C-shaped molars
02/01/2026
Mohamed Abdelkhalek
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Root canal anatomy plays a pivotal role in the success of endodontic treatment. While most teeth follow well-described anatomical configurations, certain morphological variations present significant clinical challenges. Among these, the C-shaped canal system represents one of the most complex and unpredictable anatomical patterns encountered in endodontic practice.
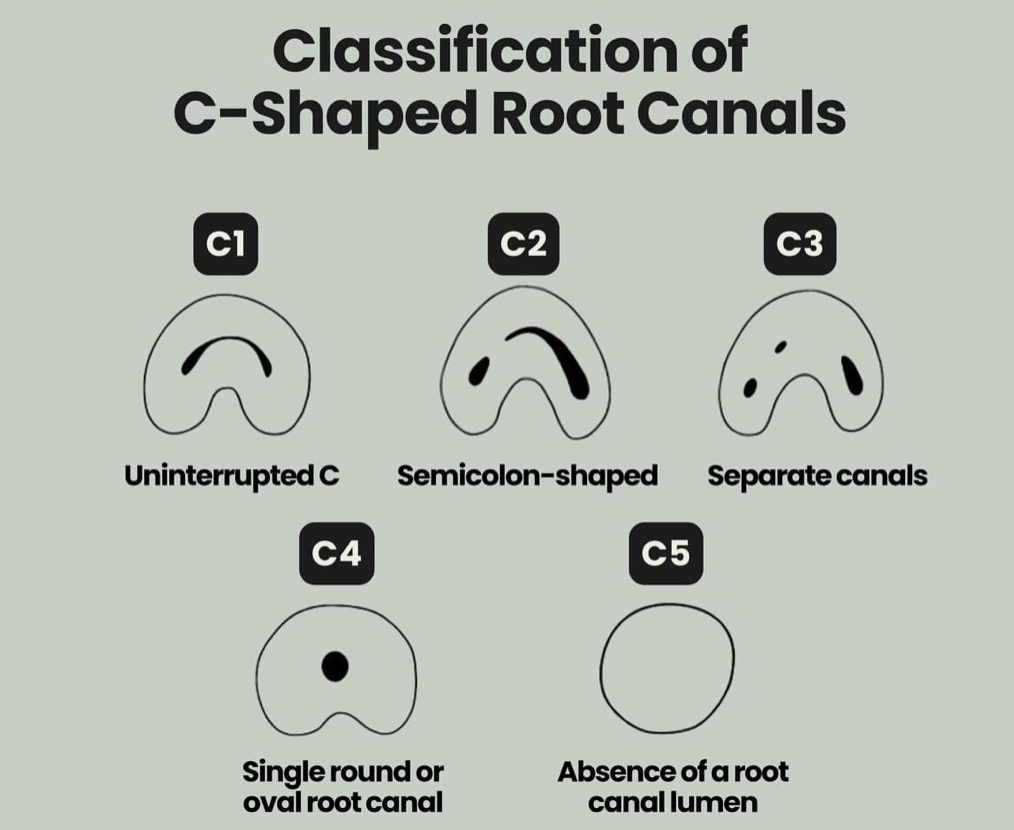
Fig. 1
The C-shaped canal configuration is characterized by a continuous or semi-continuous fin or web connecting individual canals, forming a "C"-shaped cross-section.
This anatomical variation results from the failure of Hertwig's epithelial root sheath to fuse on either the buccal or lingual surface during root development.
The prevalence of C-shaped canal systems varies widely among different populations, ethnic groups, and tooth types, reflecting the strong genetic influence on root development. This anatomical variation is predominantly observed in mandibular second molars, although it has also been reported in mandibular first molars, premolars, and, less commonly, maxillary molars.
Multiple epidemiological studies have demonstrated a significantly higher prevalence of C-shaped canals in Asian populations, with reported rates ranging from 29% to over 45% in Chinese, Korean, and Korean-American populations. In Japanese cohorts, prevalence values between 30% and 36% have been consistently reported.
These high percentages contrast sharply with those observed in Caucasian populations, where the prevalence typically ranges between 2% and 8%.
Studies conducted in Middle Eastern populations have revealed intermediate prevalence values. Reported rates range from 10% to 22%, with variations attributed to geographic location, sample size, and the diagnostic methods used. These findings are particularly relevant to regional clinical practice, as clinicians serving Middle Eastern communities may encounter C-shaped canal systems more frequently than those practicing in Western populations.
