
Minimally Invasive Management of External Cervical Resorption Avoiding Root Canal Treatment
21/05/2026
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
External cervical resorption (ECR) presents a complex clinical challenge, traditionally managed with varying degrees of intervention ranging from surgical repair to extraction. The case of this patient with a history of early orthodontic treatment involving a URA appliance, offers an instructive example of how treatment paradigms can evolve toward minimally invasive principles. This presentation critically examines the shift from an initial consultant's recommendation favouring root canal treatment to an alternative conservative approach prioritising pulp preservation. Radiographic imaging of ECR cannot be based solely on intraoral 2D imaging and CBCT imaging is justified and recommended, based on ALARA principles (Vaz de Souza et al., 2017) The patient was originally assessed by an endodontist for suspected resorptive lesions affecting the upper right anterior region (UR1, UR3, UR4). Notably, the patient reported being entirely asymptomatic, with no history of dental trauma despite a documented mesial incisal coronal fracture of UR1.
The initial consultant's clinical examination revealed:
- Normal percussion responses across all three teeth
- UR1 slightly hyper-responsive to cold (interpreted as possible early irreversible pulpitis)
- UR3 demonstrating a detectable palatal ECR defect on probing
- UR1 with a mesio-buccal defect, though largely non-accessible to probing as later revealed to be mostly interproximal.
Radiographic and CBCT findings classified the lesions using the Patel 3D classification: UR1 as 3Cp (resorption likely extending into the pulp with distal-palatal involvement), UR3 as 2Ad (coronal resorption with no apical lesion), and UR4 as 1Ad (shallow notch defect).(Patel et al., 2017)
The initial management recommendations were notably interventional:
- UR3: Root canal treatment followed by surgical repair via lingual approach
- UR4: Surgical repair alone (no pulpal involvement)
- UR1: Either surgical repair with root canal treatment or extraction with implant placement
This approach, while clinically defensible, committed the patient to endodontic treatment for UR1 and UR3 despite the absence of pulpal symptoms and the teeth's normal response to sensibility testing.
The Shift in Philosophy: Alternative Minimal Invasive Plan
The patient asked for a second opinion. The alternative management strategy was changed representig a deliberate departure from the initial proposal. The core principle underpinning this shift was the preservation of pulp vitality wherever possible, recognising that:
1. All three teeth demonstrated no periapical pathology on CBCT
2. The pulp was not breached in UR3 and UR4, with persistent visible periodontal ligament space
3. UR1 showed Class 3Cp resorption but remained asymptomatic with normal cold response (not hyper-responsive as initially reported – the alternative assessment notes a normal physiological response). A PRRS was still detectable, with an interesting deviation of the canal trajectory towards the palatal aspect as visible on the palatal aspect.
4. No apical periodontitis was detected on CBCT
The alternative plan was altered to carry out no RCT initially: managing potential pulpal exposure with VPT approach with an hydraulic cement – a significant departure from the prophylactic root canal treatment previously recommended for UR1 and UR3.
Clinical Reasoning for the Conservative Approach
The Biological Rationale
The decision to avoid elective root canal treatment rests on several pillars. First, the resorptive process in ECR is inherently extra-canal – it originates in the periodontal ligament and invades root dentine progressively. The pulp may remain uncompromised for extended periods, particularly in Class 1 and 2 lesions (Patel et al., 2018). Second, sensibility testing, while imperfect, provides useful guidance: normal responses in UR3 and UR4, and even UR1's normal response (contradicting the initial report of hyper-responsiveness), suggested pulp vitality that merited preservation. The patient agreed to later carry out root canal treatment if symptoms were to precipitate.
Third, the emerging evidence base for vital pulp therapy (VPT) in the context of resorptive defects has strengthened the rationale for conservative management. Hydraulic cements offer excellent sealing properties, biocompatibility, and the capacity to promote reparative dentine formation when pulp exposure occurs intraoperatively.
