Endodontic Retreatment of a Bifurcated Mandibular Second Premolar with 12-Month Follow-up
24/11/2025
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
A case of successful retreatment of a mandibular second premolar (FDI: 35) with chronic apical periodontitis, caused by a missed lingual canal (Vertucci Type IV bifurcation). Utilizing a dental operating microscope and Passive Ultrasonic Irrigation (PUI), both canals were cleaned and sealed with bioceramic sealer. The 12-month follow-up confirmed the patient was asymptomatic, demonstrating significant bone regeneration and complete periapical healing. Advanced technology is crucial for managing complex anatomy and achieving long-term endodontic success.

Fig. 1
A 35-year-old male patient presented with a chief complaint of intermittent pain and localized mild swelling in the region of the lower left second premolar over a three-month period. The tooth had undergone primary root canal treatment five years earlier.
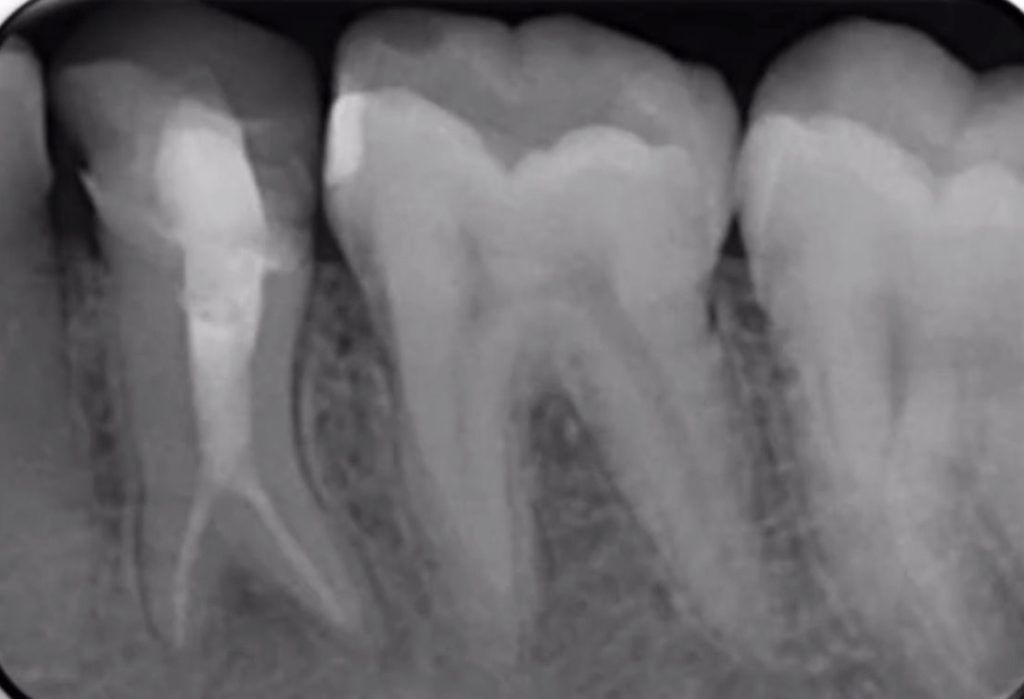
Clinical and Radiographic Findings: Clinical assessment revealed sensitivity to percussion and palpation of the buccal mucosa. The initial periapical radiograph showed a short, poorly compacted previous filling and a distinct periapical radiolucency measuring approximately 3 mm in diameter. A radiolucent area along the distal root contour strongly suggested an uninstrumented canal. The diagnosis was Chronic Apical Periodontitis secondary to inadequate root canal treatment. Figure 1: Initial periapical radiograph showing inadequate obturation and apical radiolucency.

Fig. 2
Under adequate local anesthesia and strict rubber dam isolation, the existing restoration and coronal gutta-percha were removed. The access cavity was refined, and initial exploration under the DOM confirmed only one centrally positioned, previously treated orifice. The pulp chamber floor was systematically explored by troughing the lingual developmental groove using hand files (Mani,Inc). This crucial step successfully localized a distinct, separate, and untreated lingual canal orifice, confirming a true Vertucci Type IV bifurcation originating high in the middle third of the root.
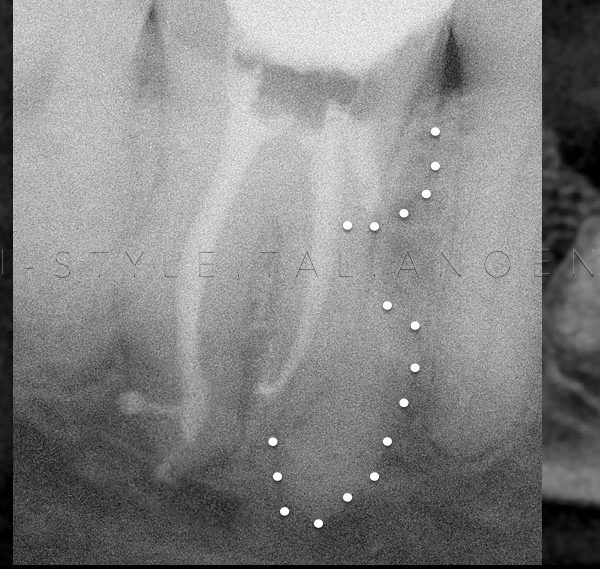
Working lengths were confirmed radiographically at 21.5 mm for both the buccal and lingual canals. (Figure 2). Figure 2: Working length radiograph confirming the Vertucci Type IV bifurcation with two separate canal diverging apically

Fig. 3
Instrumentation utilized nickel-titanium rotary files (buccal: size 30/.04; lingual: size 30/.04). Copious irrigation with heated 5.25% sodium hypochlorite (NaOCl) was enhanced by Passive Ultrasonic Irrigation (PUI) for three cycles per canal to maximize biofilm disruption. Following final rinse protocols (17% EDTA and saline), the canals were medicated with non-setting calcium hydroxide paste for one week. At the second appointment, the patient was asymptomatic. Mastercone radiograph was taken.

Fig. 4
Obturation was performed using gutta-percha and a modern bioceramic sealer via the warm vertical compaction technique, ensuring three-dimensional sealing of the two separate root canal systems. A post-endodontic core restoration was immediately placed, and the patient was referred for a definitive full-coverage ceramic crown to ensure a durable coronal seal.

Fig. 5
Clinical and radiographic follow-up was conducted at 6 and 12 months. At the 12-month review, the patient remained entirely asymptomatic. The periapical radiograph demonstrated a clear and significant reduction in the initial apical radiolucency with robust evidence of bone fill and regeneration. This confirms the successful resolution and healing of the apical periodontitis

Fig. 6
About the author:
Dr Shaili Mehta
Conclusions
This case report successfully demonstrated the non-surgical retreatment of a bifurcated mandibular second premolar (Vertucci Type IV) complicated by an undetected canal. The positive 12-month follow-up confirms complete periapical healing, underscoring the necessity of utilizing advanced magnification, ultrasonic activation, and meticulous sealing techniques for predictable long-term endodontic success in complex cases.
Bibliography
- Kottoor J, Albuquerque D, Velmurugan N, Kuruvilla J. Root Anatomy and Root Canal Configuration of Human Permanent Mandibular Premolars: A Systematic Review. Anatomy Research International 2013; 14(1):1-15.
- Vertucci F. J. Root canal morphology of mandibular premolars. The Journal of the American Dental Association. 1978; 97(1):47–50.
- Zillich R, Dowson J. Root canal morphology of mandibular first and second premolars. Oral Surg Oral Med Oral Pathol. 1973; 36:738–44.