

Management of permanent necrotic teeth with inflammatory root resorption. Case report
30/04/2026
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Root resorption represents the loss of dental hard tissues (cementum, dentine and/or enamel). This irreversible tooth structure loss most often requires orthograde endodontic treatment and/or surgical management of the defect [1]. Inflammatory root resorption (IRR) is one of the greatest challenges for endodontists because of the altered canal anatomy resultant from the resorptive process [2].
In the majority of cases, it is associated with apical periodontitis, but IRR can occur after trauma, orthodontic treatment, auto transplantation or can be associated with idiopathic factors [3-5]. From a clinical point of view, we can encounter problems during the working length determination, the chemo-mechanical debridement and sealing of the root canal due to the lack of an apical constriction, hence for an optimal long-term outcome of the root canal treatment, special techniques are employed [6].
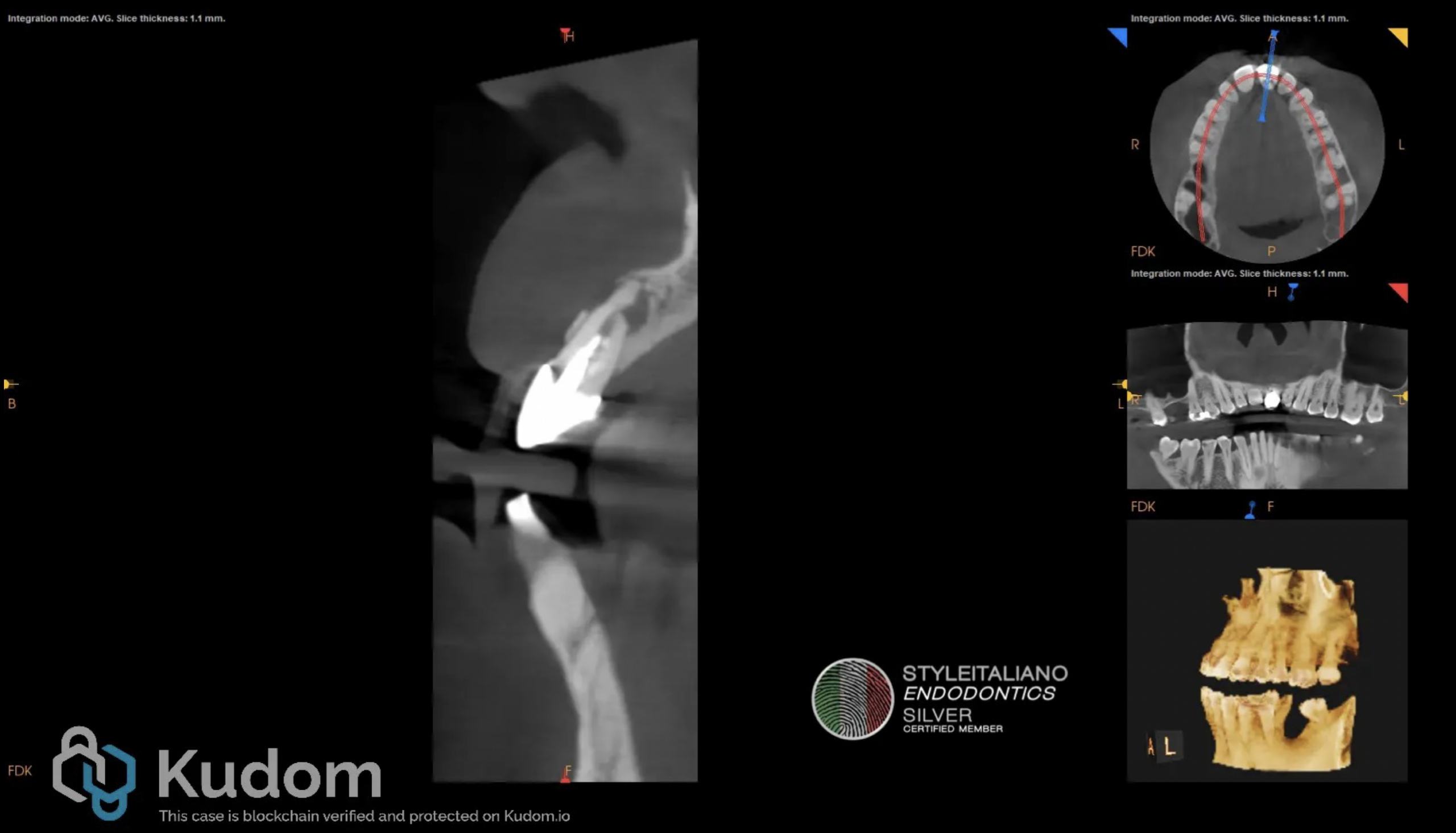
Fig. 1
A 45-year-old male patient was referred to our office for an evaluation of the upper left central incisor after the referring colleague detected an unusual canal anatomy on a periapical radiograph. The patient reported little to no discomfort and an intermittent discharge of pus through a sinus tract. After carefull clinical and radiological examination the maxillary left central incisor was diagnosed with previous root canal therapy and chronic apical abscess. The computed tomography ( CB-CT) examination revealed a well-defined radiolucency in the apical third of tooth 2.1, compatible with inflammatory root resorption as seen in Figure 1.