Risk-Benefit Reassessment
The initial consultant appropriately warned of aesthetic risks: papilla loss, gingival recession, and interproximal bone loss affecting long-term soft tissue outcomes. However, the alternative plan recognised that committing to root canal treatment introduces additional risks without clear benefit in an asymptomatic, normally responsive tooth. The advice given to the patient explicitly acknowledged risk of endodontic treatment in case of symptoms in particular on UR1.

Fig. 1
Intraoral long-cone periapical x-ray showing ECR on the UR3 and UR4.
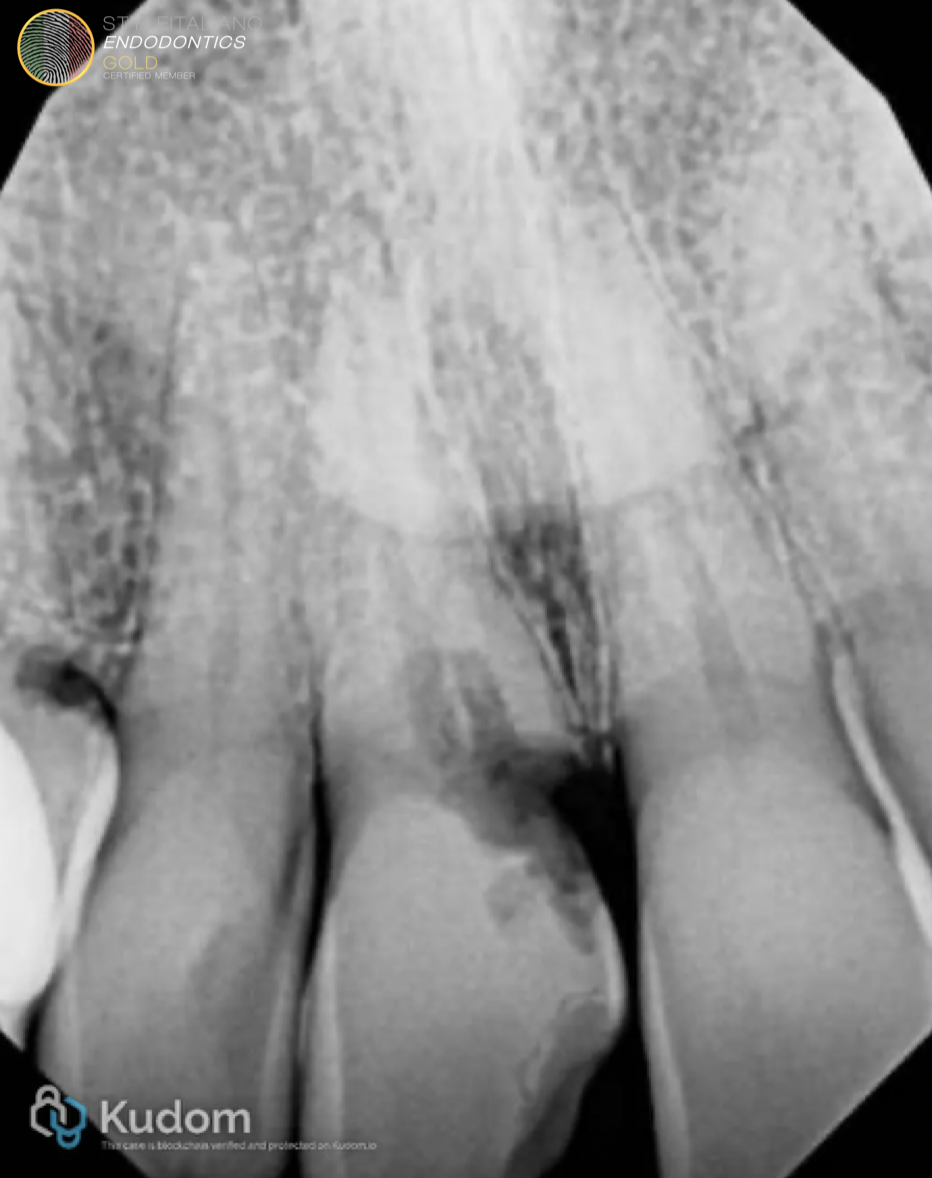
Fig. 2
Intraoral long-cone periapical x-ray showing ECR on the UR1.