Gender-based differences have also been investigated, with several studies reporting a higher prevalence in females compared to males. This trend is thought to be related to genetic and developmental factors influencing root morphology, although the exact mechanism remains unclear.
The introduction of cone-beam computed tomography
(CBCT) has led to a noticeable increase in reported prevalence values compared with conventional radiographic studies. CBCT provides three-dimensional visualization of complex canal configurations, allowing more accurate detection of C-shaped morphology, particularly in cases where conventional radiographs fail to reveal the characteristic anatomical features.
Overall, the high prevalence of C-shaped canals in certain populations underscores the importance of careful preoperative assessment and the routine consideration of this anatomical variation, particularly when treating mandibular second molars.
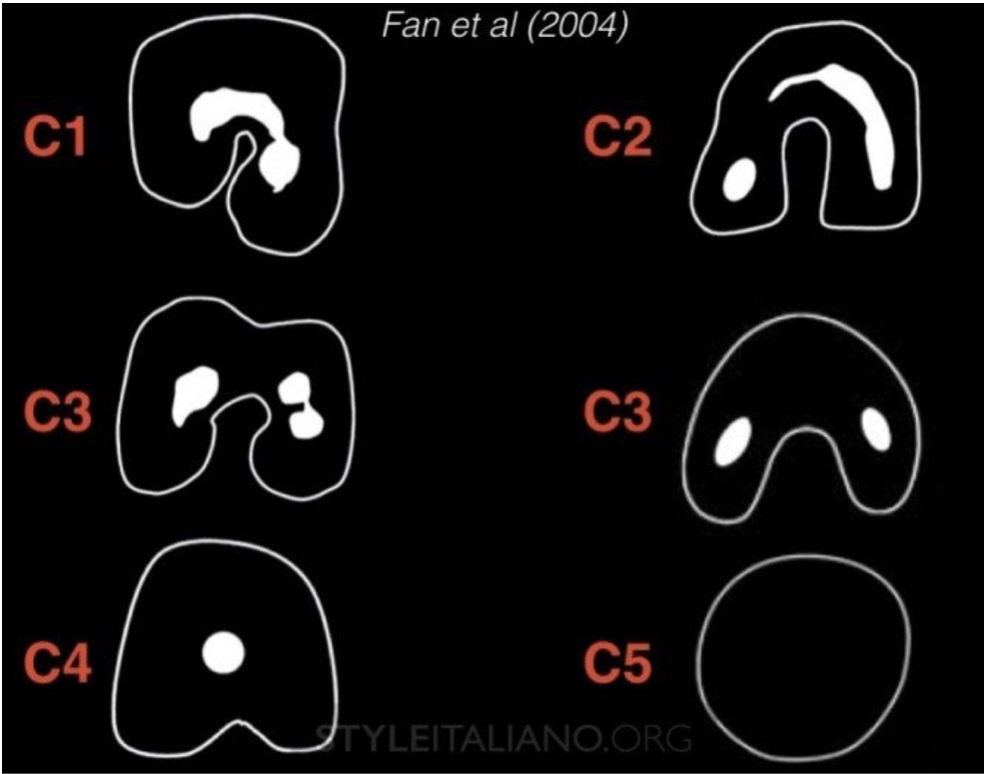
Fig. 2
C-shaped root canal systems exhibit significant anatomical complexity and variability. Several classification systems have been proposed to describe their morphology. The most widely accepted and clinically relevant classification is that of Fan et al. that was done in 2004, which categorizes C-shaped canals according to their cross-sectional configuration.
In the next slides I’m gonna share with you every type clinically & radiographically
Fan's Classification
Type Description
C1
A continuous C-shaped canal with no separation.
C2
A semicolon-shaped canal resulting from discontinuation of the C outline.
С3
Two or three distinct canals with no C-shaped configuration. • C3a: Two separate canals. • C3b: Three separate canals.
C4
A single round or oval canal.
C5
No visible canal lumen (often observed near the apex).