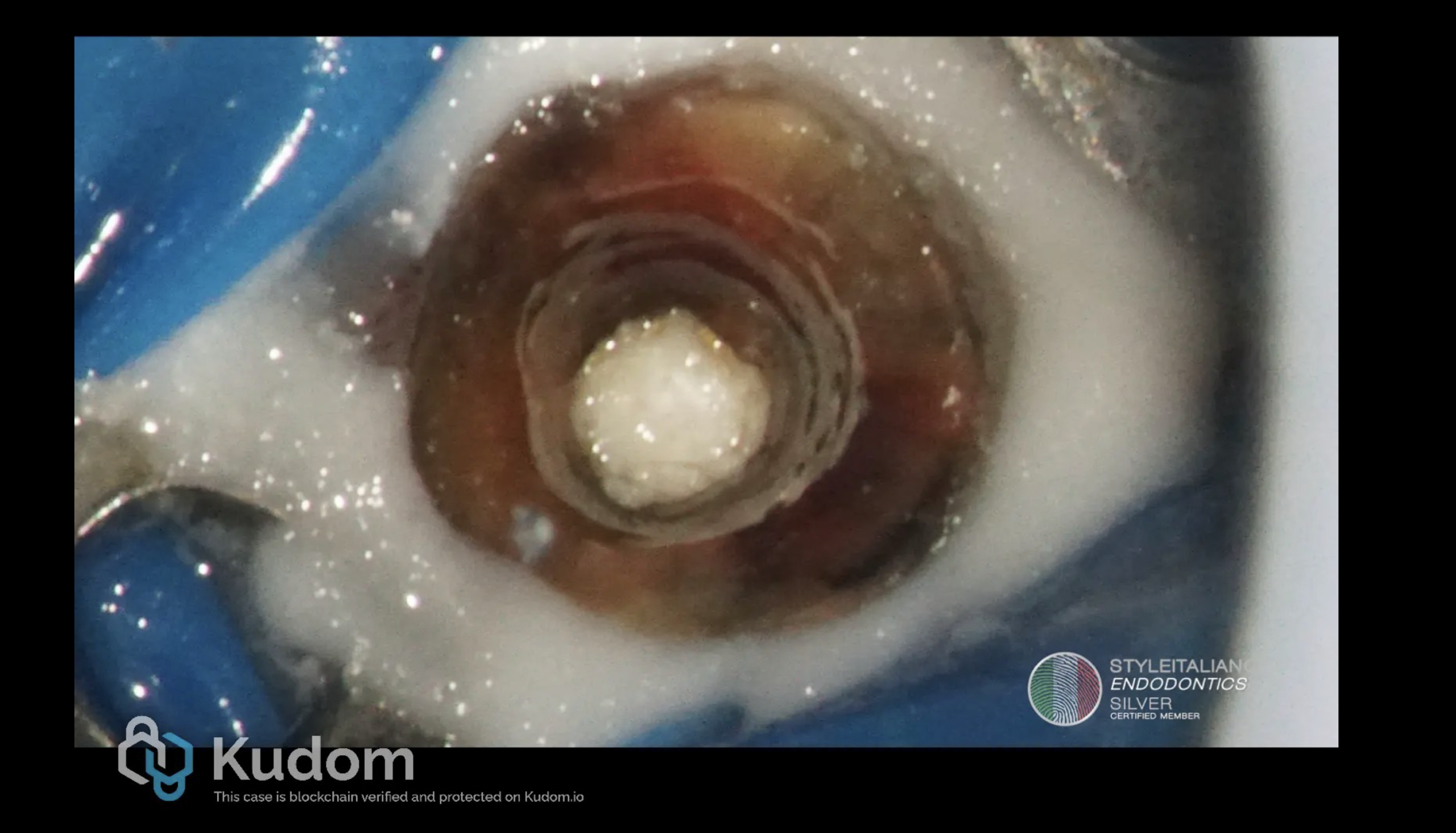
Fig. 2
For the treatment plan, non-surgical endodontic treatment was proposed and accepted by the patient. The treatment was performed under an operating microscope and rubber dam isolation. After removing the crown and establishing access with Ultrasonic tips, the canal was scouted with 10k and 15k stainless-steel hand files. Working length was established with the help of an electronic apex locator and confirmed by CB-CT measurement. The canal was shaped with Reciproc blue files until 40/06 and the apical one third was prepared by hand files until 60/02. NaOCl 5.25% was used throughout the endodontic procedure to facilitate chemical disinfection and removal of debris. After shaping, the hypochlorite was activated with sonic tips and, once cleansing was completed, we proceeded with 17% EDTA irrigation in order to remove the smear layer. After