Why Dual-Cure Cementation Matters for Indirect Composite Restorations in Endodontically Treated Teeth
23/05/2026
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Indirect composite restorations require a luting material that combines reliable adhesion, efficient handling and predictable polymerization, even in areas where light transmission may be limited. A dual-cure resin cement offers a clear clinical advantage: it can be light-activated where access is optimal, while the chemical cure supports polymerization in deeper or less accessible areas. This makes it particularly suitable for inlays, onlays, crowns, veneers and other indirect restorations where complete light penetration cannot always be guaranteed.
A clinical case wil be shown in which a first lower molar with symptomatic irreversible pulpitis and normale periapical tissues was treated endodontically and restored with a build up in the first visit, while in the second visit a composite indirect restoration was luted by means of OverCEM SA by Overfibers.
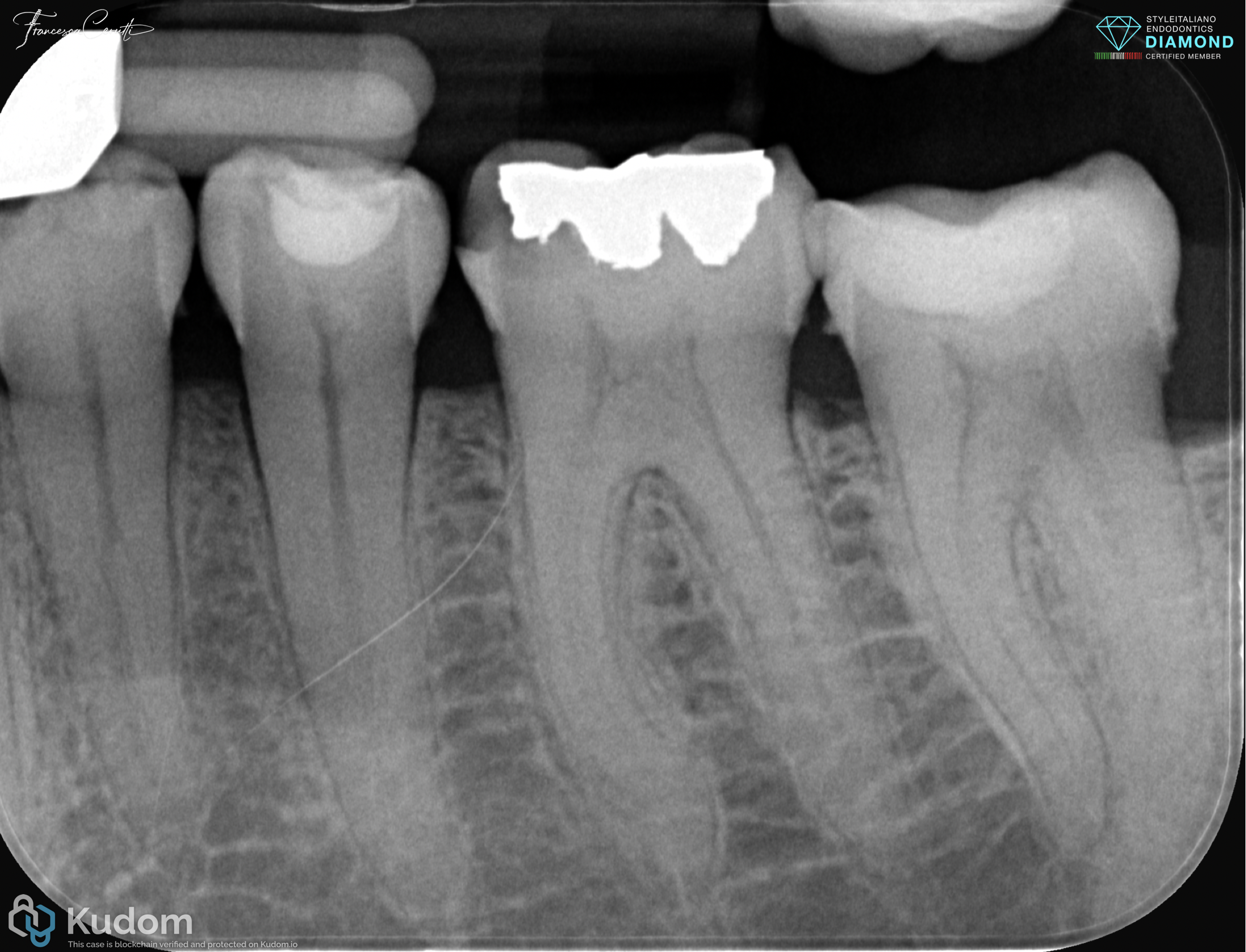
Fig. 1
A 45 years old male patient came to my attention complaining about intense, spontaneous, non subsiding and radiating pain in the lower left hemiarch.