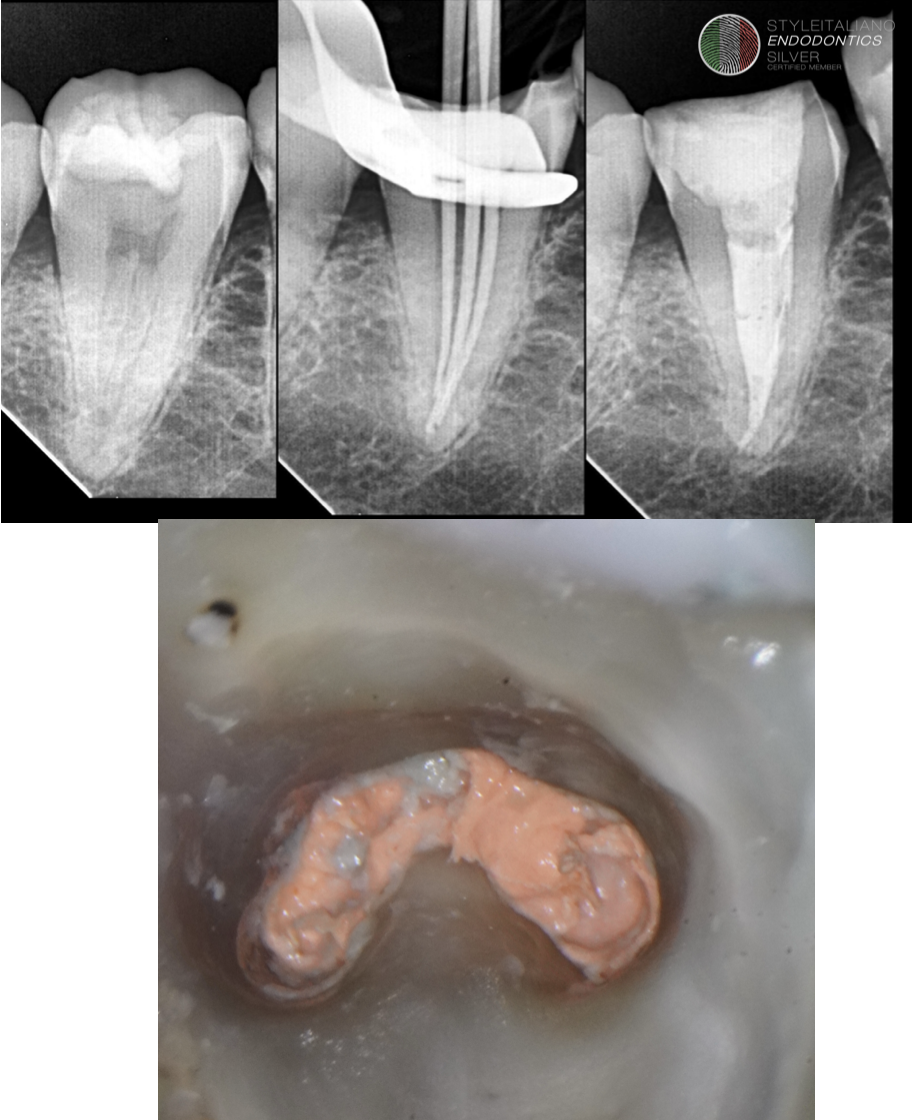
Fig. 3
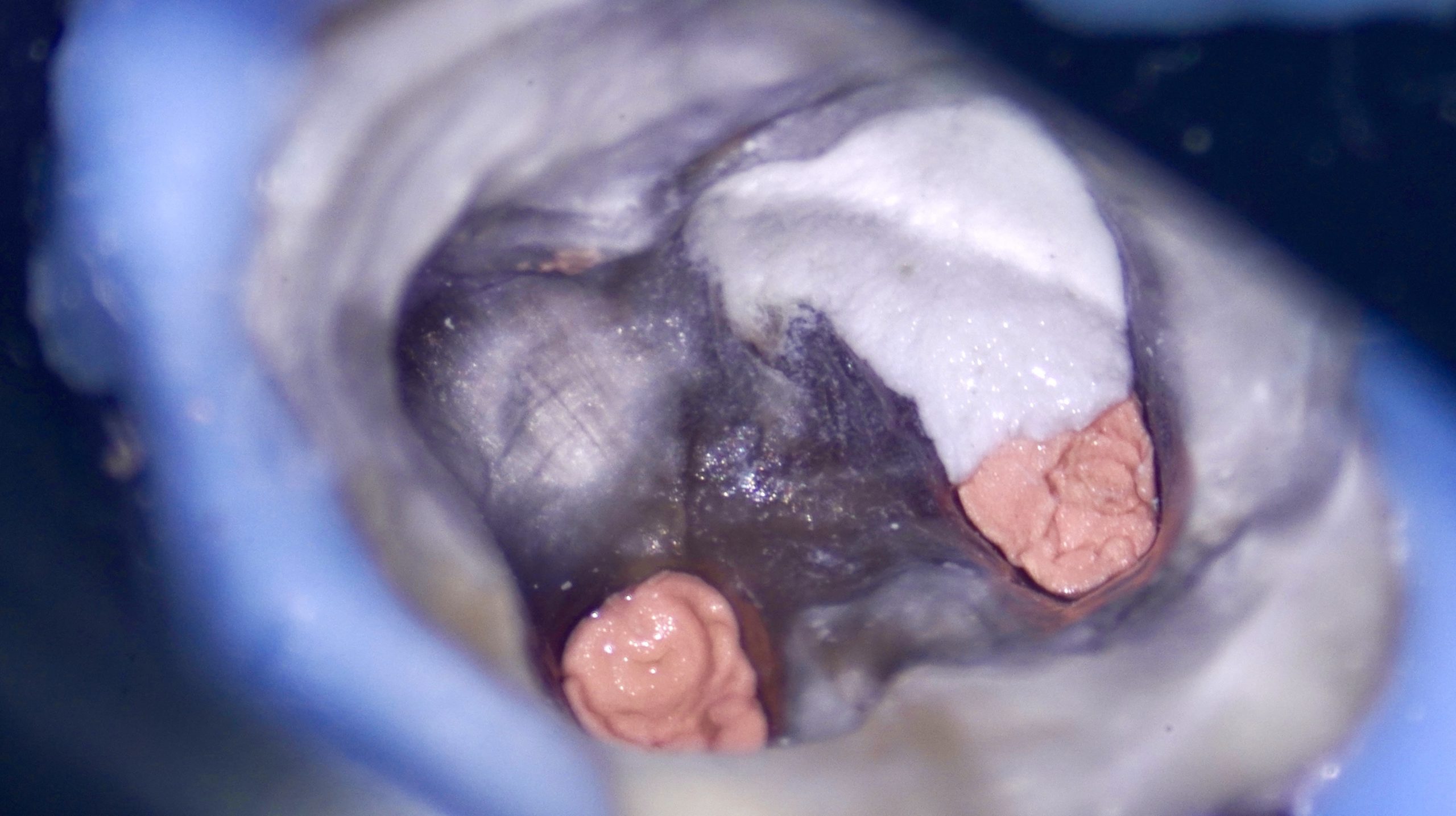
C1 configuration
The C1 configuration represents the baseline and most characteristic form of the C-shaped canal system. In this configuration, the canal lumen forms a continuous crescent-shaped outline extending from the mesial to the distal aspect without any separation. This uninterrupted morphology establishes a single, broad canal space with an extensive isthmus and thin dentinal walls, creating a unified internal anatomy rather than multiple discrete