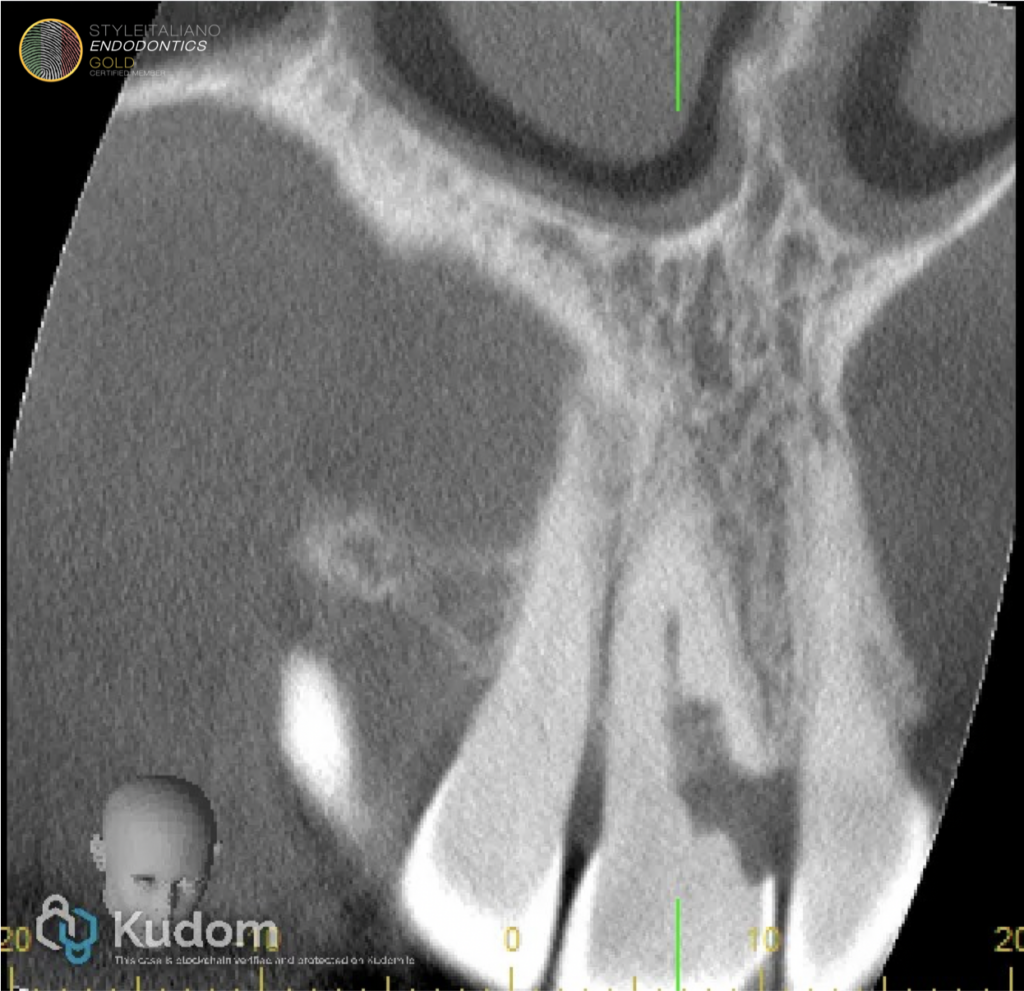
Fig. 3
UR1 extensive ECR resorption infrabony in nature and with probable involvement of the pulp as per CBCT imaging as per frontal view

Fig. 4
The sagittal view reveals a palatal displacement of the canal with a preserved Pericanalar Resorption-Resistant Sheet (PRRS) on the UR1 with absence of periapical lesion.