The X-ray showed a defective amalgam restoration on tooth 3.6 for which I planned endodontic treatment and indirect restoration.

Fig. 2
Due to the complexity of the anatomy, I chose to perform the endodontic treatment with a conservative heat-treated reciprocating file system, to irrigate according to my regular protocol and to fill with the single cone and silicate-based hydraulic sealer.
After the core build-up, a scan was taken and the dental technician prepared an indirect restoration.
Video of the procedure

Fig. 3
In order to simplify the workflow and ensuring at the same time excellent clinical performances, I selected OverCEM SA as a luting material.
OverCEM SA is a dual-curing, self-adhesive resin cement. Its self-adhesive formulation eliminates the need for separate etching, primer and adhesive steps on dentin, helping to save chair time and reduce technique sensitivity. The material is indicated for a wide range of substrates, including composites, zirconia, ceramics, lithium disilicate, metals and fiber posts, making it a versatile solution for everyday indirect cementation.
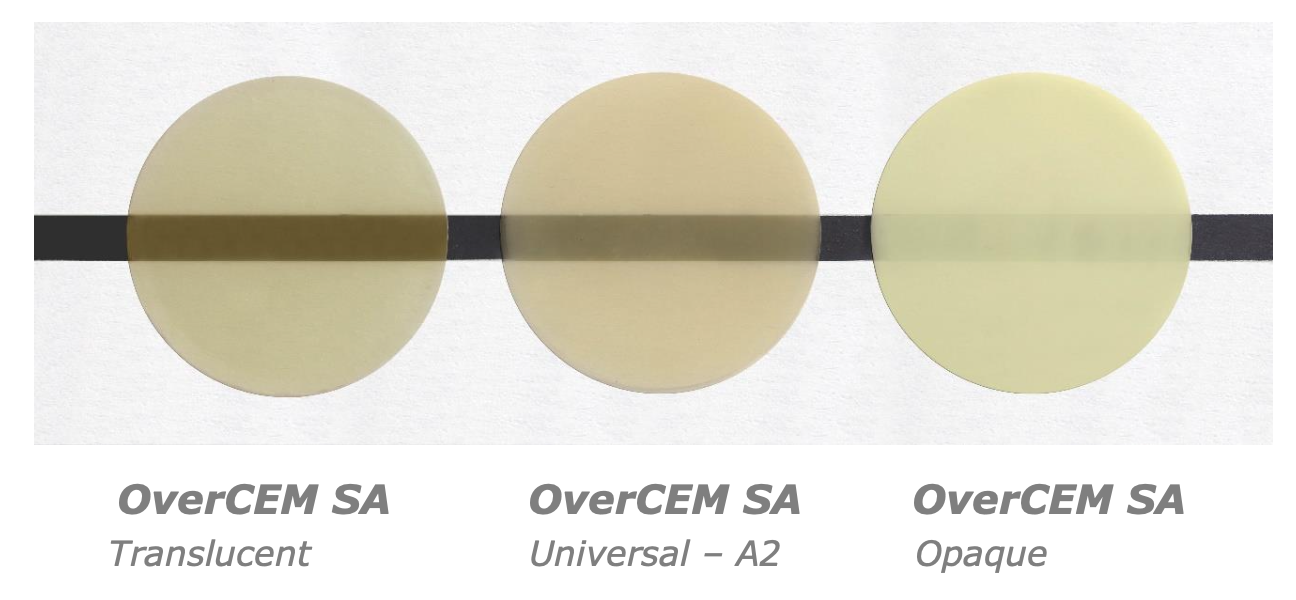
Fig. 4
Since the tooth was not heavily discolored and I wanted a good chromatic adaptation of the restoration to the tooth, I selected the shade Universal.
