Cracked Teeth (CT) and Vertical Root Fractures (VRF)
14/05/2026
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Cracked Teeth (CT) and Vertical Root Fractures (VRF) are common forms of longitudinal tooth fractures encountered in clinical practice. Cracked teeth typically present as thin, incomplete fractures or surface disruption of enamel and dentin, and possibly cementum that originate in the crown with unknown depth or extension. Although described as a “syndrome,” it does not exhibit a consistent pattern of clinical symptoms, making it difficult to diagnose (1).
In contrast, vertical root fractures usually begin within the root and extend coronally, whereby the fractured segments are incompletely separated; it may occur buccal-lingually or mesial-distally; it may cause an isolated periodontal defect(s) or sinus tract; it may be radiographically evident. While a Split Root is a continuation of a crack or vertical root fracture, whereby the fractured segments are completely separated longitudinally (1).
Both conditions pose diagnostic and therapeutic challenges, requiring careful clinical evaluation and appropriate imaging. Early detection is essential for improving treatment outcomes, preserving tooth structure, and selecting the most suitable management approach.
Causes
CTS may result from multiple factors, including parafunctional habits such as bruxism, trauma, and age-related structural changes.
Signs and Symptoms
CTS is associated with a wide range of clinical manifestations that often lack a consistent pattern. The presentation varies depending on the pulpal status: vital, inflamed, necrotic, or root canal treated (2).
Location:
The mandibular first molar is the tooth most frequently affected, followed by the maxillary premolars, maxillary molars, and mandibular premolars. As the first permanent teeth to erupt, mandibular first molars are more susceptible to caries and often undergo multiple restorative procedures, increasing their risk of fracture. In addition, the wedging effect exerted by the prominent mesiopalatal cusp of maxillary first molars (2).
Pain:
Pain is often described as dull and poorly localized, but it may present as the characteristic “rebound pain.”; sharp pain that occurs upon release of biting pressure. Pain is often triggered during intake of fibrous foods due to flexure and subsequent recoil of the fractured cusp, which stimulates nerve fibers within the dentinal tubules through the odontoblastic layer, as well as via hydrodynamic fluid movement inside the tubules (3).
Causes of Vertical Root Fracture (VRF) Occur in root canal treated teeth (5).
- Endodontic Procedures: Excessive force during canal filling (obturation) or using too much pressure with spreaders (lateral condensation).
- Endodontic Posts: The insertion or wedging effect of metal/fiber posts, which can lead to fractures.
- Excessive Tooth Structure Removal: Over-preparation of the canal, reducing the dentin thickness and weakening the root.
- Anatomical Factors: Narrow roots or specific anatomy.
- Post-Treatment Failure: Failure to place a crown immediately after a root canal, allowing the tooth to be exposed to forces it cannot handle.
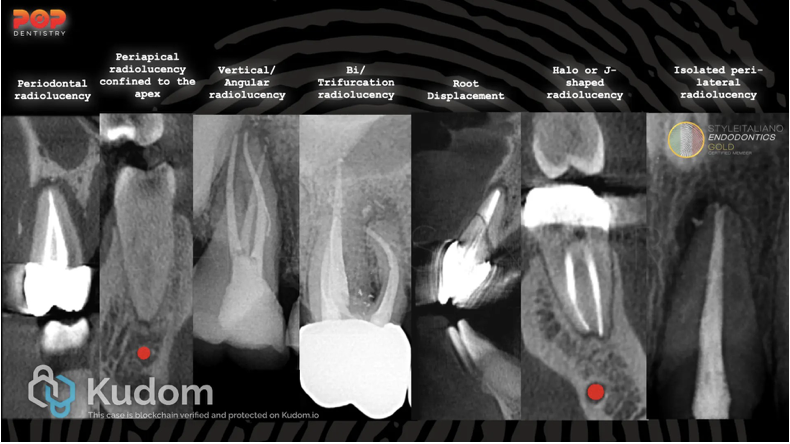
Fig. 1
Radiographic signs of crack and fracture in teeth

Fig. 2
Radiographic Considerations for VRF
The presence of two sinus tracts on both the buccal and lingual aspects are considered a sign for a vertical root fracture. Common features that can be observed from cone beam imaging. These include:
1. Bone Loss in the mid-root area, with intact bone coronal and apical to the defect.
2. Absence of the entire buccal plate of bone.
3. Space between the buccal and lingual plate of the bone and the root surface.
4. Visualization of the vertical root fracture.

Fig. 3
AAE classification of the cracked and fractured teeth (4)
1. Craze line

Fig. 4
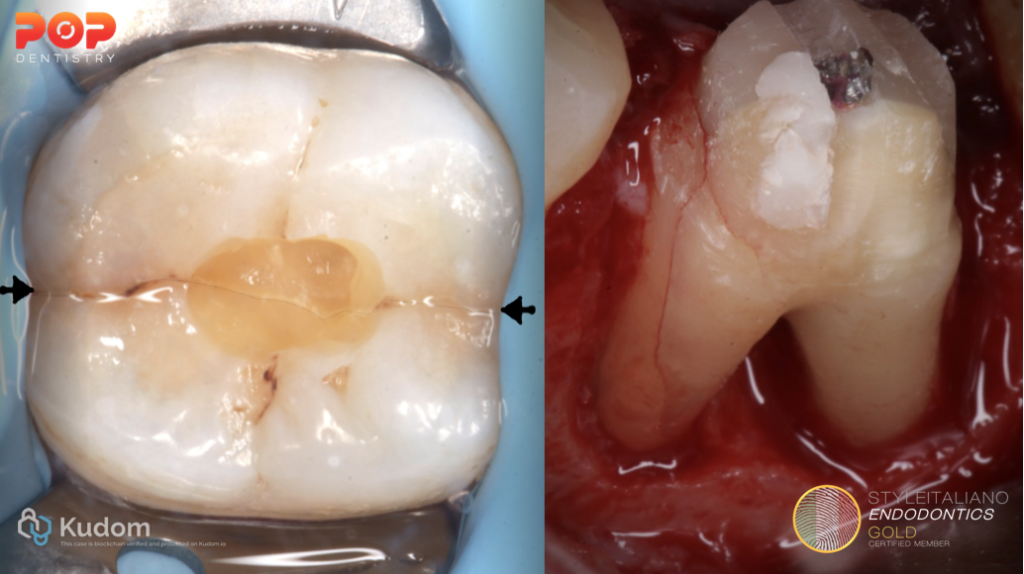
2. Cracked tooth

Fig. 5
3. Fractured Cusp

Fig. 6
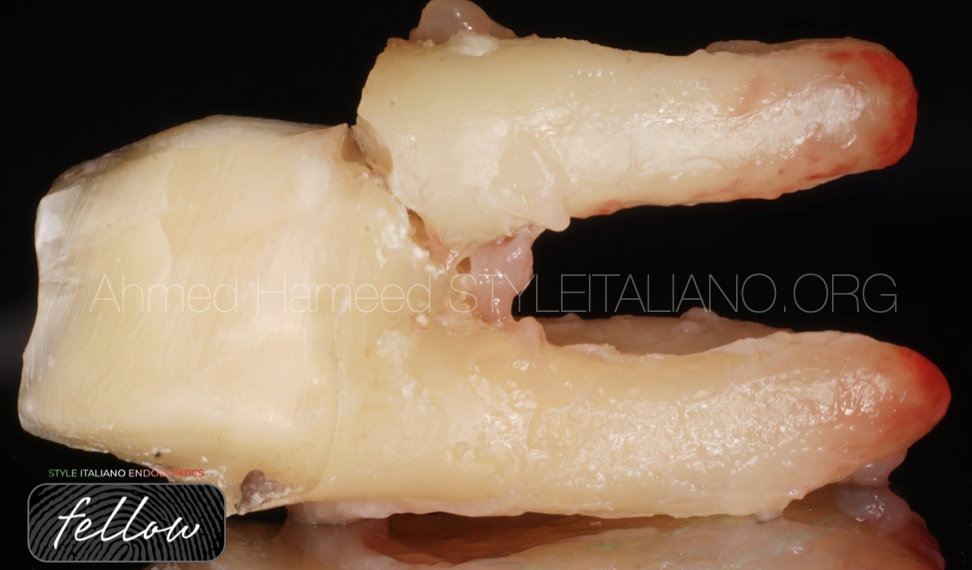
4. Vertical Root Fracture
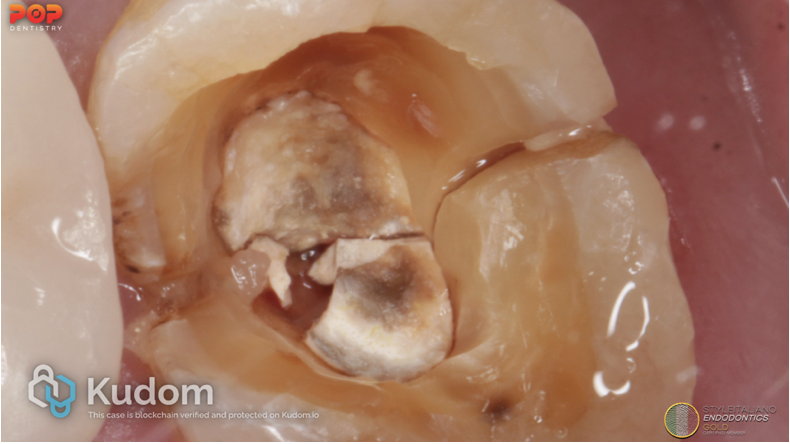
Fig. 7
5. Split Tooth
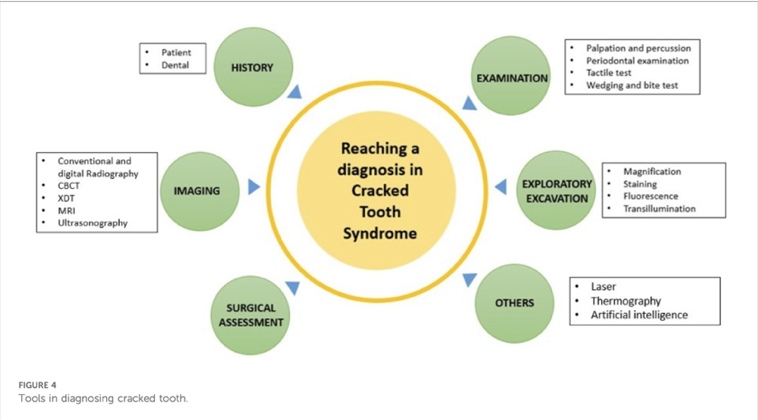
Fig. 8
Diagnosis begins with a thorough dental history followed by a careful clinical examination.
Key aspects include identifying the patient’s chief complaint and assessing whether pain occurs during chewing—either on biting or upon release. Additional considerations include a history of fractured or dislodged restorations, episodes of transient sensitivity to cold, and the presence of tooth mobility.
- Examination of the soft tissues to detect any localized swelling or the presence of sinus tracts.
- Percussion.
- Palpation of surrounding tissues.
- Biting tests, with each cusp assessed individually .
- Vitality testing.
- Periodontal probing.
- Removal of existing restorations, when necessary, to allow complete visualization of the crack.
- Transillumination, which helps identify disruptions in light transmission commonly associated with cracked teeth.
- Dye staining—performed either before or after removal of restorations—can further enhance visualization of crack lines.
- In certain cases, surgical assessment may be required for definitive evaluation.
- Radiographic examination is also essential and should routinely include periapical radiographs (PA) as well as cone beam computed tomography (CBCT) to improve detection and assessment of the extent of fractures.
The use of a surgical operating microscope is recommended, as subtle cracks or fractures are often not visible to the naked eye (4).