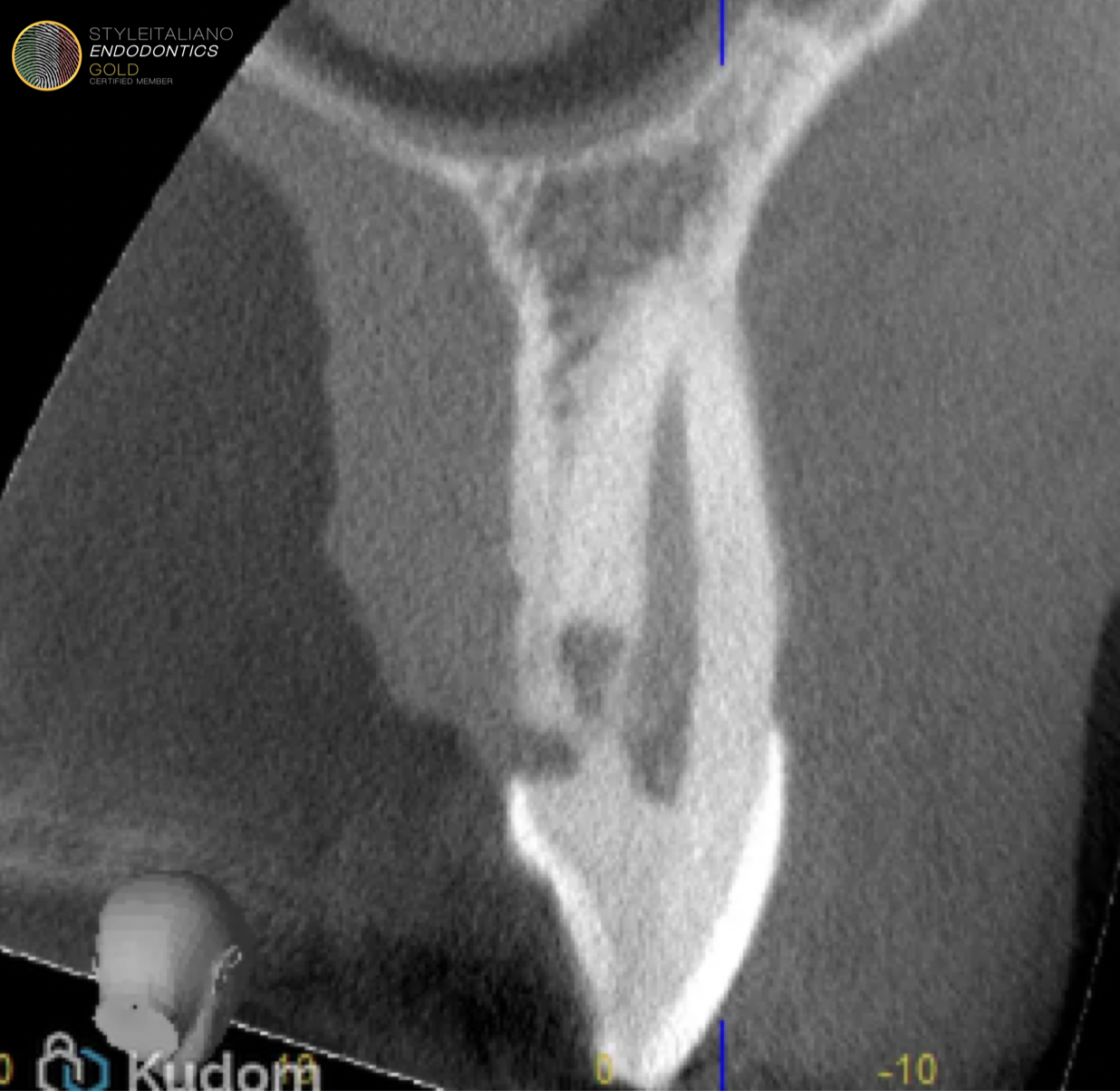
Fig. 5
Sagittal view on small FOV CBCT of the palatal lesion on the UR3. No periapical lesion present and no direct pulpal involvement.