the final irrigation, the canal was dried using paper points and the working lenght was again checked by the paper point technique as a third complementary method to ensure the corect initial measurement of the working lenght [7]. A collagen sponge was placed as a resorbable internal matrix (apical barrier) beyond the apical foramen to prevent extrusion of filling materials [8] as seen in Figure 2. This colagen sponge acts as a stable base for compacting the filling material, allowing for a single-session, safe, and efficient root canal treatment of open apices [8].

Fig. 3
The canal was sealed using mineral trioxide aggregate (MTA) apical barrier and warm gutta-percha with resin sealer as seen in Figure 3. Intracoronal sealing was done with a dual cure flowable composite resin.
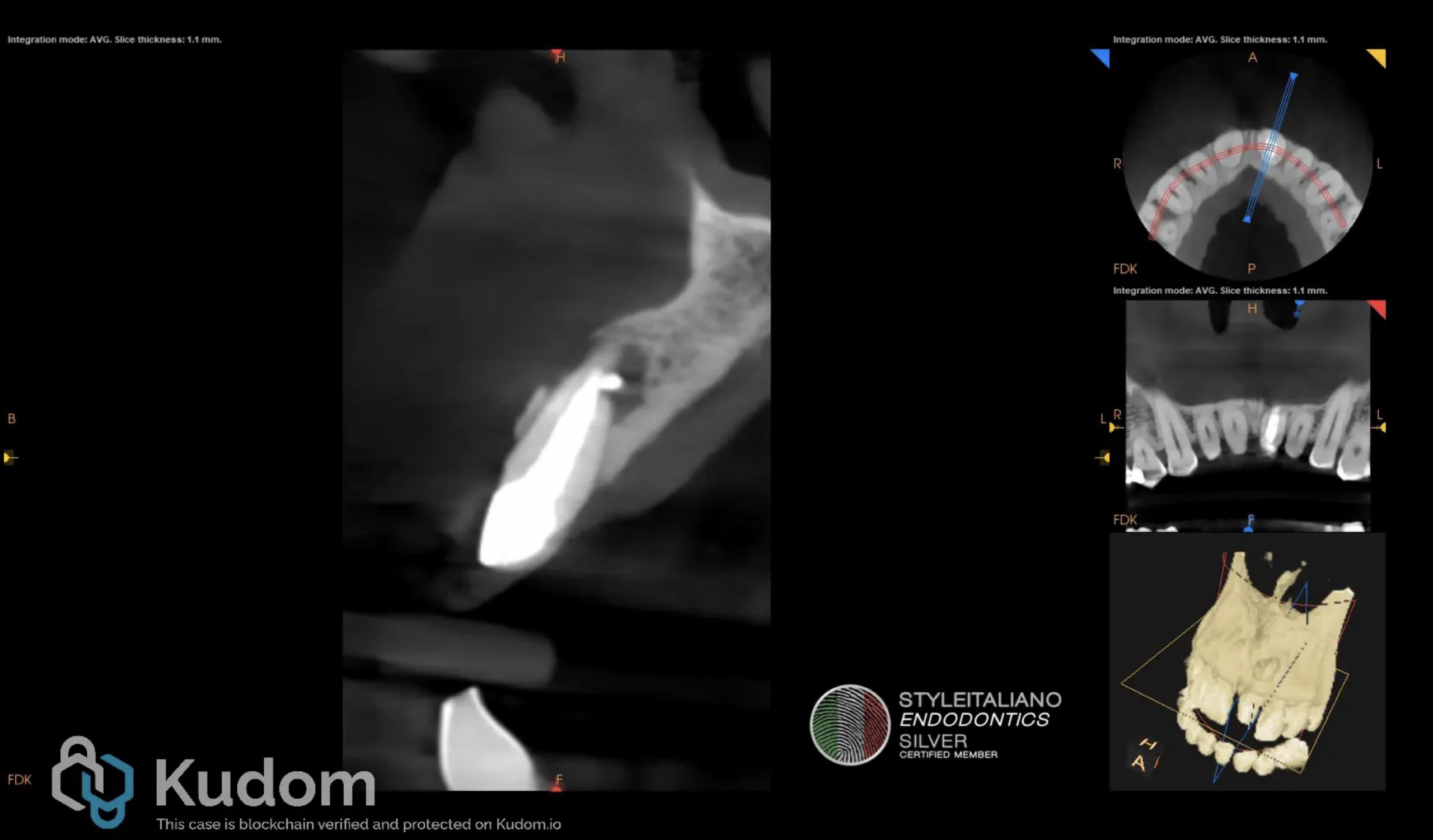
Fig. 4
Post endodontic treatment status of tooth 2.1 CB-CT view.