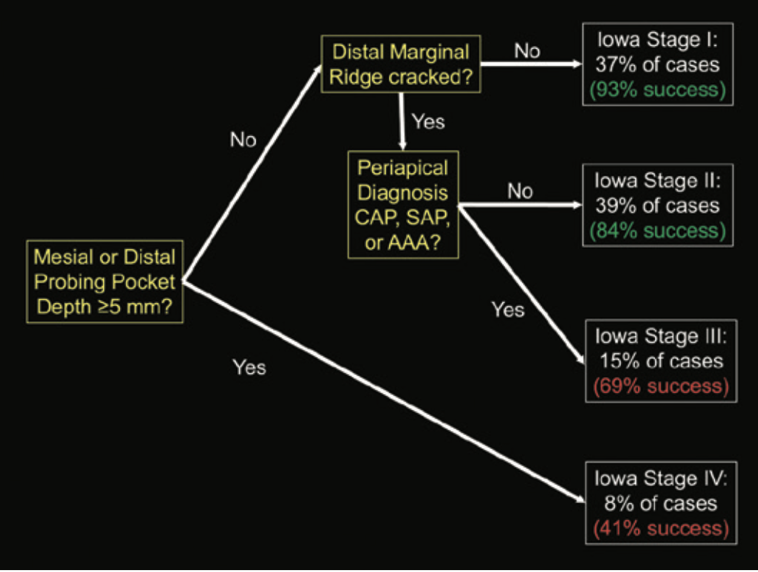
Fig. 9
Treatment Options for Cracked Teeth (4)
Although predicting the exact prognosis of a cracked tooth is not always possible, current evidence provides valuable guidance for clinical decision-making.
- It is important to inform patients that the affected tooth is structurally compromised and may carry a guarded prognosis. However, a cracked tooth should not be considered hopeless.
- Early diagnosis is crucial, as it significantly enhances tooth survival—particularly when a full-coverage crown is placed promptly. Evidence indicates that cracked teeth with reversible pulpitis and normal periapical status that receive immediate crowning have about an 80% likelihood of not requiring root canal treatment (5,6).
- If symptoms persist and progress to irreversible pulpitis or pulpal necrosis, root canal treatment becomes necessary.
- Patients with reversible pulpitis who opt for crown placement should be informed that, if endodontic therapy is later required, it can be performed through the existing crown without the need for replacement afterward.
“Clinical outcomes of cracked teeth depend on multiple factors, including the extent and location of the crack, pulpal condition, and timing of intervention. While many cracked teeth can function successfully for years with appropriate management, variability in prognosis should always be communicated.
The Iowa Staging Index (4) is a decision-making “tree” to identify the factors influencing the success of cracked teeth following root canal treatment and subsequent crown placement.
Three key factors have been shown to significantly affect outcomes.
- The first factor is the depth of periodontal probing associated with the crack. Shallower probing depths (less than 5 mm) are generally linked to better outcomes.
- The second factor is the location of the crack, with cracks involving the distal marginal ridge demonstrating lower success rates.
- The third factor is the presence of periapical pathology at the time of diagnosis. Conditions such as acute apical abscess, symptomatic or asymptomatic apical periodontitis, and chronic apical abscess are all associated with a poorer prognosis.
The Iowa Staging Index further categorizes prognosis based on these variables.
1. Stage I, teeth present with probing depths < 5 mm, no apical pathology, and a crack limited to the mesial marginal ridge. These cases show high success (around 93%) and survival rates (up to 97%) (8).
2. Stage II same as stage I, but with a distal marginal ridge crack, resulting in a slightly reduced success rate of 84%.
3. Stage III, teeth still have probing depths < 5 mm and distal cracks, but with associated apical pathology, reducing success to approximately 69%.
4. Stage IV includes teeth with probing depths > 5 mm regardless of crack location, where success drops significantly to about 41% (9).
Treatment Options for Vertical Root Fractures (4)
Single-rooted teeth with VRF require extraction, as predictable treatment options are limited. These fractures often occur in teeth that have previously undergone endodontic therapy and later develop periapical pathology. Teeth that have been root canal treated—especially those restored with posts or with significant loss of root structure—are at higher risk, although fractures can also occur in non-endodontically treated teeth.
Multi-rooted teeth with VRF have been managed historically with conservative surgical approaches such as root resection, root amputation, or hemisection, rather than extraction followed by implant placement. (Root amputation procedures have demonstrated survival rates of approximately 92% over 12 years, while hemisection procedures have reported survival rates ranging from 79% to 91% over follow-up periods of 7 to 30 years).
