
The power of Bioceramics: Management of a Large Periapical Lesion Using Bioceramics material. A Non-Surgical Approach
09/06/2026
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
The management of large periapical lesions in teeth with immature or enlarged apical foramina remains one of the most challenging scenarios in endodontic practice. In such cases, conventional obturation techniques may fail to achieve an adequate apical seal due to the absence of a natural apical constriction.
Mineral Trioxide Aggregate (MTA) and other bioceramic materials have emerged as reliable alternatives for apical barrier formation, owing to their excellent sealing ability, superior biocompatibility, and bioactive properties.
The apical plug technique provides a predictable artificial apical barrier, allowing effective three-dimensional obturation of the remaining canal space while promoting favorable healing outcomes
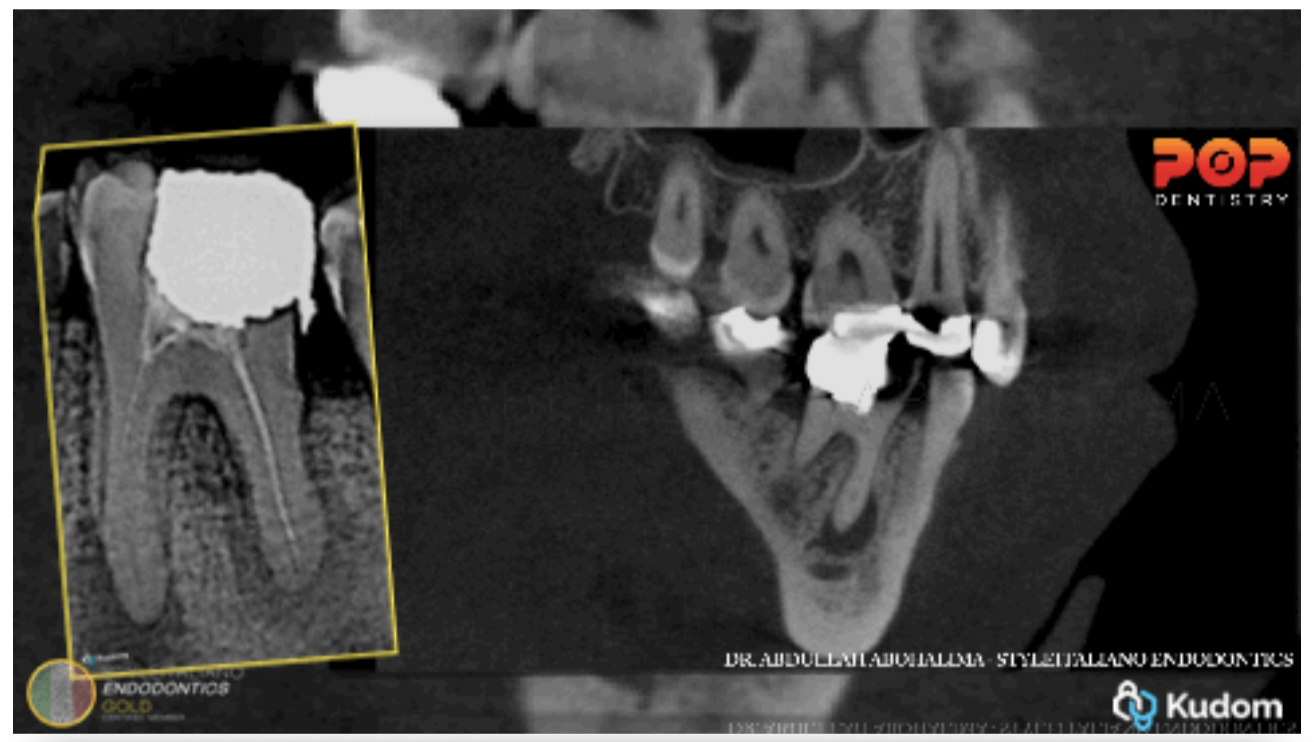
Fig. 1
CBCT evaluation revealed a very large lesion surrounding the mesial and distal root, extending into the furcation area.