canals. Clinically, C1 is generally encountered in the coronal and middle thirds of the root and serves as the fundamental pattern from which more segmented configurations (C2-C4) may evolve along the root length.
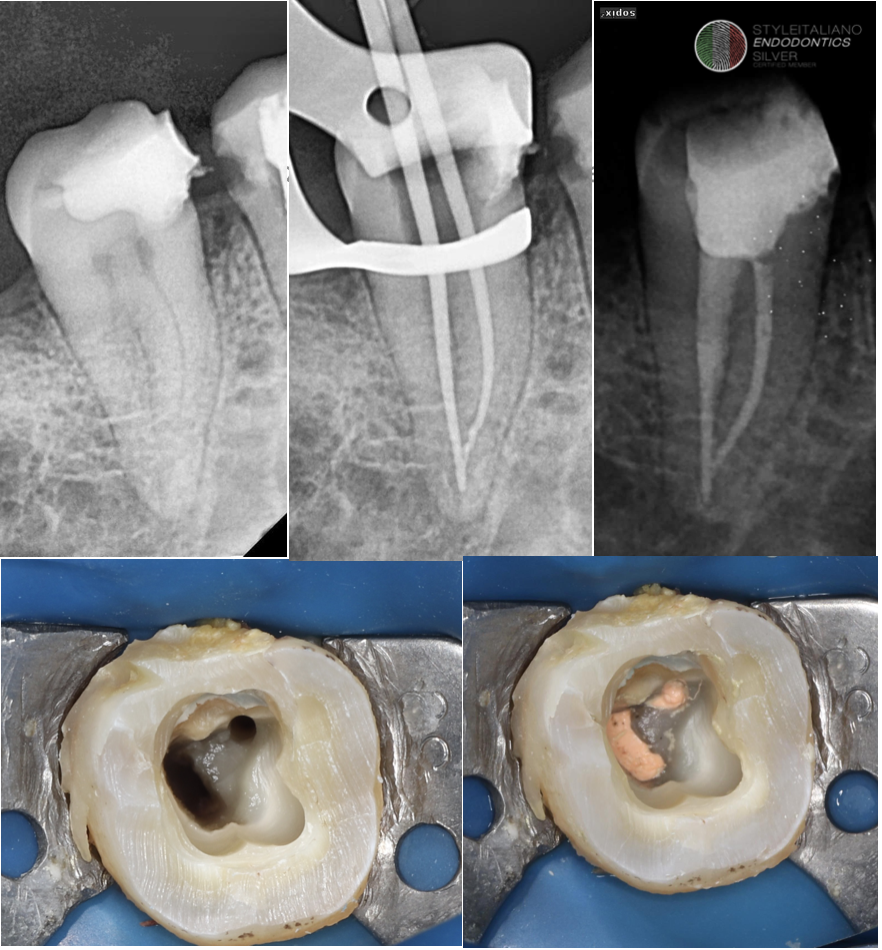
Fig. 4
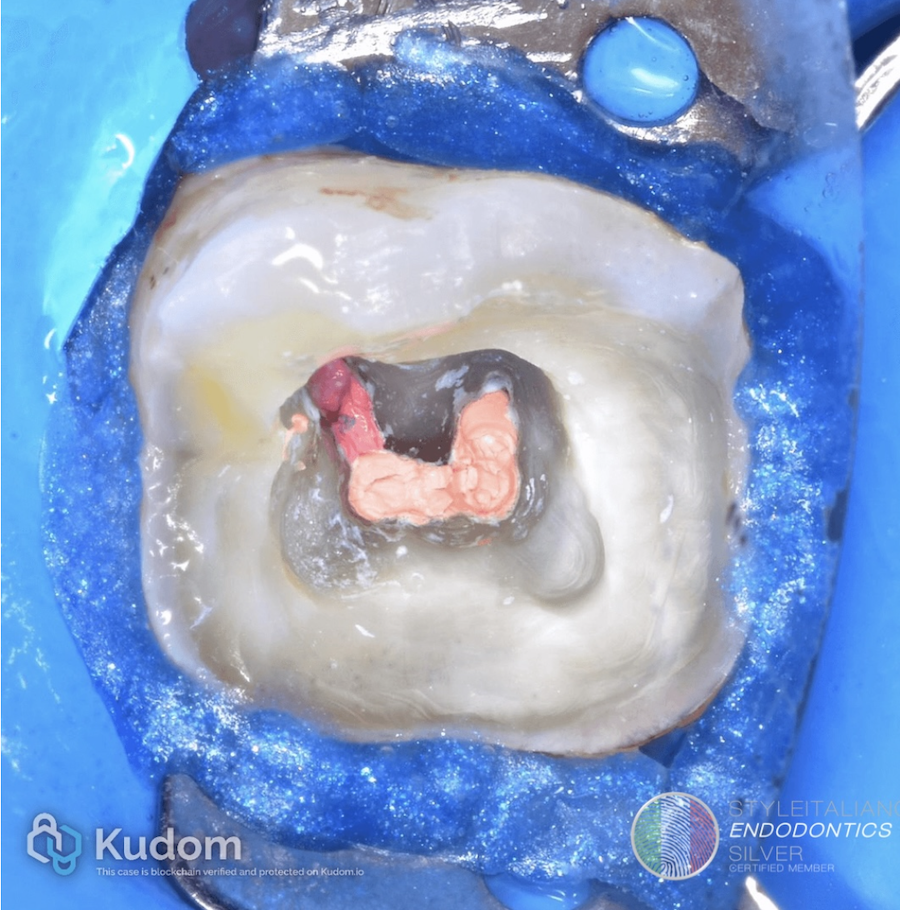
C2 configuration
The C2 configuration represents a transitional form between the continuous C-shaped anatomy of C1 and the more segmented canal systems observed in advanced configurations. In this pattern, the original C-shaped outline becomes partially disrupted, producing a semicolon-shaped canal lumen. This disruption results in the formation of a main canal accompanied by a secondary canal space that remains connected by a narrow isthmus or dentinal web. Unlike C1, the canal system in C2 is no longer a single unified space; however, residual communication between canal segments persists, maintaining anatomical complexity. Clinically, this configuration poses increased challenges for complete debridement and obturation due to the presence of narrow connecting fins and irregular canal contour.