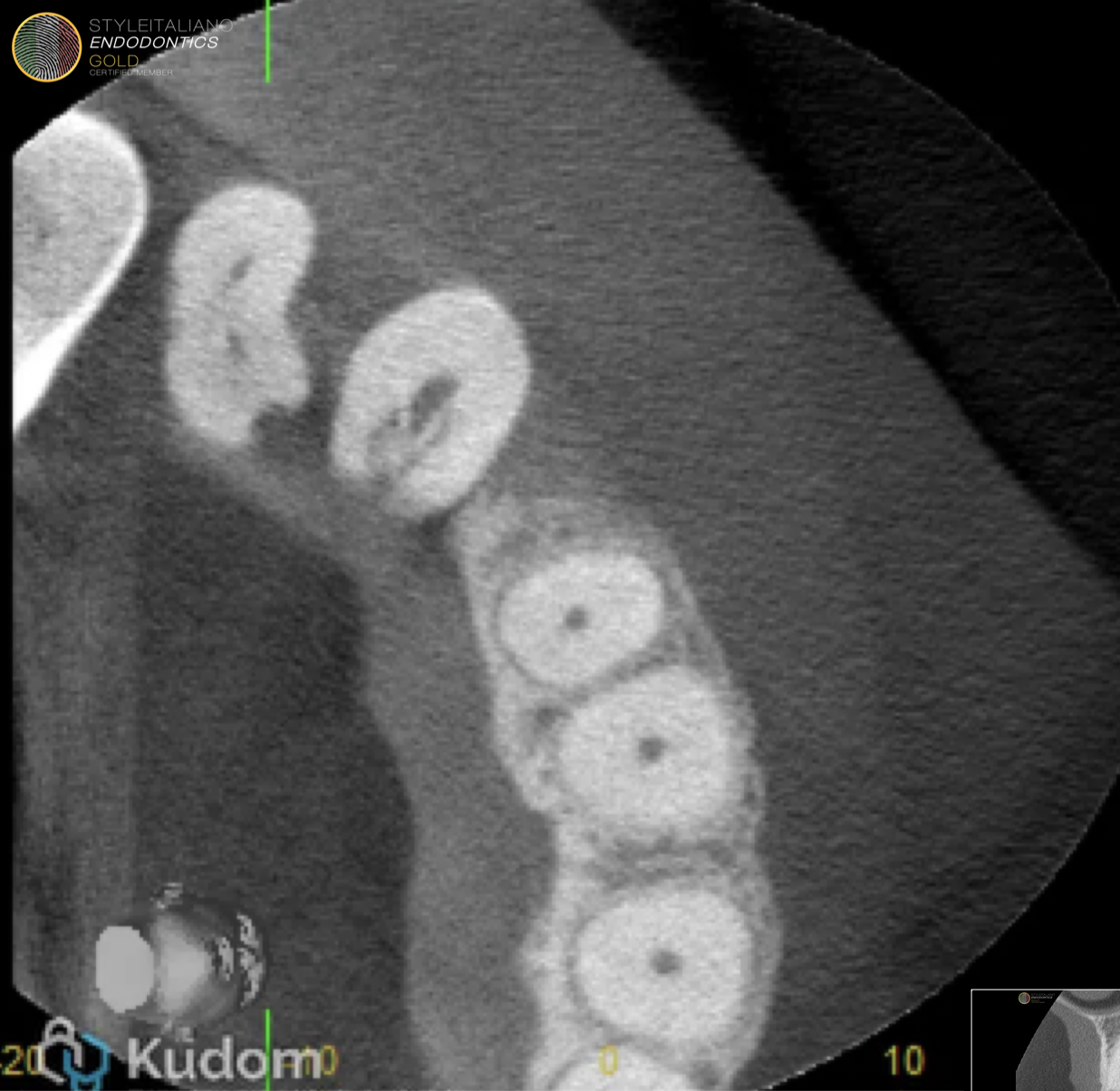
Fig. 6
Coronal view of the small fov CBCT showing the small notch incipient lesion on the UR4 together with the paltal lesion on the UR3.

Fig. 7
Preoperative clinical photograph showing the bleeding on probing associated with the interproximal ECR.