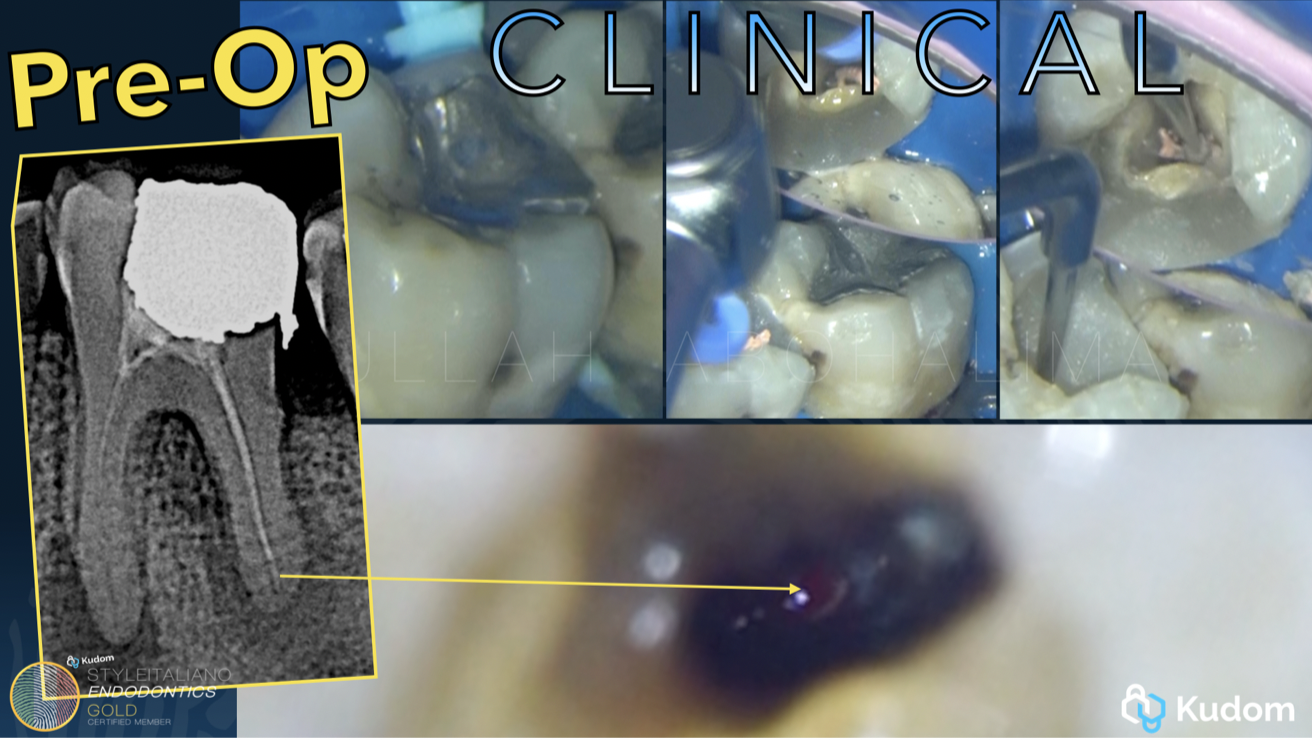
Fig. 2
Coronal disassembly was carried out with removal of the existing amalgam restoration, followed by a pre-endodontic build-up. Previous gutta-percha was removed to facilitate adequate retreatment procedures.