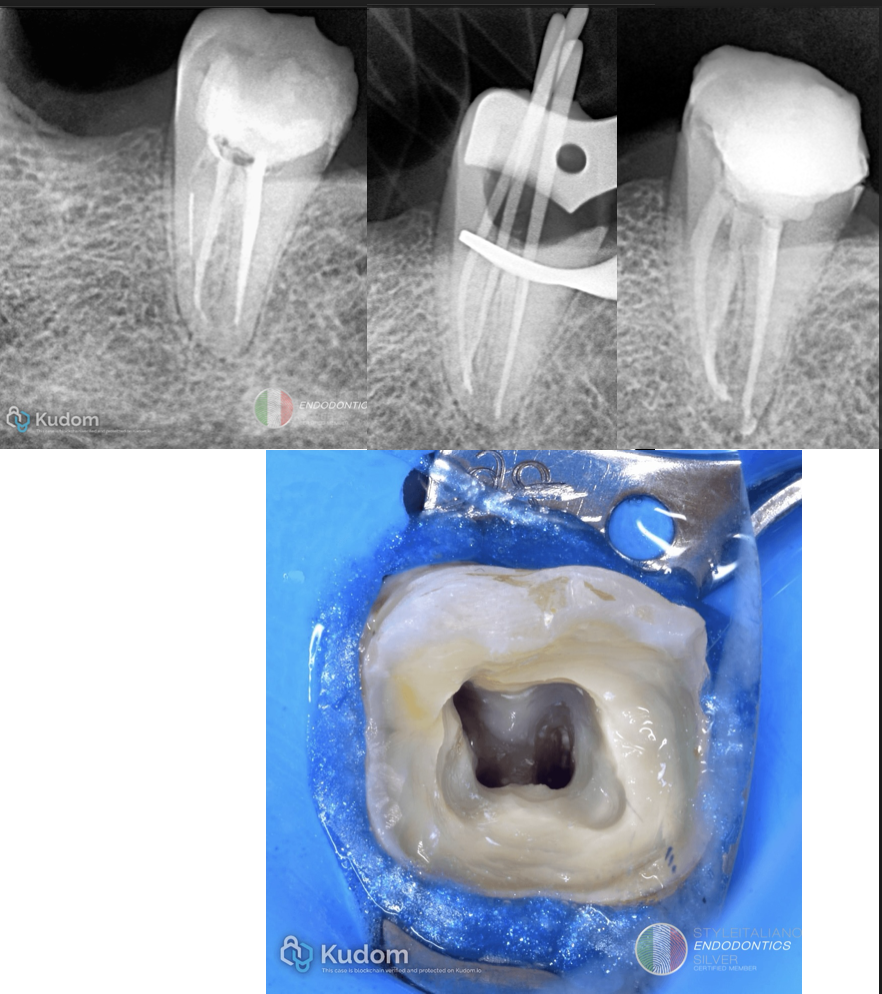
Fig. 5
C3(a) configuration
The C3a configuration represents a further progression in the segmentation of the C-shaped canal system, characterized by the complete loss of the continuous C-shaped outline. In this subtype, the canal space is divided into two distinct and clearly separated canals with no remaining isthmus or dentinal connection between them.