Treatment Sequence and Technical Execution
UR1 Repair: Buccal Approach
The first procedure addressed UR1, the most advanced lesion (3Cp). Under rubber dam isolation, a buccal flap was raised, and the resorptive defect was accessed. Following removal of inflammatory tissue, pulp capping with hydraulic cement was performed, followed by composite restoration. This approach successfully avoided root canal treatment despite the lesion's radiographic extension into the pulp – the key being that the pulp remained vital and responsive, allowing a vital pulp therapy rather than extirpation.

Fig. 8
Open Flap rubber dam placement and restoration in situ. This techinique can maximise the vital pulp therapy outcome minimising pulp contamination.

Fig. 9
Postoperative x-ray of the external repair in composite with direct pulp capping to carry out a vital pulp therapy approach
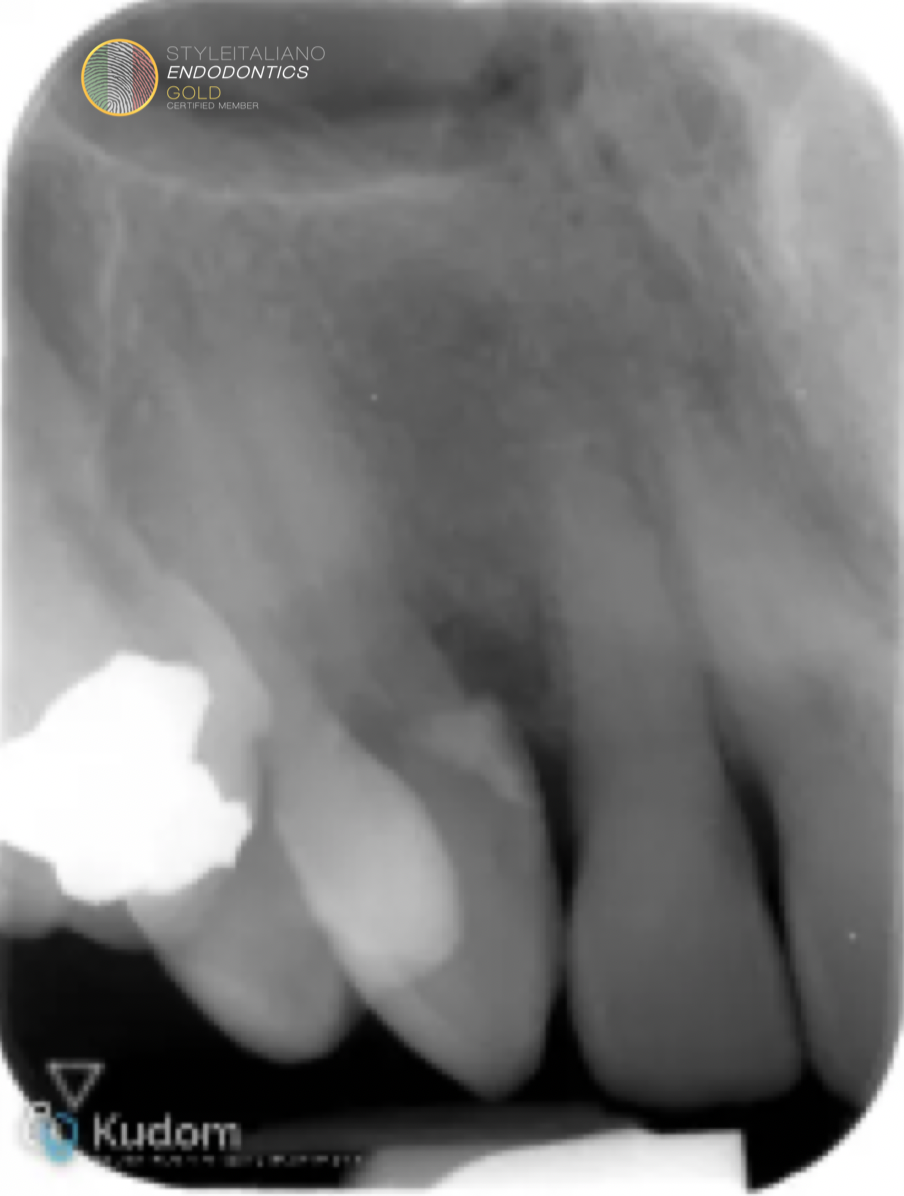
Fig. 10
LCPA showing the exernal repair executed with GIC on UR3 and UR4.