These findings support the view that such traditional treatment modalities are not only conservative but may also provide long-term outcomes that are comparable to or even superior to implant therapy.
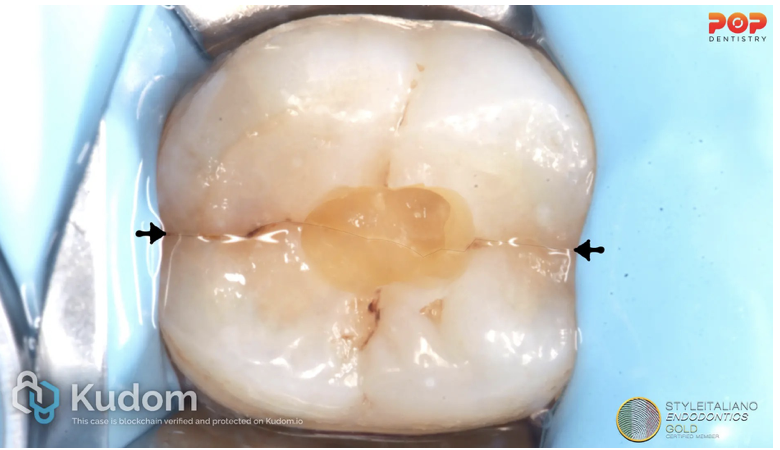
Fig. 10
This patient has presented with a history of direct trauma to the front of the face. The lower right central incisor had undergone RCT and apical surgery after luxation. Tooth mobility and further resorption were reported after 1.5 years, and the tooth was eventually extracted due to grade III mobility. The patient has also presented with dull and poorly localized pain related to the lower right quadrant, “rebound pain.”; sharp pain that occurs upon release of biting pressure. The tooth was +ve to percussion, responsive to the vitality, biting test and had no periodontal probing.

Fig. 11
Radiographic examination reveals widening of the PDL space related to the roots of the lower 2nd molar.

Fig. 12
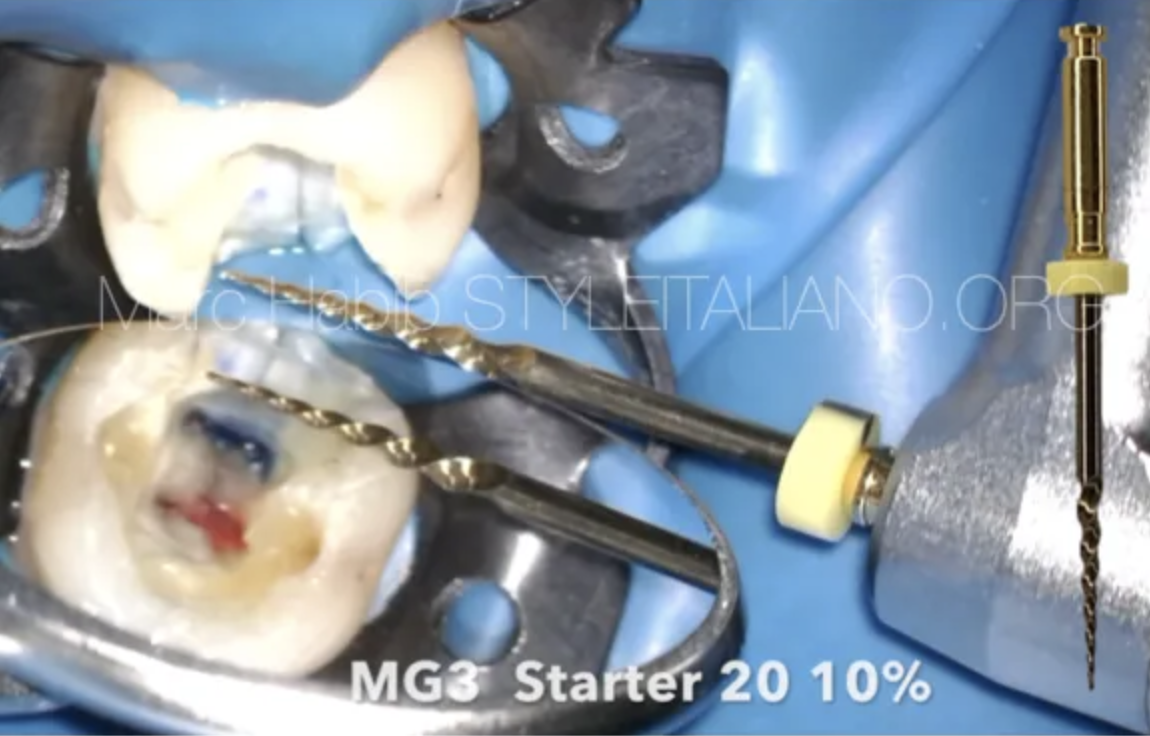
Conservative access cavity preparation.