This configuration reflects a transition from a partially connected anatomy (as seen in C2) to a fully separated canal system, resulting in a morphology that clinically resembles a conventional two-canal pattern rather than a unified C-shaped space. Although the canals appear anatomically independent, their origin from a C-shaped system often leaves irregular canal contours and thin dentinal walls, which may still complicate cleaning and obturation
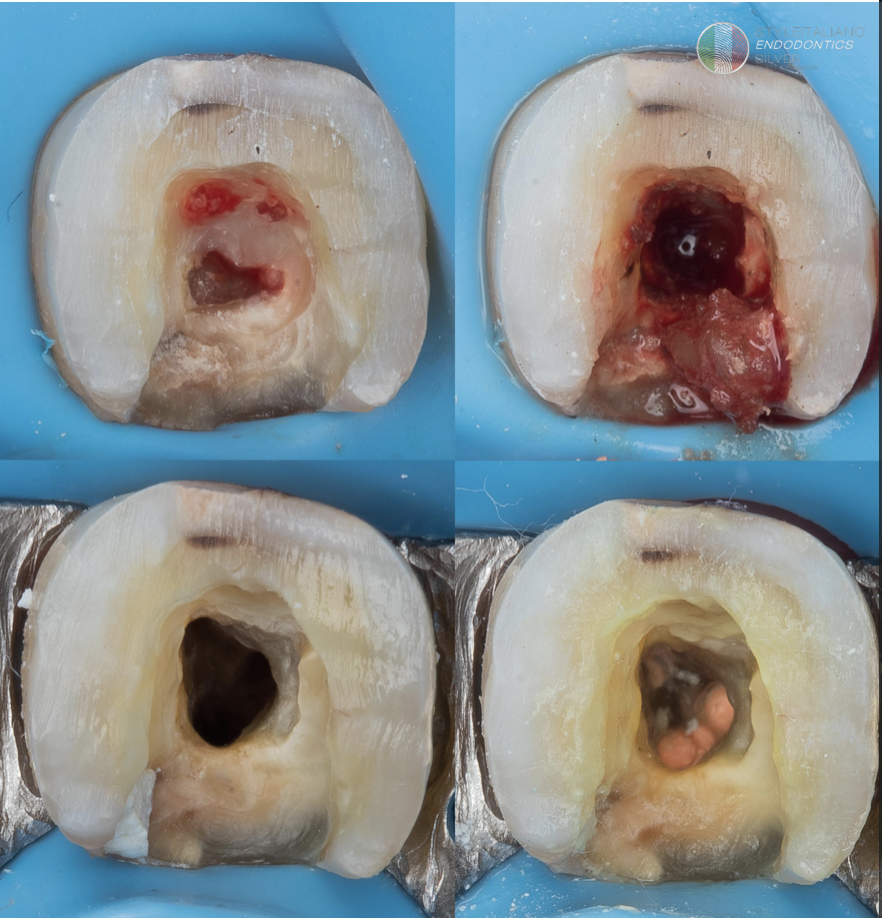
Fig. 6
C3(b) configuration
The C3b configuration represents the most advanced stage of segmentation within the C-shaped canal system.
In this subtype, the original C-shaped anatomy is completely lost, and the canal space is divided into three distinct and separate canals, with no remaining intercanal communications. This configuration reflects a fully individualized canal morphology, which may closely resemble a conventional three-canal pattern.
Nevertheless, the canals typically retain irregular internal contours and thin dentinal walls as remnants of their C-shaped origin
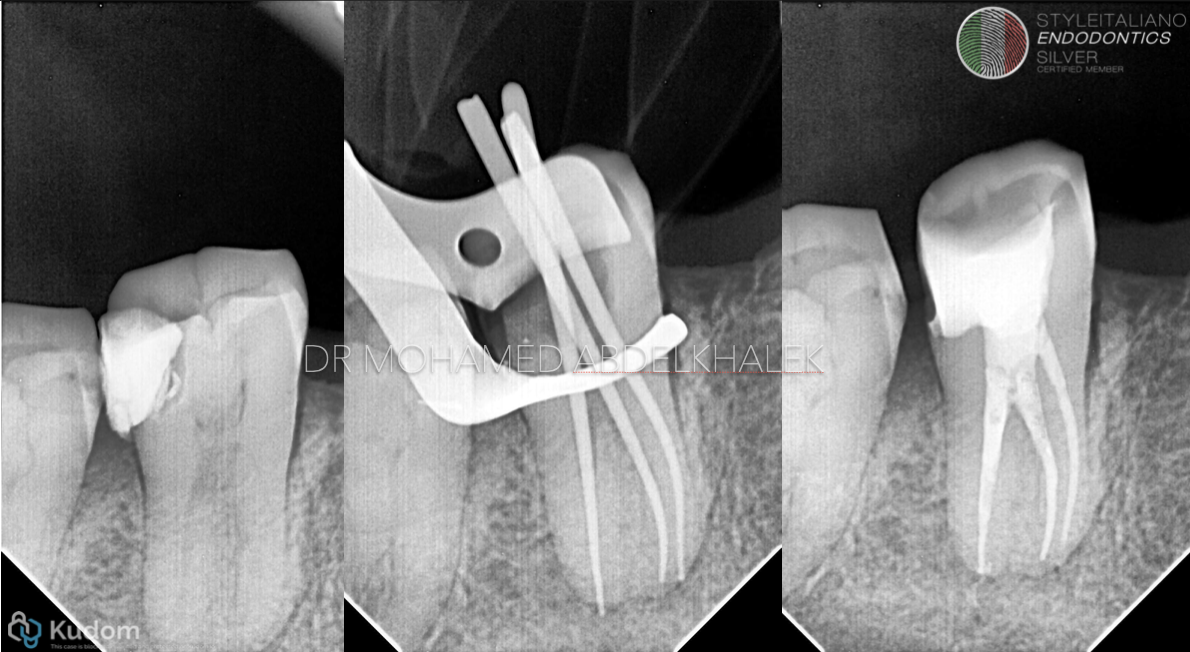
Fig. 7
These anatomical characteristics may complicate instrumentation and obturation, necessitating careful canal scouting, conservative shaping, and enhanced irrigation strategies to ensure thorough disinfection.