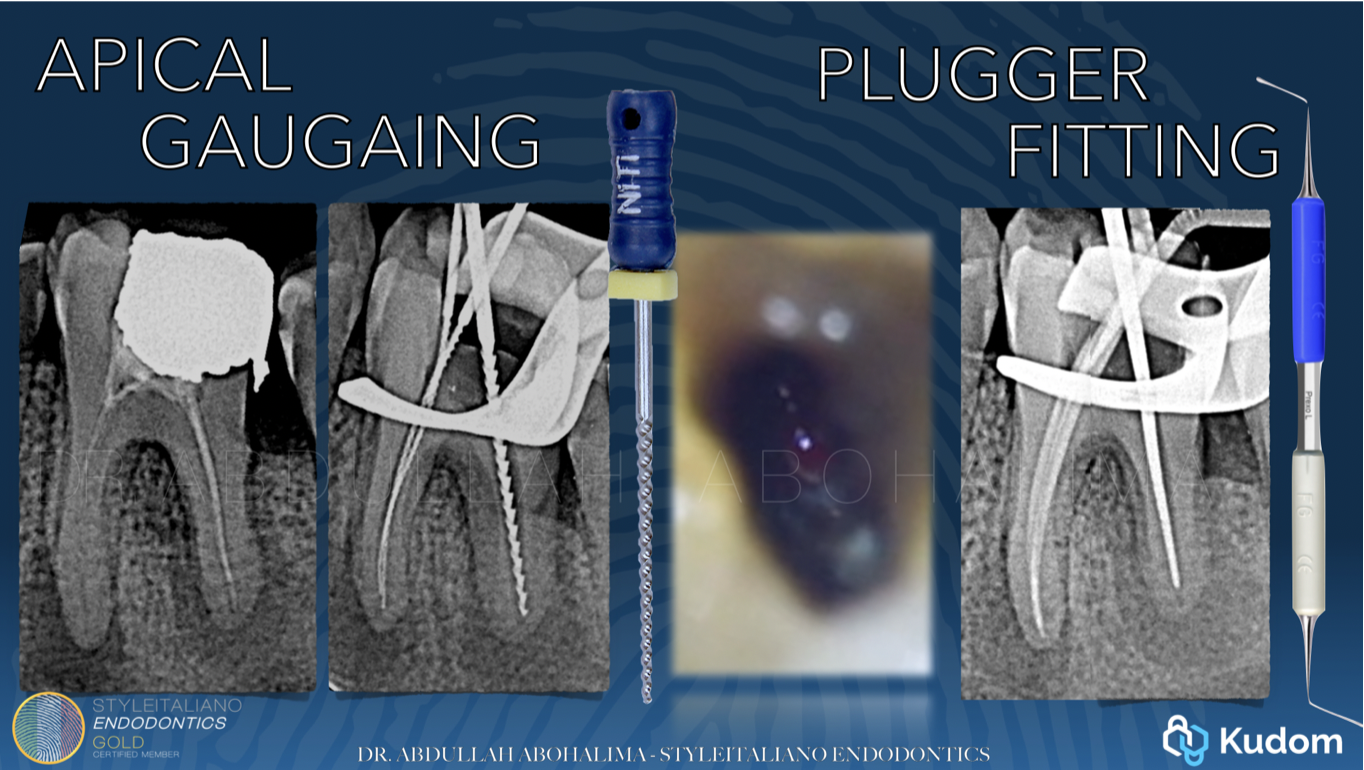
Fig. 3
Working length determination and apical gauging revealed an enlarged apical foramen corresponding approximately to ISO size #60, indicating loss of a natural apical constriction.

Fig. 4
Based on current evidence supporting the superior sealing ability and bioactivity of bioceramic materials compared to conventional gutta-percha–based obturation, an apical plug technique using bioceramic putty was selected.
Step-by-step protocol for a Bioceramic Putty Apical Plug
Under magnification, the apical foramen was clearly visualized.