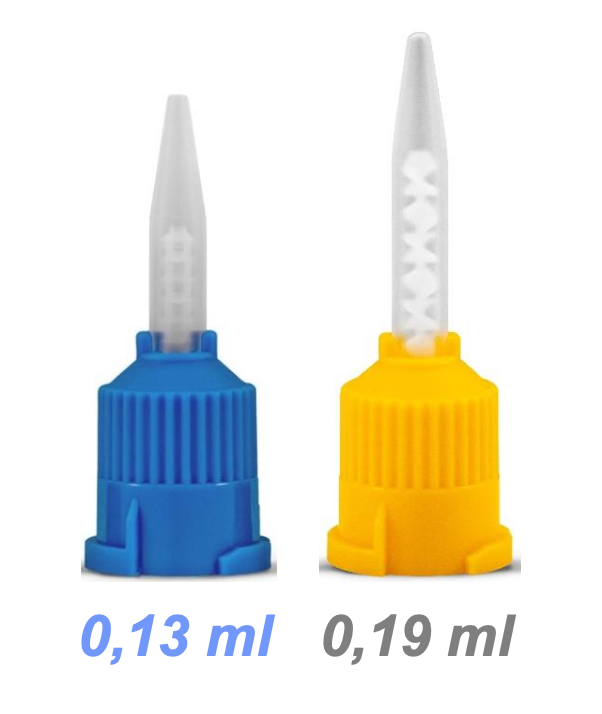
Fig. 5
A key benefit of OverCEM SA is its practical delivery system. The T-Mixer Regular tip is described as the smallest auto-mixing tip on the market, and it reduces cement waste by 30% in volume compared with conventional mixing tips. For indirect composite restorations, this means more precise application, less material loss and improved control during placement.

Fig. 6
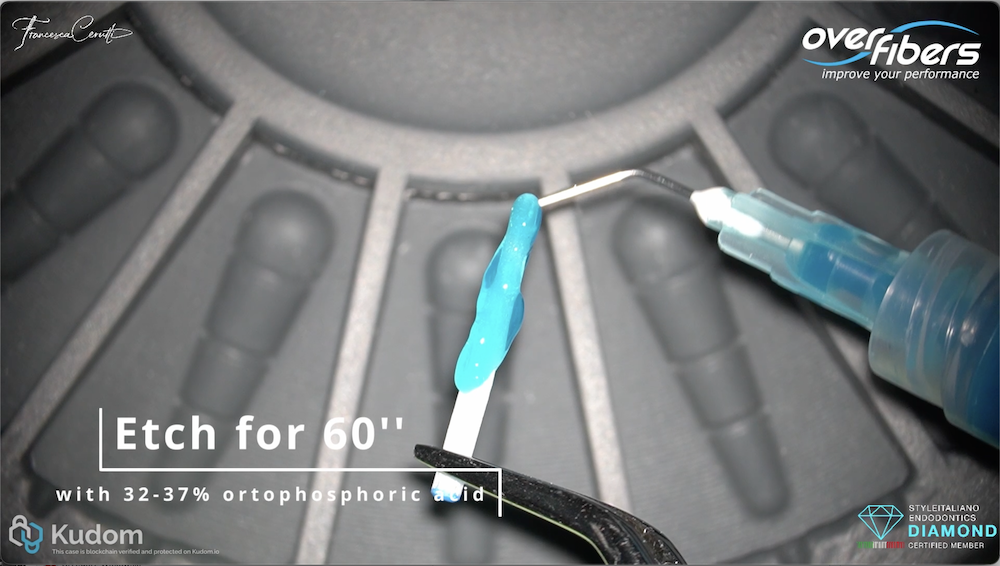
As prescribed, I used 9% hydrofluoric acid gel for 30 seconds to condition the inner surface of the restoration, then I rinsed with a water spray for at least 20 seconds.
