- Missed DB canal split at middle half and separate apex.
- Short ML canal obturation.
- Periapical radiolucency beneath both apices.

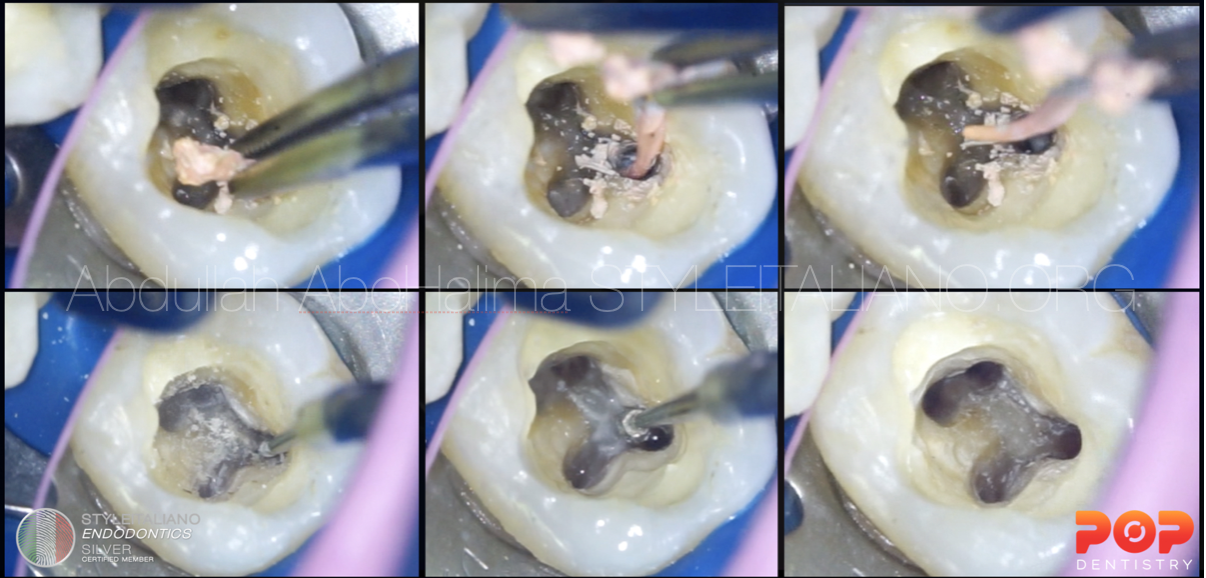
Fig. 3
Macro shot of finding the DB canal.
I always try to find the missed canal first and shape it, before removing the GP from other canals.
Using U.S to trough up to middle half at the division level & using full conc sodium hypo to flush out debris.
Catching the canal via DG16 and negotiating it and enlarging it.
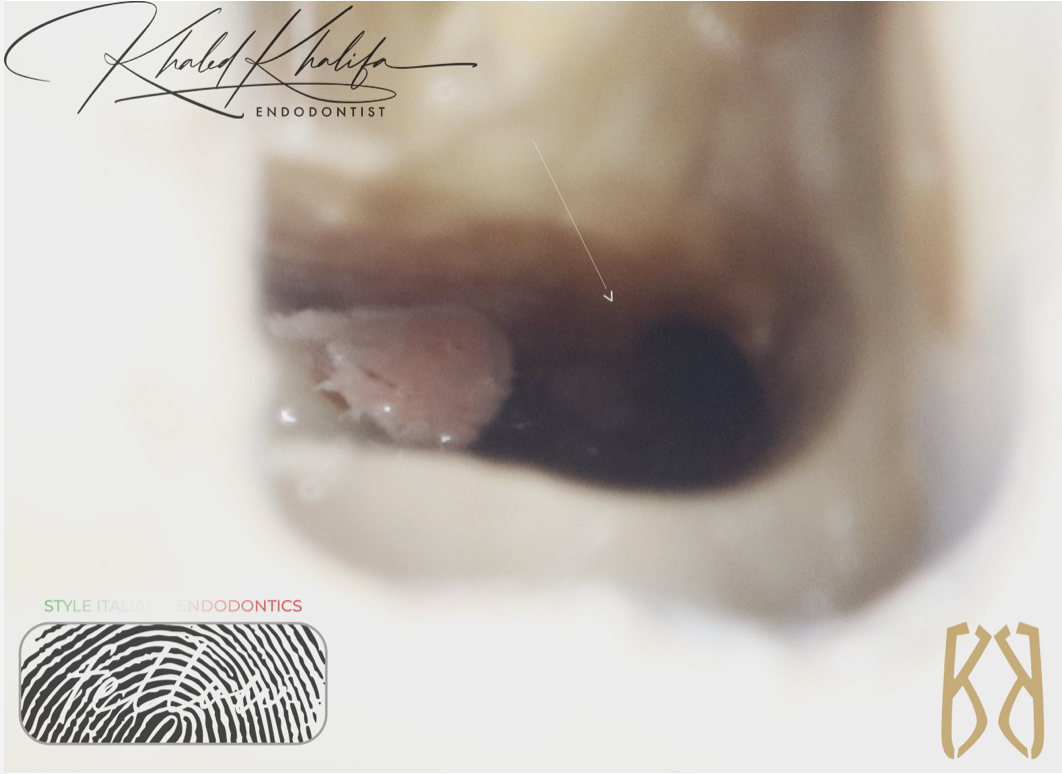
Fig. 4
Here you can see the canal very deep down and using this trick its easier to identify and not to slip by mistake into the other canal.

