Premolar gemination: a case report
06/07/2026
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Gemination is a rare developmental dental anomaly resulting from the incomplete division of a single tooth germ, producing an enlarged crown with varying degrees of root and canal complexity. In the permanent dentition, it most frequently affects anterior teeth, whereas involvement of mandibular premolars is exceptionally uncommon. This unusual anatomy can complicate diagnosis and treatment planning, particularly when endodontic intervention is required.
Successful management of geminated teeth relies on a thorough understanding of their highly variable internal morphology. Conventional radiography may not adequately reveal the complexity of the root canal system, making advanced imaging and magnification valuable adjuncts for achieving predictable outcomes.
This article presents the nonsurgical endodontic treatment of a geminated mandibular right second premolar. The case highlights the importance of careful diagnosis, modern endodontic techniques, and a systematic approach to managing complex anatomical variations, ultimately demonstrating that even exceptionally rare developmental anomalies can be treated successfully with meticulous planning and execution.
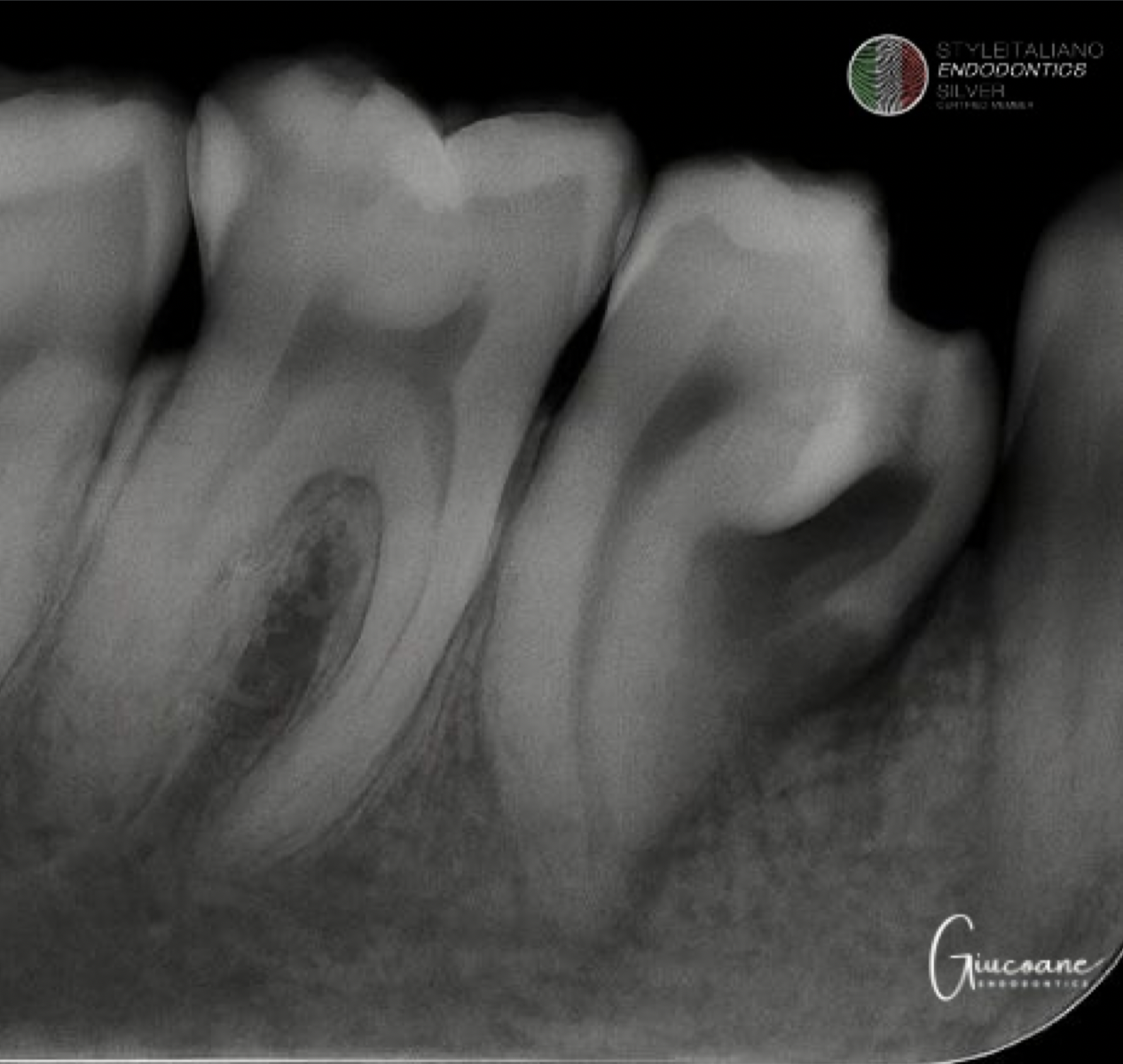
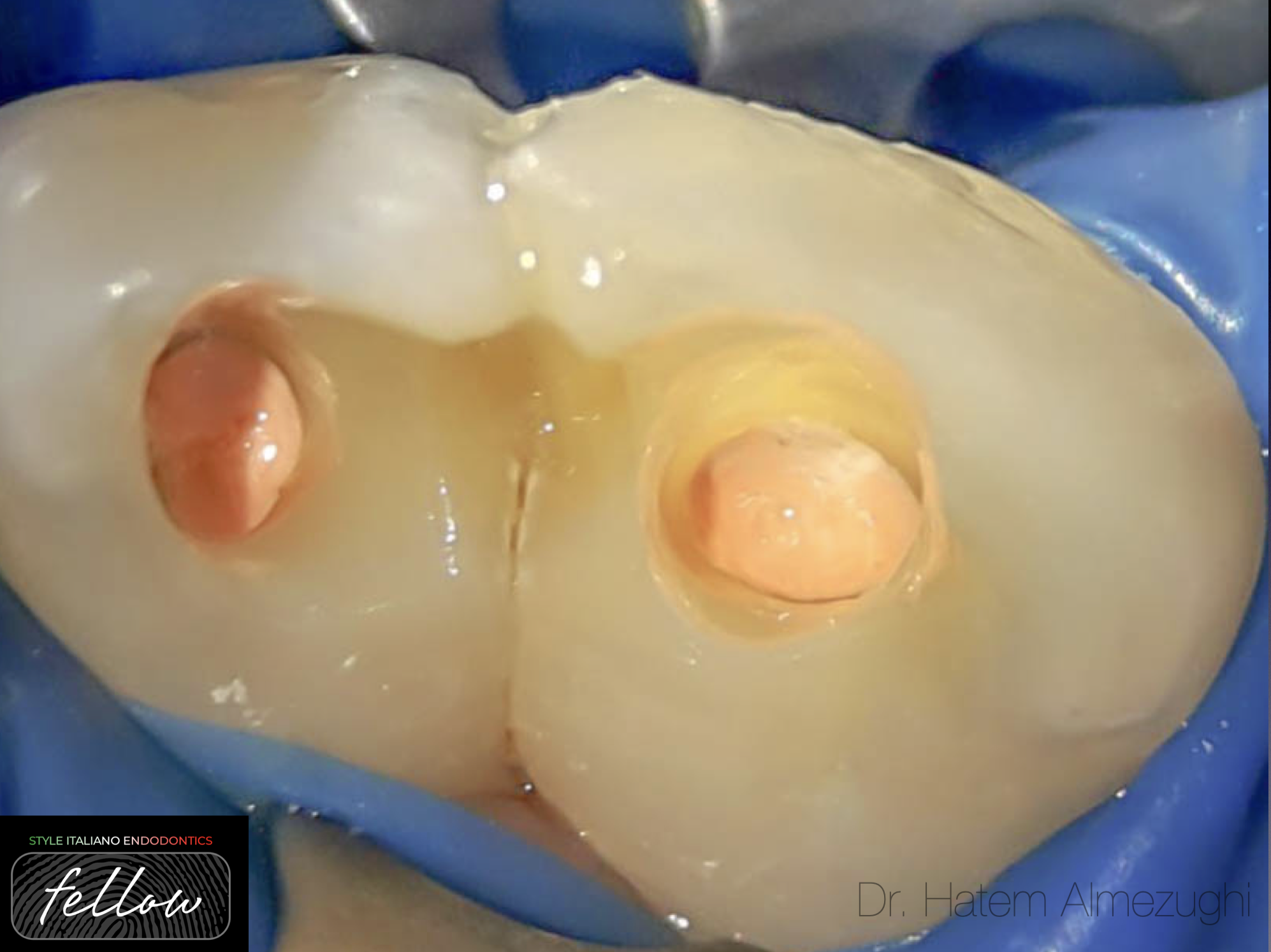
Fig. 1
A healthy 25 years old patient arrived in the office 7 days after she received an emergency treatment from a general dentist.
The colleague used a bur to open the mesial root and placed a temporary cement hoping the acute episode will subside. Following this treatment he referred the patient to our practice.