UR3 and UR4 Repair: Palatal Envelope Flap
A subsequent procedure addressed UR3 and UR4 simultaneously via a palatal envelope flap approach. For UR3, following inflammatory tissue removal, Hydraulic cement was placed as the repair material. Notably, for UR3 and UR4 (a shallow 1Ad lesion), glass ionomer cement (GIC) was utilised due to practical limitations: the inability to achieve ideal isolation and limited moisture control. This pragmatic material selection demonstrates clinical adaptability. GIC's moisture tolerance and fluoride release make it a reasonable alternative when ideal conditions cannot be achieved.
Post-operative Outcomes
Follow-up review demonstrated:
- Good healing overall
- The UR1 area showed mild inflammation at the papilla base incision distal to UR1 with minimal bleeding
- Pulp status confirmed as normal on UR1
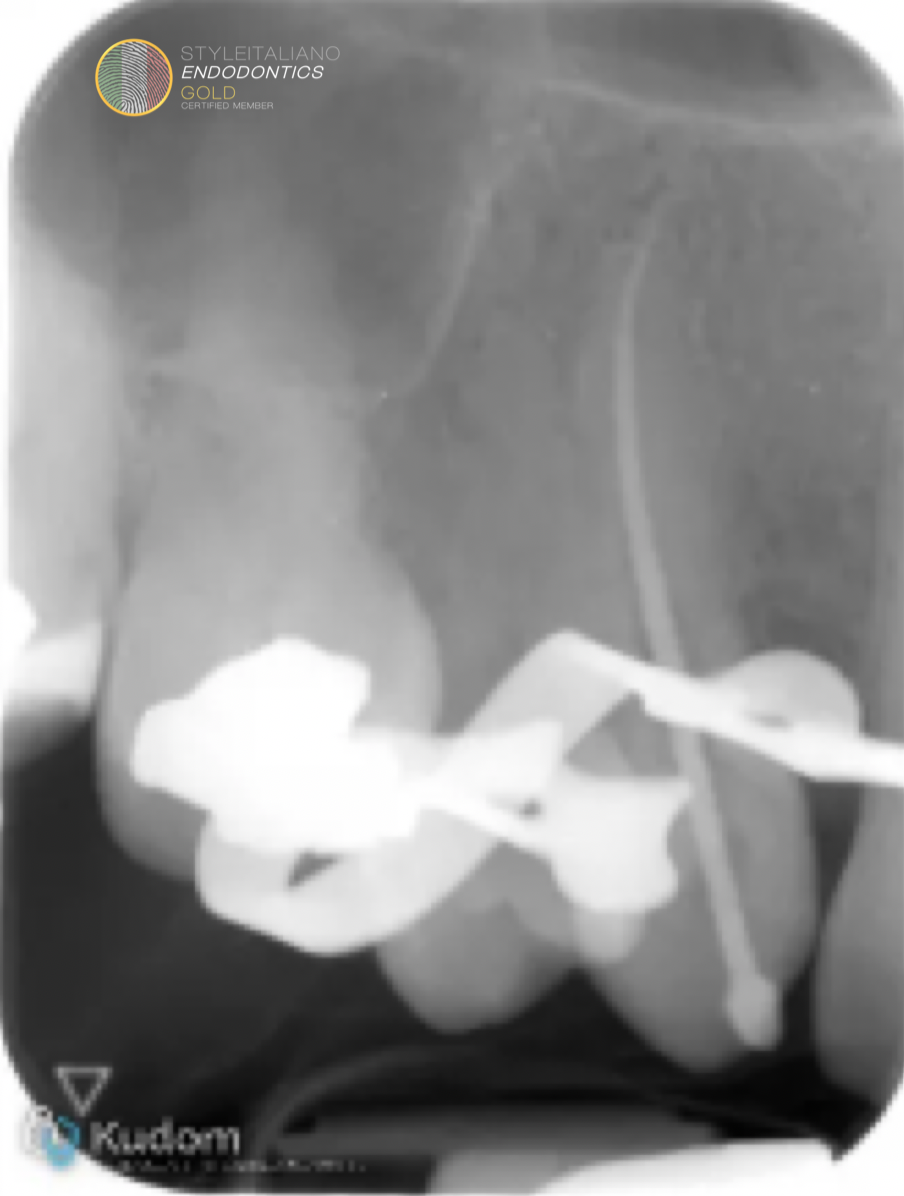
Fig. 11
Intraoperative xray of master apical cone on UR3.