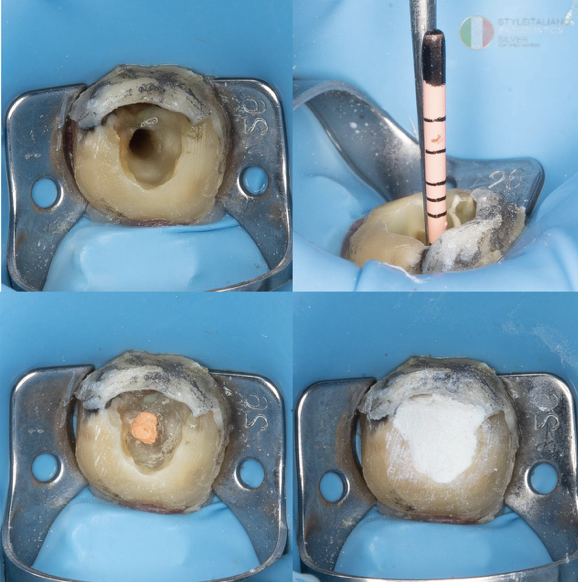
Fig. 8
C4 configuration
The C4 configuration represents a terminal stage in the morphological transformation of the C-shaped canal system. In this configuration, the complex, segmented anatomy observed in C3 simplifies into a single round or oval canal lumen. This form reflects a marked reduction in internal anatomical irregularities and intercanal complexity, often observed in the apical third of the root.
Despite the apparent simplicity of its shape, the canal in C4 may still present thin dentinal walls and residual anatomical asymmetry related to its C-shaped origin.

Fig. 9
Clinically, this configuration may give a false impression of straightforward anatomy, emphasizing the importance of cautious instrumentation and thorough irrigation to ensure complete debridement.
Fig. 10
C5 configuration
The C5 configuration represents the final and most apically positioned stage of C-shaped canal morphology.
It is characterized by the absence of a visible canal lumen, which is typically attributed to extreme canal narrowing or complete obliteration near the apical region.
This configuration reflects advanced anatomical constriction resulting from the progressive segmentation and tapering of the C-shaped system along the root length. Clinically, C5 presents a significant challenge for canal negotiation, working length determination, and effective disinfection, necessitating the use of magnification, ultrasonics, and gentle canal scouting techniques to avoid procedural complications.
Conclusions
The C-shaped root canal configuration in second mandibular molar has an ethnic predilection. Our understanding in the anatomical presentations of this variation will help us manage this configuration effectively. Diagnosis as well as root canal procedure is important to be carried out adequately to ensure good treatment result.
Bibliography
1. Cooke HG, Cox FL. C-shaped canal configurations in mandibular molars. J Am Dent Assoc 1979; 99:
8360839.
2. Yang ZP, Yang SF, Lin YL. C-shaped root canals in mandibular second molars in Chinese population.
3.Endod Dent Traumatol 1988; 4: 1600163 Manning S. Root canal anatomy of mandibular second molars. Part Il C-shaped canals. Int. Endod. J 1990; 23: 40-45
4. Melton DC, Krell KV, Fuller MW. Histological Anatomical and features of C-shaped canals in mandibular second molars. J Endod 1991; 17: 384-388.
5.Sabala CL, Benenati FW, Neas BR. Bilateral root or root canal aberra- tions in a dental school patient population. J Endod 1994; 20: 38042.
6. Haddad GY, Nehme WB, Ounsi HF. Diagnosis, classification, and frequency of C-shaped canals in