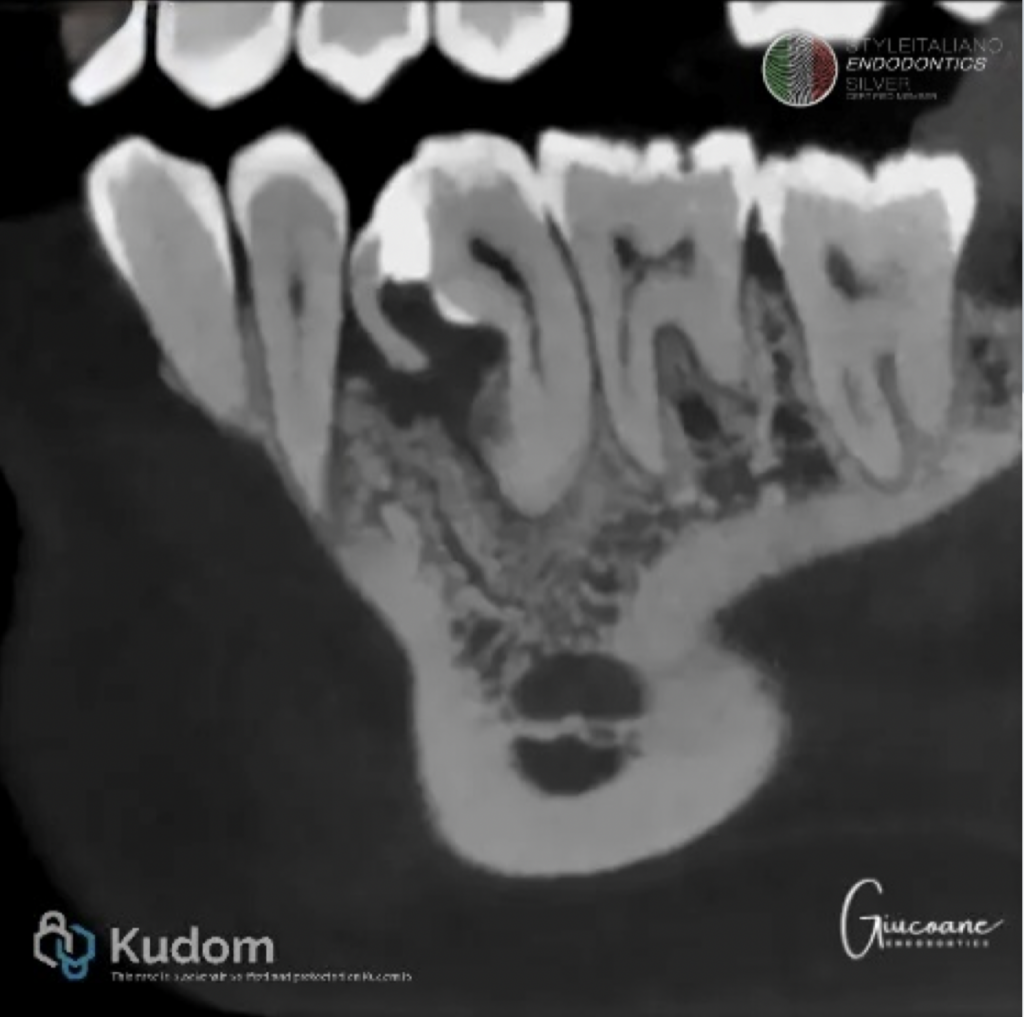
Fig. 2
The patient arrived complaining of spontaneous pain in the lower right jaw. CT scan revealed a 4.5 with gemination in which the supernumerary presented radiolucency on the mesial side from the coronal portion up until the portal of exit which looked either resorbed or perforated.