Two months following the external repair the UR3 started to develop symptoms of irreversible pulpitis with pain on clinostatism. Root canal treatment on the UR3 was carried out in a single visit.
The UR1 remains vital at the 9 months’ review.

Fig. 12
Postoperative xray showing the completed RCT on UR3.
Conclusions
This case raises important questions about the threshold for recommending root canal treatment in ECR. The initial consultant's approach – advocating RCT for UR3 (a Class 2 lesion with no pulpal involvement) and for UR1 (despite normal pulpal status) – reflects a traditional, perhaps overly cautious, philosophy. The assumption appears to be that pulpal involvement is inevitable or that access for repair necessitates pulpectomy.
Yet the alternative approach demonstrates that:
1. Even Class 3 lesions (3Cp) may permit vital pulp therapy rather than complete extirpation
2. Patient-reported outcomes (avoiding unnecessary endodontics) align with biological plausibility
The literature increasingly supports this position. Patel and colleagues have emphasised that the 3D classification should guide treatment but not mandate RCT for all lesions reaching the pulp. The critical distinction is whether the pulp is necrotic or irreversibly inflamed versus merely exposed but vital.
Limitations and Caveats
A balanced discussion must acknowledge the limitations of the conservative approach. The follow-up period documented is short-term; long-term monitoring is essential to confirm pulp vitality maintenance and absence of resorption progression. The use of GIC for UR3 and UR4, while pragmatic, may not provide the same long-term seal as composite, though the shallow nature of the lesion (1Ad) mitigates this concern.
The UR3 that seemed to be the least involved compared to the UR1 ended up requiring a root canal treatment, this may indicate that the VPT was far more effective in the presence of an appropriate isolation or other factor including type of material to seal the biomaterial (GIC vs composite)
Conclusion
This case presentation illustrates that external cervical resorption can be successfully managed using minimally invasive techniques that prioritise pulp preservation. With an easier fall-back plan with conventional access root canal treatment. The first line of treatment avoiding prophylactic root canal treatment and employing vital pulp therapy with hydraulic cements,
The contrast between the initial consultation's recommendations (RCT for UR3 and UR1, with implant discussion) and the actual treatment delivered following the request for a second opinion (no initial RCT, VPT where needed) highlights an evolving philosophy in managing ECR. When the pulp responds normally, is free of apical pathology, and the resorptive defect can be adequately accessed, a trial of vital pulp therapy with appropriate bioactive materials represents a defensible, patient-centred alternative to immediate endodontic intervention. Long-term follow-up will ultimately determine the durability of this approach, but the immediate outcomes are encouraging.
Bibliography
Vaz de Souza D, Schirru E, Mannocci F, Foschi F, Patel S. External Cervical Resorption: A Comparison of the Diagnostic Efficacy Using 2 Different Cone-beam Computed Tomographic Units and Periapical Radiographs. J Endod. 2017 Jan;43(1):121-125. doi: 10.1016/j.joen.2016.09.08. Epub 2016 Dec 6. PMID: 27939734.
Patel S, Foschi F, Mannocci F, Patel K. External cervical resorption: a three-dimensional classification. Int Endod J. 2018 Feb;51(2):206-214. doi: 10.1111/iej.12824. Epub 2017 Sep 13. PMID: 28746776.
Patel S, Foschi F, Condon R, Pimentel T, Bhuva B. External cervical resorption: part 2 - management. Int Endod J. 2018 Nov;51(11):1224-1238. doi: 10.1111/iej.12946. Epub 2018 Jun 9. PMID: 29737544.