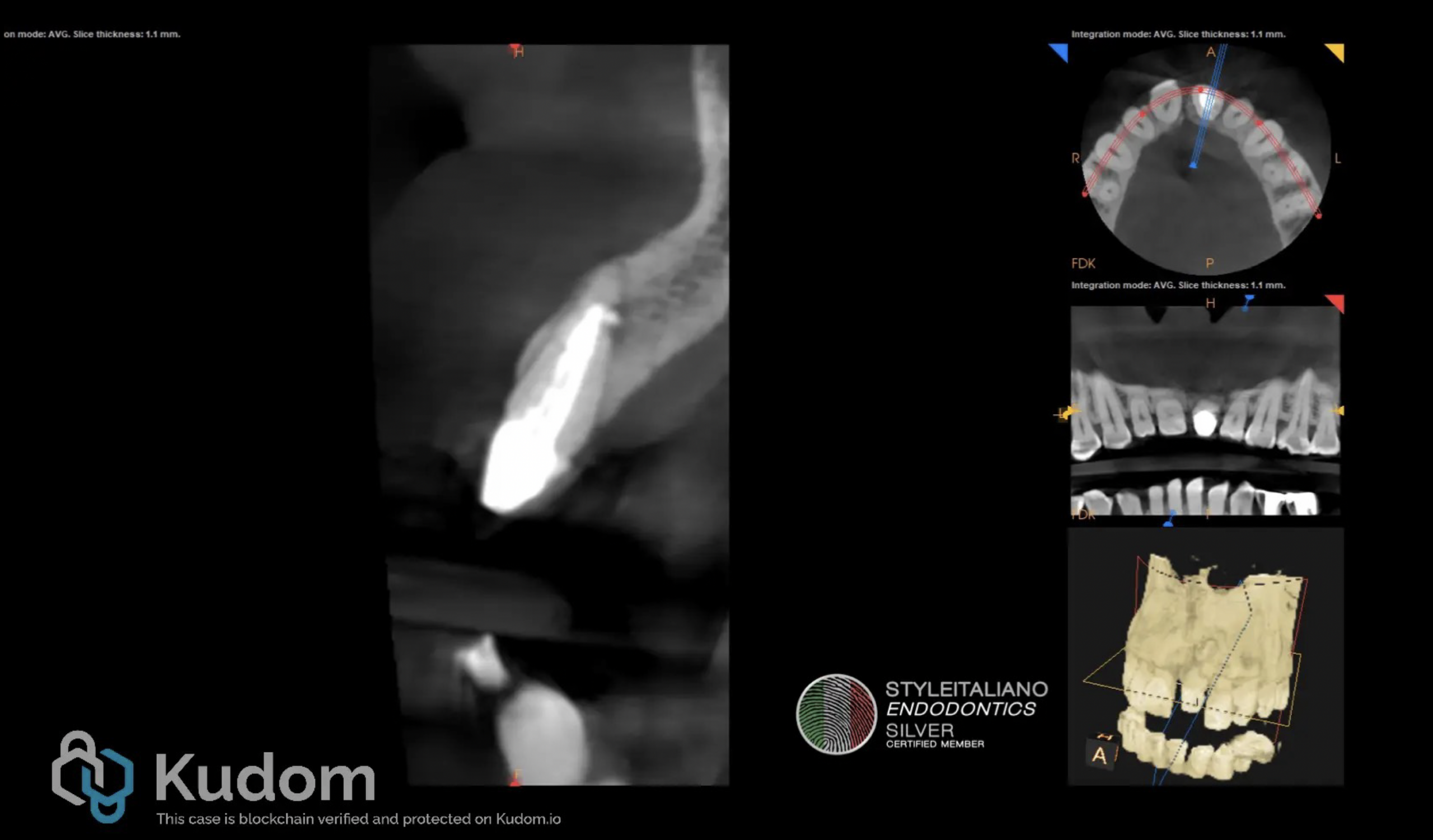
Fig. 5
At the 6 months recall, the patient remained free of symptoms and the CB-CT examination showed signs of healing, as seen in Figure 5.