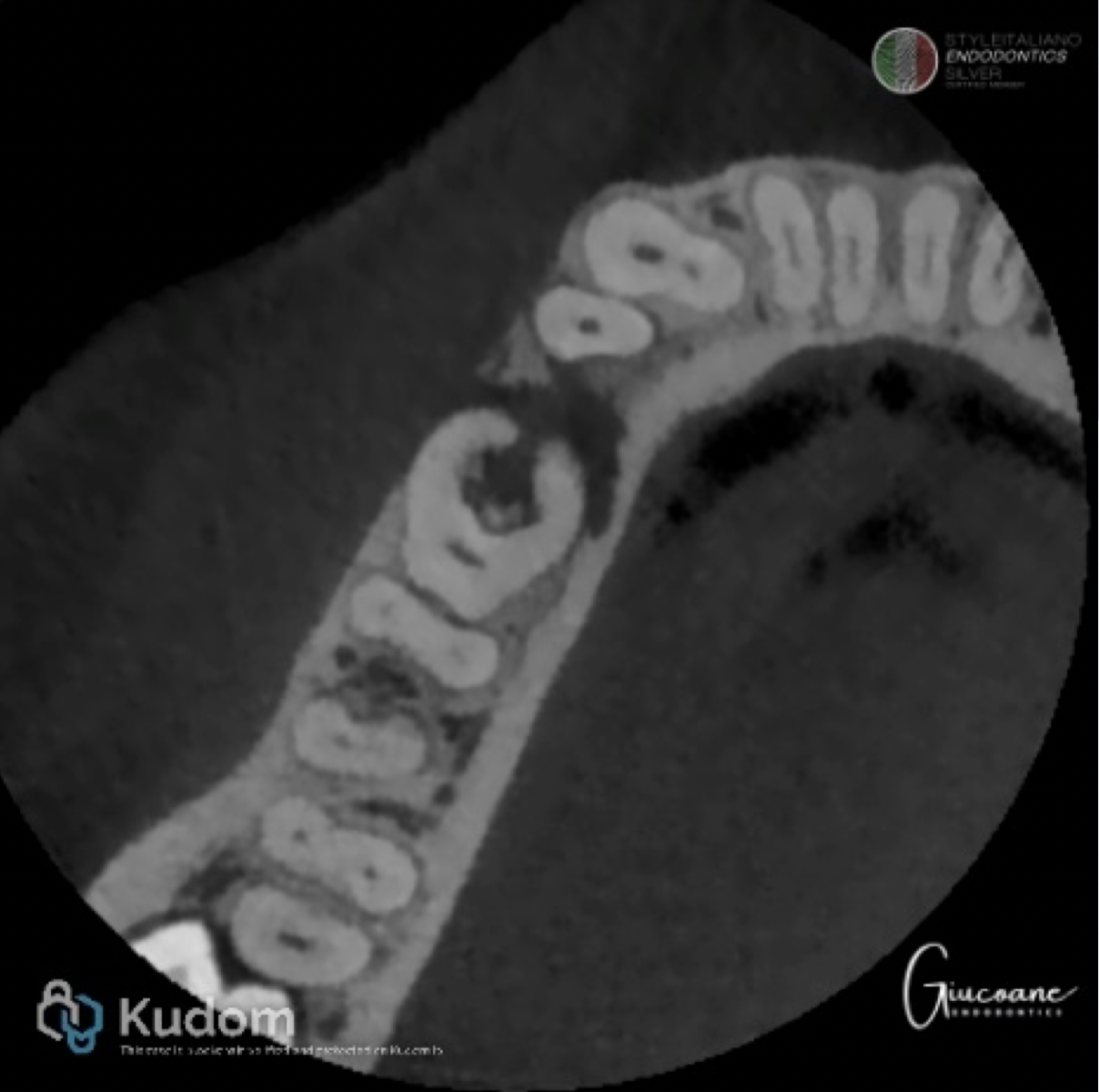
Fig. 3
Sensitivity tests were negative while percussion was positive.
Probing was limited to 5 mm but the round shape of the mesial portion was considered a possible cause.

Fig. 4
After taking into consideration all the clinical and paraclinical factors the diagnosis according to the AAE and ESE classification was pulp necrosis and localized symptomatic apical periodontitis.
The patient agreed to have a root canal treatment.