Fig. 13
RCT was completed on two visits with minimal canal preparation and Obtruation. The patient was referred back to the prosthodontist for crown placement.
Conclusions
Cracked Teeth
Early detection of cracked teeth is paramount, as it significantly improves the likelihood of long-term tooth survival. While not all cracked teeth require root canal treatment, placement of a full-coverage crown is essential in all cases. Occlusion should be carefully evaluated during the initial examination, with adjustments made to minimize excessive forces.
When root canal treatment is indicated, conservative access cavity preparation is recommended to avoid further compromise of the tooth structure. the placement of an orifice barrier below the level of the crack—ideally under magnification using a surgical operating microscope—may help improve outcomes. A definitive crown should be placed as soon as possible; however, in cases of reversible pulpitis, a well-adapted temporary crown may be used until symptoms resolve. Regular follow-up and monitoring of occlusion are also crucial for long-term success (4).
Vertical Root Fractures
Advances in imaging, particularly the use of cone beam computed tomography (CBCT), have improved the diagnosis of vertical root fractures. Despite this, such fractures are generally considered catastrophic for the affected root. In single-rooted teeth, extraction is typically the only viable treatment.
For multi-rooted teeth, a more conservative approach may be possible. Clinical evidence suggests that removal of the fractured root, followed by restoration of the remaining root structure, can yield favorable outcomes—often surpassing those of some implant treatments. Ongoing monitoring and occlusal adjustments remain essential components of care (4).
Bibliography
- Scott B. McClanahan, D.D.S., M.S., ChairSpecial Committee to Revise the Glossary (2020), et al., American Association of Endodontists (2020) Glossary of endodontic terms Tenth Edition. 2020: p. 48.
- Hasan S, Singh K, Salati N. Cracked tooth syndrome: overview of literature. International Journal of Applied and Basic Medical Research. 2015;5(3):164–8.
- Brännström M. The hydrodynamic theory of dentinal pain: sensation in preparations, caries, and the dentinal crack syndrome. Journal of endodontics. 1986;12(10):453–7.
- Krell KV. Cracked teeth and vertical root fractures: a new look at a growing problem. ENDODONTICS: Colleagues for Excellence; American Association of Endodontists: Chicago, IL, USA. 2022.
- Khasnis SA, Kidiyoor KH, Patil AB, Kenganal SB. Vertical root fractures and their management. Journal of Conservative Dentistry and Endodontics. 2014 Mar 1;17(2):103-10.
- Krell, K.V. and E.M. Rivera, A six year evaluation of cracked teeth diagnosed with reversible pulpitis: treatment and prognosis. J Endod, 2007. 33.
- Davis, M.C. and S.S. Shariff, Success and Survival of Endodontically Treated Cracked Teeth with Radicular Extensions: A 2- to 4-year Prospective Cohort. J Endod, 2019. 45(7): p. 848-855.
- Krell, K.V. and D.J. Caplan, 12-month Success of Cracked Teeth Treated with Orthograde Root Canal Treatment. J Endod, 2018. 44(4): p. 543-548.
- Raj S, Singh A. Cracked tooth syndrome: a diagnostic dilemma-a mini review. Frontiers in Oral Health. 2025 Jun 24;6:1572665.
- Abbott, P. and N. Leow, Predictable management of cracked teeth with reversible pulpitis. Aust Dent J, 2009. 54(4): p. 306-15.