After completion of the irrigation protocol, a collagen matrix was used as an apical barrier to prevent extrusion of the biomaterial. In some cases, a collagen matrix is required to help control the placement of the material and prevent extrusion. In other cases, I prefer not to use it in order to allow direct contact between the bioceramic material and the periapical tissues. This decision mainly depends on the size of the apical foramen or lesion, where precise control of the material is essential to achieve an optimal seal
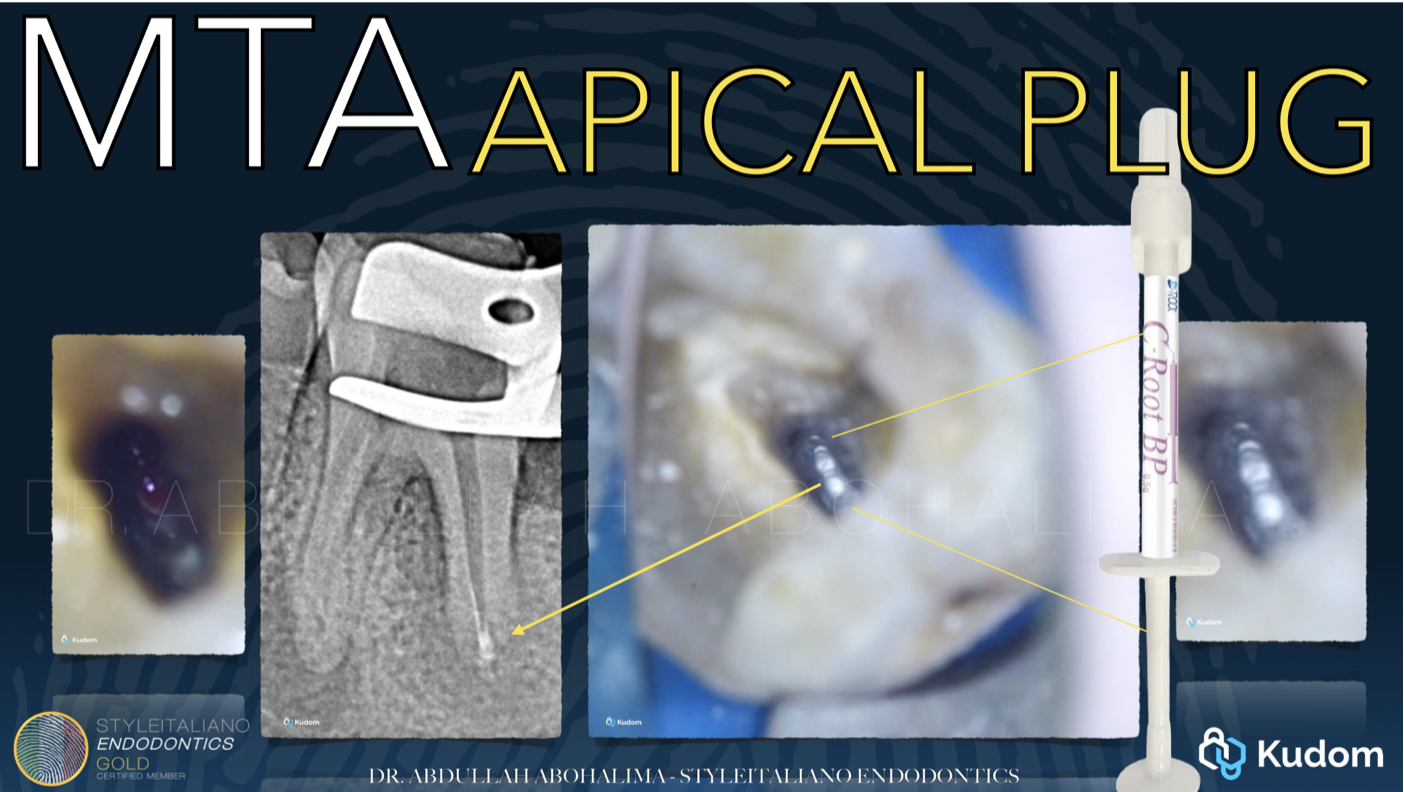
Fig. 5
C-Root Bioceramic putty was delivered using a MAP system and carefully adapted to the apical region. A modified gutta-percha cone, trimmed 3 mm short of the working length, was used as a plugger to achieve controlled compaction of the material.