Fig. 6
Moreover, at the 6 months recall the clinical aspect shows good signs of healing and the sinus tract appers to be closed.
The complex anatomic irregularities of the root canal and the resorption defect provide technical difficulties for thorough cleaning and obturation of the root canal [9]. A useful tool for such cases is the CB-CT, which is part of the current armamentarium in modern endodontics, together with the electronic apex locator (EAL) [10]. EAL demonstrated 87% accuracy as evaluated by CB-CT measurements [11]. For the obturation of the root canal a blockage of the apical foramen can be performed using MTA but other materials may be used such as Ca(OH)2 based materials or other bioceramic material [6].
Conclusions
Orthograde root canal treatment remains the preferred method to deal with teeth diagnosed with IRR. Early detection and a correct diagnosis are essential for successful management of such cases.
Bibliography
1. Bakhsh A, Patel S, Bhuva B. Root Resorption. In: Ahmed HMA, Dummer PMH, editors. Endodontic Advances and Evidence-Based Clinical Guidelines. 2022. Available from: https://doi.org/10.1002/9781119553939.ch5
2. Blicher B. Differentiating Resorption. AAE News. 2021 Jan 5. Available from: https://www.aae.org/specialty/differentiating-resorption/
3. Santos JB, Mateo-Castillo JF, Nishiyama CK, Esper LA, Pinto LD, Pinheiro CR. External root resorption: diagnosis and treatment. clinical case report. J Dent Health Oral Disord Ther. 2018;9.
4. Abbott PV. Prevention and management of external inflammatory resorption following trauma to teeth. Aust Dent J. 2016 Mar;61 Suppl 1:82-94. doi: 10.1111/adj.12400. PMID: 26923450.
5. Asgary S, Parhizkar A. Management of External Inflammatory Root Resorption following Tooth Autotransplantation Using a Modified Combination of Triple Antibiotics. Case Rep Dent. 2022 Jun 15;2022:5178339. doi: 10.1155/2022/5178339. PMID: 35754759; PMCID: PMC9217544.
6. Patel S, Saberi N, Pimental T, Teng PH. Present status and future directions: Root resorption. Int Endod J. 2022 Oct;55 Suppl 4(Suppl 4):892-921. doi: 10.1111/iej.13715. Epub 2022 Mar 30. PMID: 35229320; PMCID: PMC9790676.
7. Marcos-Arenal JL, Rivera EM, Caplan DJ, Trope M. Evaluating the paper point technique for locating the apical foramen after canal preparation. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108(5):e101-e105. doi:10.1016/j.tripleo.2009.06.011.
8. Graziele Magro M, Carlos Kuga M, Adad Ricci W, et al. Endodontic Management of Open Apex Teeth Using Lyophilized Collagen Sponge and MTA Cement: Report of Two Cases. Iran Endod J. 2017;12(2):248-252. doi:10.22037/iej.2017.48
9. Sangavi T, Karthick A, Venkatesh A, Dhakshinamoorthy M. Management of internal root resorption: A Review. 2021;7:658-662.
10. Martins JNR, Marques D, Silva EJNL, Caramês J, Versiani MA. Prevalence Studies on Root Canal Anatomy Using Cone-beam Computed Tomographic Imaging: A Systematic Review. J Endod. 2019 Apr;45(4):372-386.e4. doi: 10.1016/j.joen.2018.12.016. Epub 2019 Mar 2. PMID: 30833097.
11. Shibin J, Gs P, M S, S N, Adimoulame S, M K. Evaluation of the Working Length Determination Accuracy by Cone-beam Computed Tomography in Primary Teeth. Int J Clin Pediatr Dent. 2022;15(Suppl 1):S92-S96. doi: 10.5005/jp-journals-10005-2330. PMID: 35645504; PMCID: PMC9108823.