Once dried, I applied a silane primer and after 60 seconds I gently air-dried the restoration.
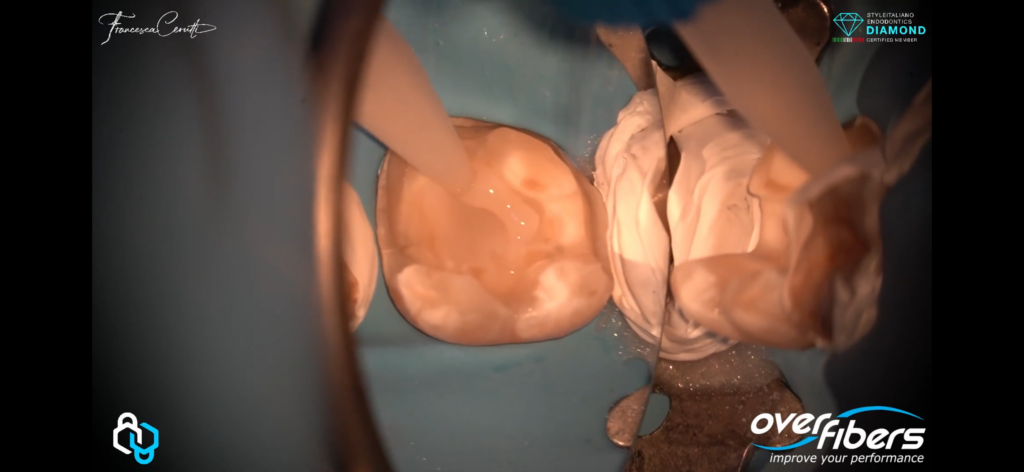
The tooth was isolated with rubber dam, cleaned and then the restoration was luted, as shown in the video.
The key points to carry out a correct cementation procedure are:
- Put a filter on the microscope, if you are using one, since the intensity of the light could start early the polymerization process.
- As a general rule when you use this product, bleed the syring until equal amounts of product are extruded and, after mounting the tip, discard the first drop of material.
- After seating the restoration, wait for 60 seconds before light curing
- The excess cement can be briefly light-cured for 1–2 seconds to reach a gel phase, allowing it to be removed easily with a scaler and dental floss. before final polymerization. This feature is particularly valuable around restoration margins, where fast and controlled clean-up helps preserve precision and reduces finishing time.
- After this, complete the polymerization by light curing each surface of the restoration for at least 20 seconds at >1000mW/cm2.
Conclusions
Overall, OVERCEM SA combines the advantages of dual-cure polymerization with a self-adhesive protocol, a compact low-waste mixing tip and simplified excess removal. For indirect composite restorations, these characteristics support a faster, cleaner and more predictable cementation procedure.
Bibliography
1. Acquaviva P, Cerutti F, Adami G, Gagliani M, Ferrari M, Gherlone E, et al. Degree of conversion of three composite materials employed in the adhesive cementation of indirect restorations: a micro-Raman analysis. J Dent. 2009;37(8):610-5.
2. de Kuijper M, Cune MS, Özcan M, Gresnigt MMM. Clinical performance of direct composite resin versus indirect restorations on endodontically treated posterior teeth: A systematic review and meta-analysis. J Prosthet Dent. 2023;130(3):295-306.
3. Shu X, Mai QQ, Blatz M, Price R, Wang XD, Zhao K. Direct and Indirect Restorations for Endodontically Treated Teeth: A Systematic Review and Meta-analysis, IAAD 2017 Consensus Conference Paper. J Adhes Dent. 2018;20(3):183-94.