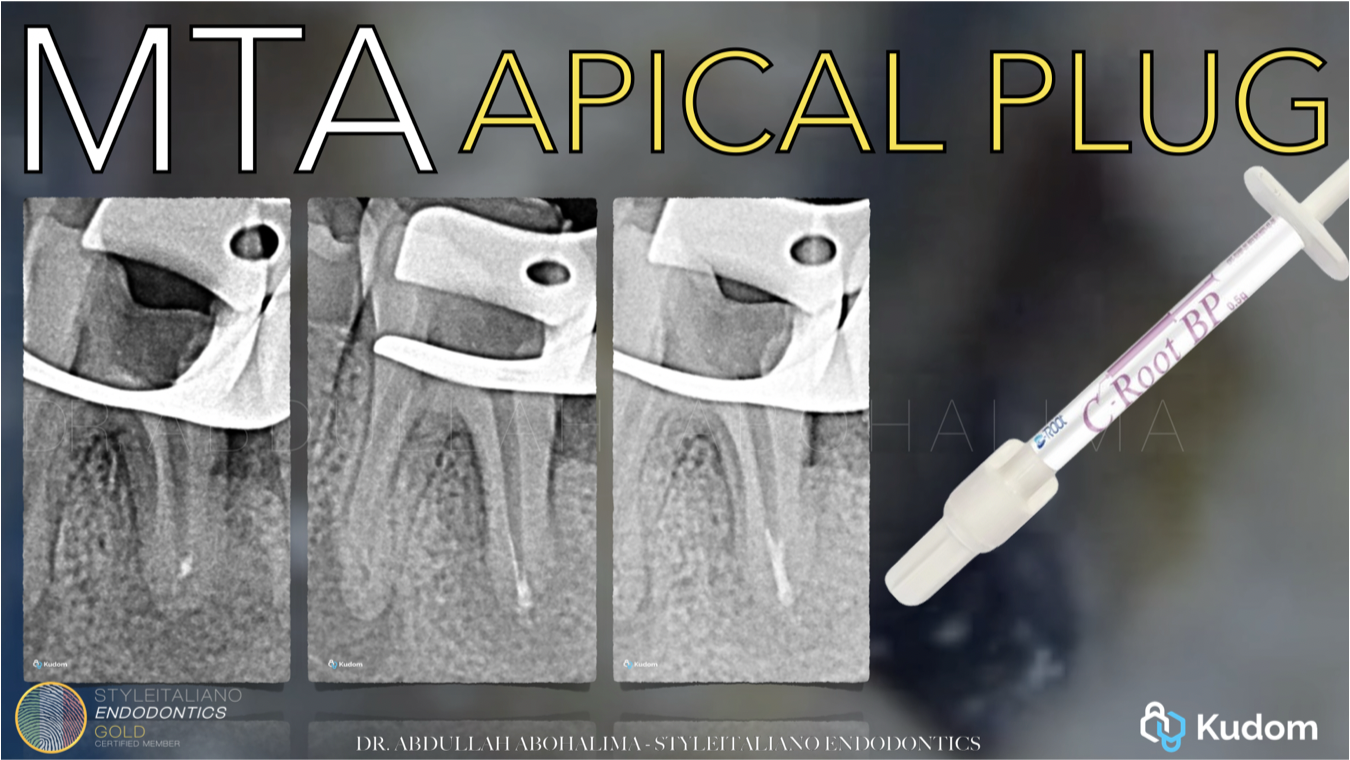
Fig. 6
Radiographic evaluation confirmed proper positioning and adaptation of the C-Root bio ceramic putty apical plug
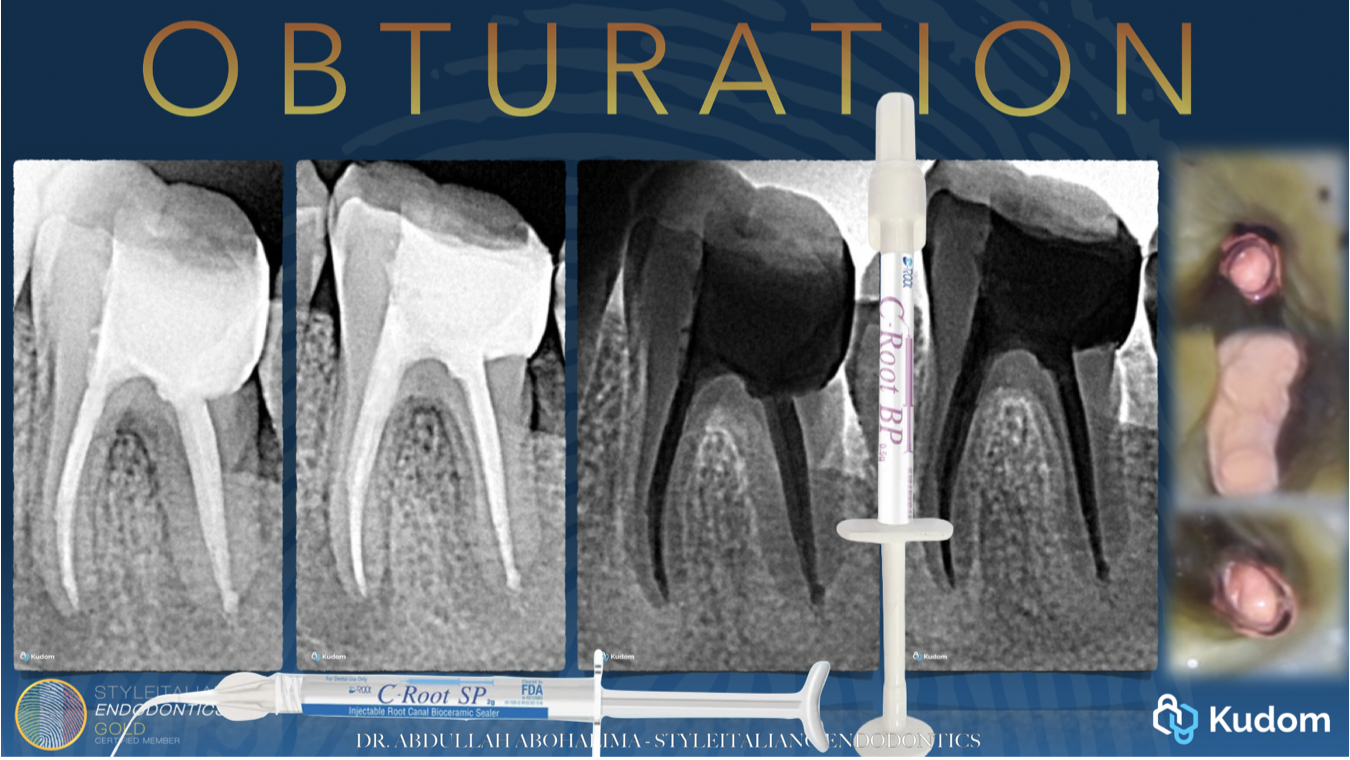
Fig. 7
Once a stable apical barrier was established, C-Root bioceramic sealer was applied, followed by backfilling with thermoplasticized gutta-percha using a backfill device to complete obturation of the remaining canal space.
At follow-up, CBCT evaluation revealed complete healing of the periapical lesion, with axial and sagittal views confirming marked bone regeneration and re-establishment of normal periapical architecture.