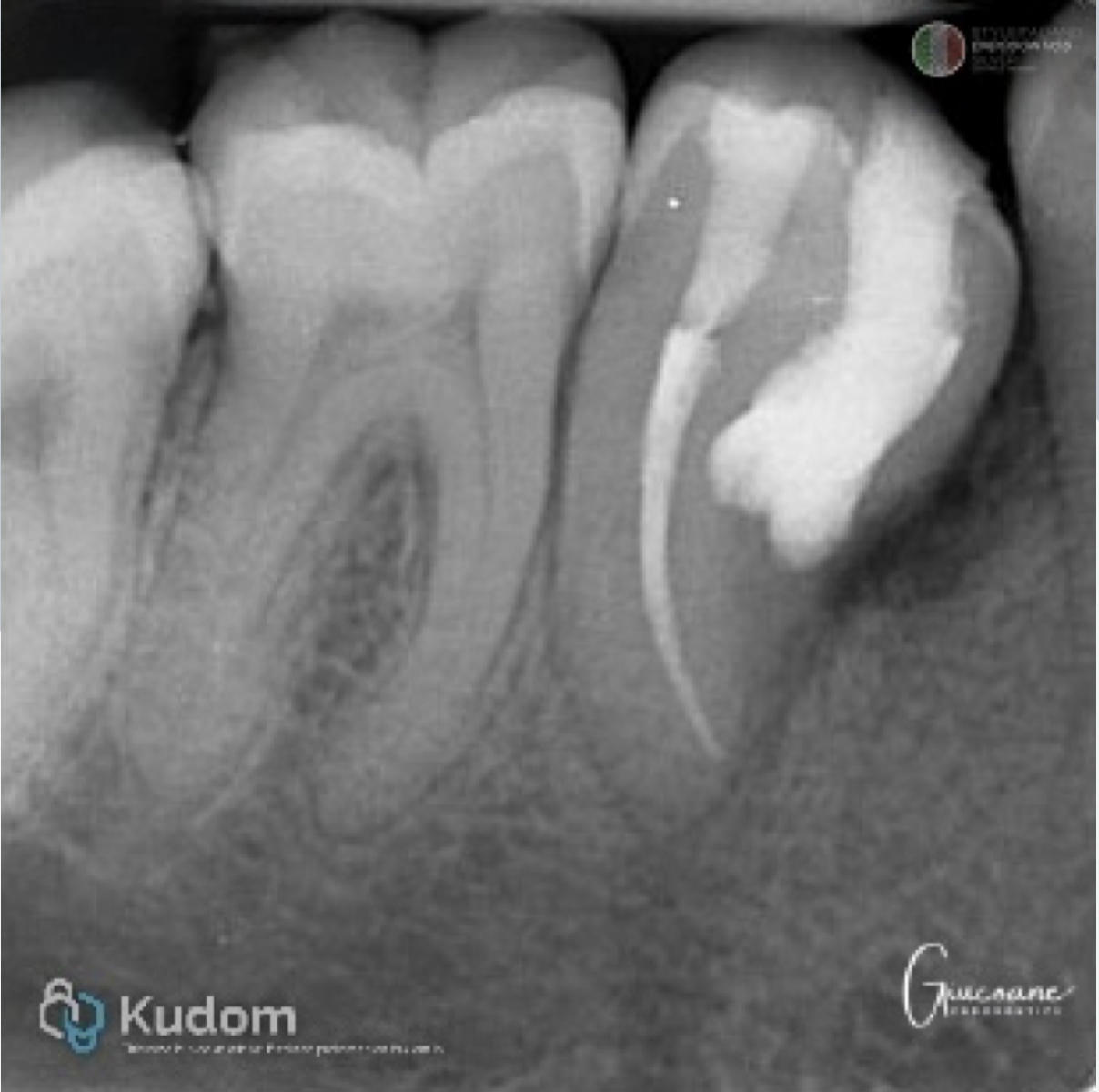
Fig. 5
1. After isolation, the temporary restoration was removed.
2. The perforation/resorption was located and debrided using small excavators.
3. The supernumerary root canal was irrigated with NaOCl 5,25%.
4. While it was disinfecting, the main canal was accessed.
5. The main root canal was shaped using rotary files.
6. Irrigation was done in both root canal spaces with NaOCl 5,25% and EDTA 17% both ultrasonically activated.
7. The main root canal was obturated using modified warm vertical compaction.
8. The perforation/resorption site was filled with bioceramic putty material.
9. Direct restorations were performed on both openings.
Currently the patient is pain free. Waiting for recall.
Conclusions
Anatomical variations continue to represent one of the greatest challenges in endodontics. While additional canals and unusual root configurations are well documented, developmental anomalies such as gemination remain exceptionally rare, particularly in mandibular premolars. Their unpredictable internal anatomy demands careful diagnosis and a tailored treatment strategy. CBCT, magnification and contemporary endodontic techniques are mandatory for achieving a successful clinical outcome.
Bibliography
1. Aryanpour S, Bercy P, Van Nieuwenhuysen JP. Endodontic and periodontal treatments of a geminated mandibular first premolar. Int Endod J. 2002 Feb;35(2):209-14. doi: 10.1046/j.1365-2591.2002.00464.x. PMID: 12019492.
2. James EP, Johns DA, Johnson K, Maroli RK. Management of geminated maxillary lateral incisor using cone beam computed tomography as a diagnostic tool. J Conserv Dent. 2014 May;17(3):293-6. doi: 10.4103/0972-0707.131810. PMID: 24944458; PMCID: PMC4056406.
3. Badole GP, Shenoi PR, Parlikar A. Endodontic management of central incisor associated with large periapical lesion and fused supernumerary root: a conservative approach. Restor Dent Endod. 2018 Oct 26;43(4):e44. doi: 10.5395/rde.2018.43.e44. PMID: 30483468; PMCID: PMC6237732.