Fig. 5
Here we removed all GP, finished all canals prep and implemented great irrigation protocol to prepare the case for obturation.

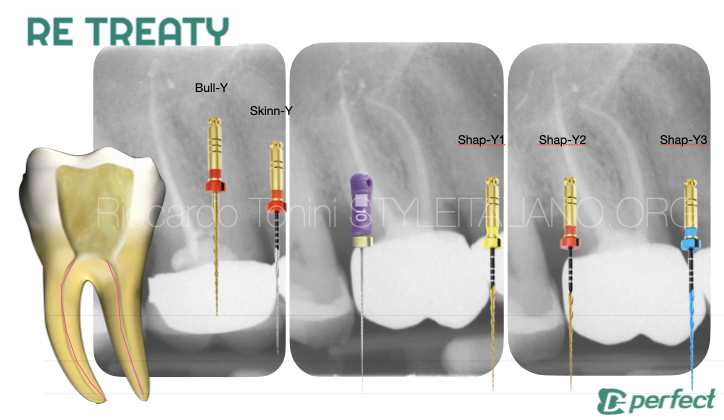
Fig. 6
TCA technique is great for these types of cases by placing CM wire files manually then mounting the rotary device to select which canal to prepare.

Fig. 7
Post operative Xray showing 3D obturation to all canals and split.
Using bioceramic sealer and Continous wave obturation technique to maximize the success rate of the case.

Fig. 8
About the author:
Dr Khaled Khalifa
B.D.S. Misr International University
Endodontic Specialist
Course Director “The Endo Formula”
Endodontic Consultant in multiple private clinics
Member of The Royal College of Surgeons England (MJDF)
Member of The American Association Of Endodontics (AAE)
Member of British Association Of Endodontics (BES)
Practice limited to Endodontics
Conclusions
Such cases improve the quality of patient’s life and it relies the most on diagnosis before any clinical skills.
This patient on follow ups completely healed & stopped her trigeminal neuralgia medications and I have been following her up to 6 months to make sure there is no recurrence of symptoms.
Bibliography
- Abbott P, Diagnosis and management planning for root-filled teeth with persisting or new apical pathosis.
Endodontic Topics, 2008. 19(1): p. 1-21. - Friedman S, Considerations and concepts of case selection in the management of post-treatment
- Zhang MM, Fang GF, Chen XT, Liang YH. Four-year outcome of nonsurgical root canal retreatment using cone-beam computed tomography: a prospective cohort study. J Endod 2021;47:382–90.
- Schilder H. Filling root canals in three dimensions. Dent Clin North Am. 1967; : 723-74Reit C. Grondahl H.G. Management of periapical lesions in endodontically treated teeth:ùstudy on clinical decision making. Swed Dent J. 1984; 8: 1-7
- Witherspoon DE, Small JC, Regan JD. Missed canal system are the most likely basis for Endodontics pretreatment of molars.Tex Dent J. 2013 Feb;130(2):127-39.
- Baruwa AO, Martins JNR, Meirinhos J, Pereira B, Gouveia J, Quaresma SA, Monroe A, Ginjeira A. The Influence of Missed Canals on the Prevalence of Periapical Lesions in Endodontically Treated Teeth: A Cross-sectional Study. J Endod. 2020 Jan;46 (1) 34-39.