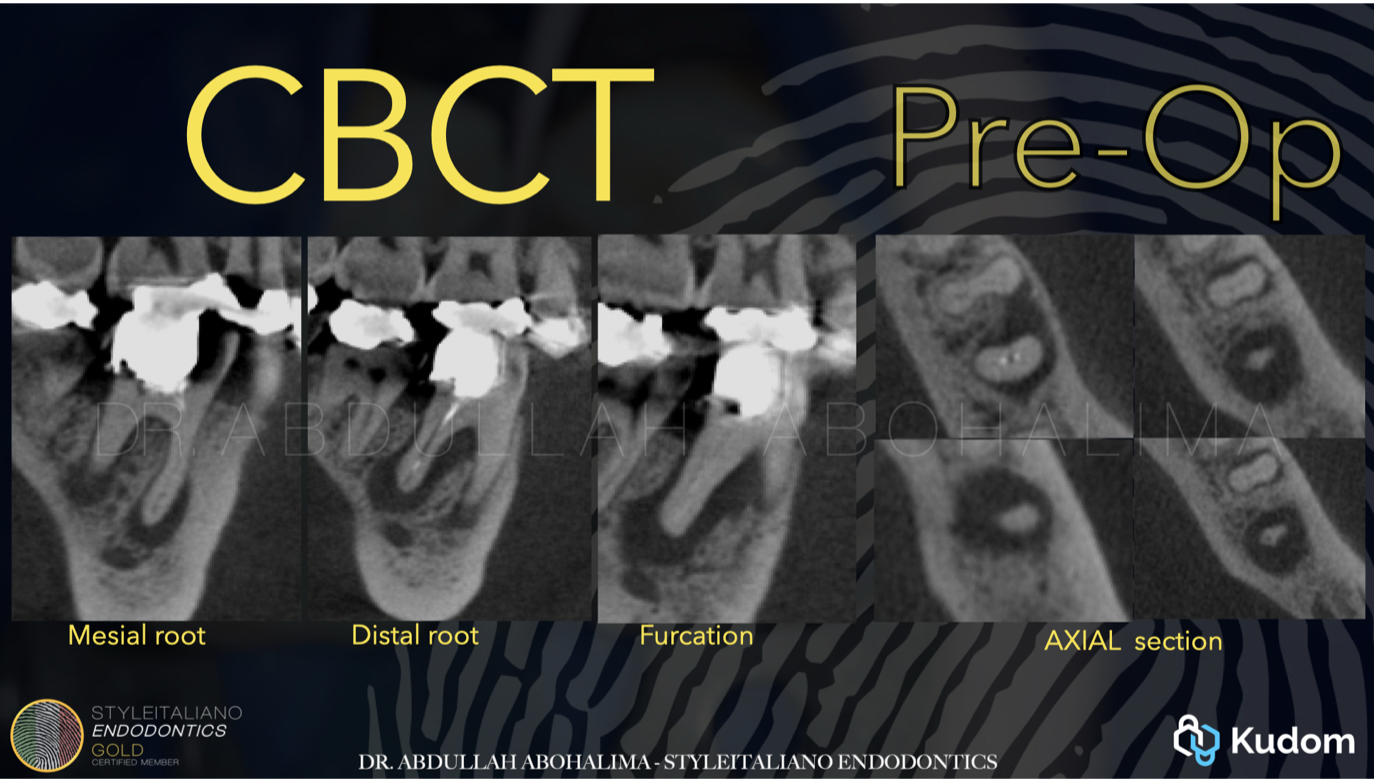
Fig. 8
CBCT before
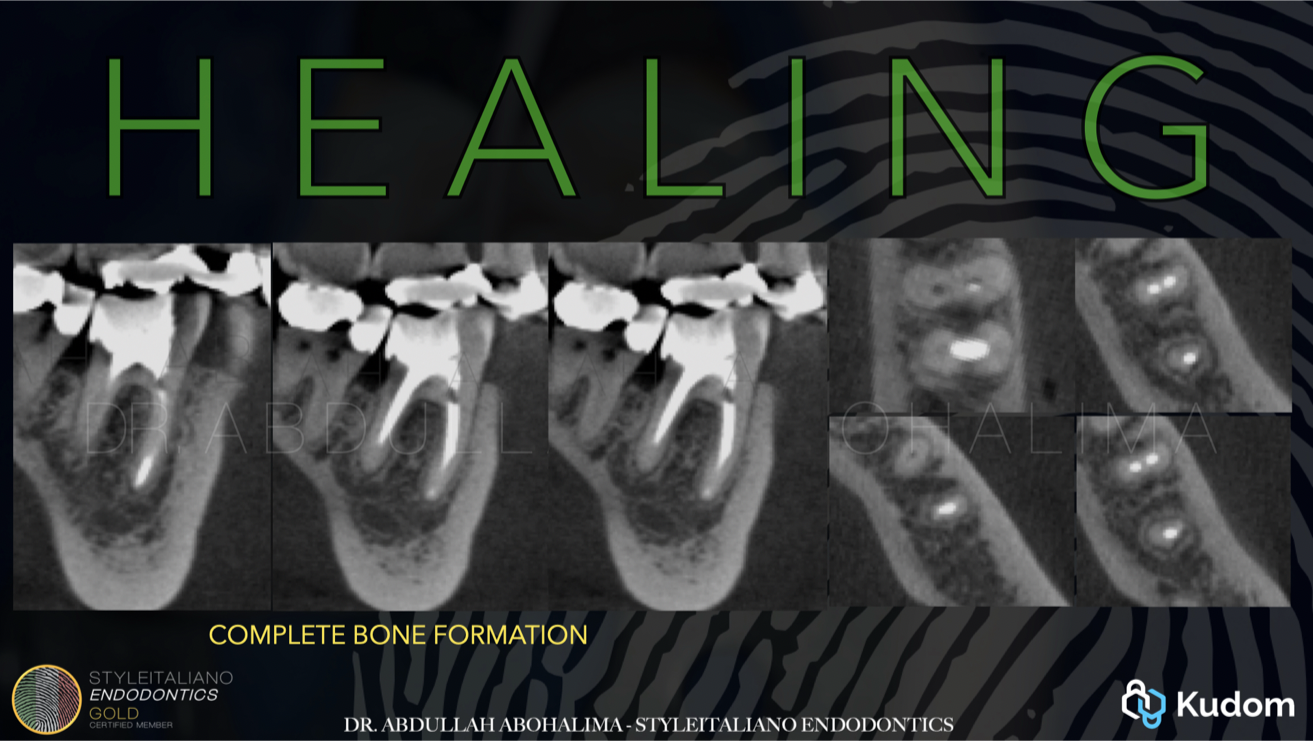
Fig. 9
CBCT after healing
Conclusions
This case demonstrates the clinical effectiveness of bioceramic materials in the management of teeth presenting with large periapical lesions and compromised apical anatomy.
Bioceramic materials not only provide a predictable apical seal but also exhibit bioactive properties that promote periapical healing and bone regeneration. These properties contribute to favorable long-term outcomes, particularly in cases where conventional obturation techniques are limited by the absence of an apical constriction.
Bibliography
- Torabinejad M, Corr R, Handysides R, Shabahang S. Outcomes of nonsurgical retreatment and endodontic surgery: a systematic review. J Endod. 2009;35(7):930-937. DOI: 10.1016/j.joen.2009.04.023.
- Sabeti M, Chung YJ, Aghamohammadi N, et al. Outcome of Contemporary Nonsurgical Endodontic Retreatment: A Systematic Review of Randomized Controlled Trials and Cohort Studies. J Endod. 2024;50(4):414-433.
- Torabinejad M, Chivian N. Clinical applications of mineral trioxide aggregate. J Endod. 1999;25(3):197-205. DOI: 10.1016/S0099-2399(99)80142-3.
- Parirokh M, Torabinejad M. Mineral trioxide aggregate: a comprehensive literature review—Part III: Clinical applications, drawbacks, and mechanism of action. J Endod. 2010;36(3):400-413.
- Torabinejad M, Parirokh M. Mineral trioxide aggregate: a comprehensive literature review—Part II: Leakage and biocompatibility investigations. J Endod. 2010;36(2):190-202. DOI: 10.1016/j.joen.2009.09.010.
