Regenerative endodontics: a case report
07/07/2025
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Obtaining a proper seal in immature teeth is a difficult task because of the wide apical delta it presents. But regernerative endodontics gives us the chance to create pulp in the root canal out of nothing, using only common materials to ensure that the tooth continue its development in order to support its function and its sensitive response.

Fig. 1
A healthy 10 years old patient arrived in the office 2 weeks after suffering a traumatic accident while riding a bike which led to the coronal fracture of 1.1 involving enamel and dentine, creating a small opening to the pulp chamber.
The tooth had second degree mobility and was sensitive to palpation.
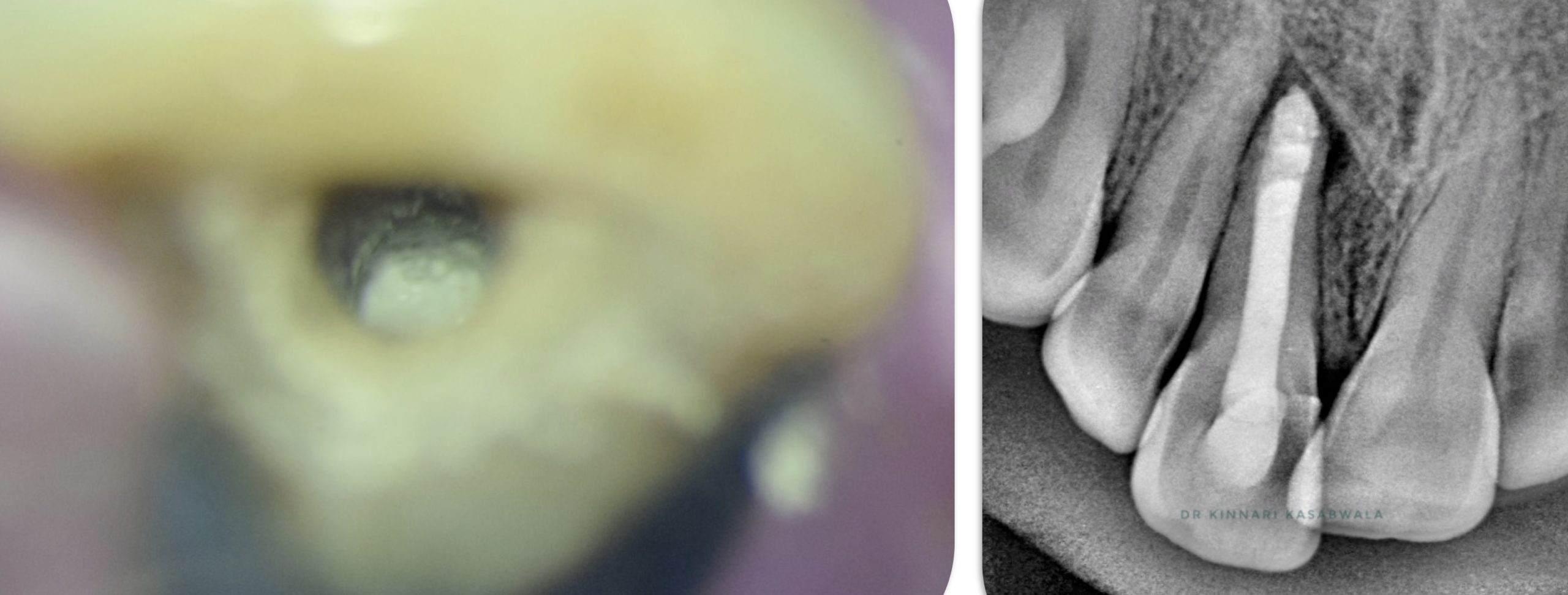
Following vitality tests and paraclinical examination pulp necrosis and subluxation are confirmed.
Treatment plan
Because an incomplete root with a large foramina is observed on the periapical radiographic image, regenerative endodontics is proposed as a treatment option to the patient and his parents. After obtaining their agreement, the treatment plan includes regenerative endodontics and also stabilization of the tooth using a flexible immobilization.

Fig. 2
Necrotic pulp is removed from the root canal using rotary files

Fig. 3
Irrigation is performed using NaOCl 5,25% and EDTA

Fig. 4
After drying, Ca(OH)2 is placed in the root canal

Fig. 5
After a month Ca(OH)2 is removed and canals irrigated with NaOCl 5,25% and EDTA.
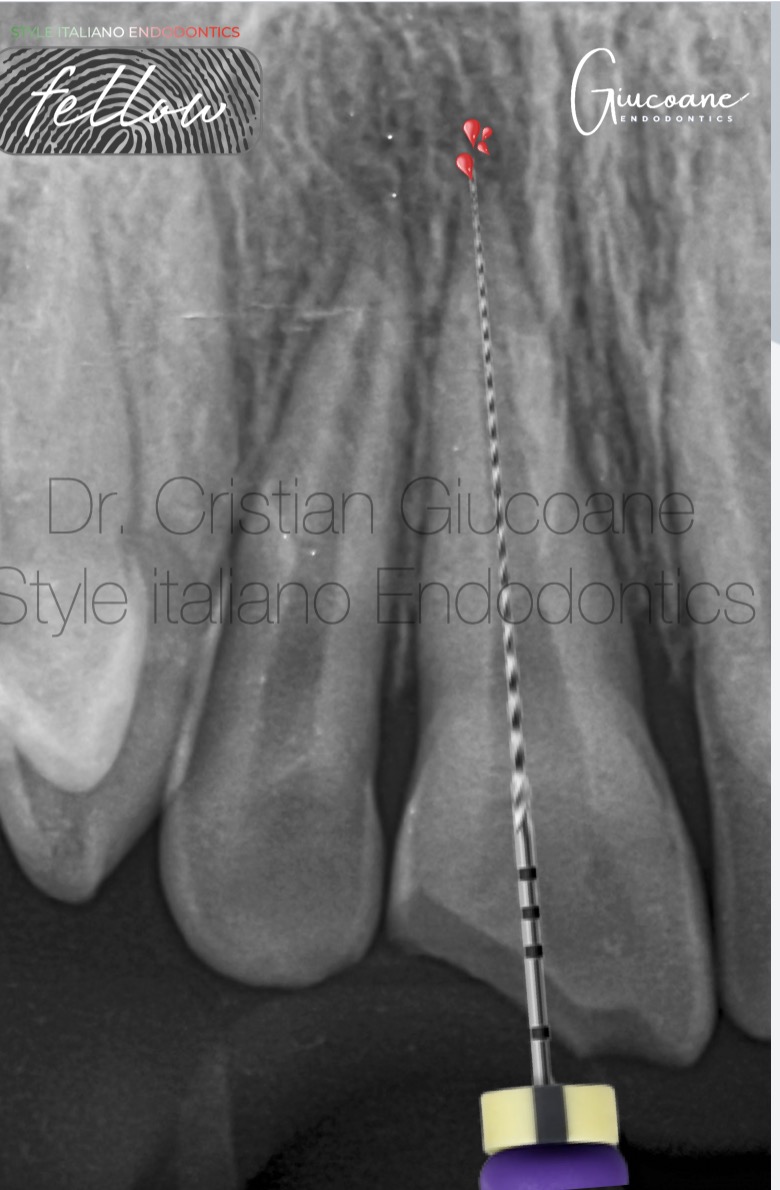
Fig. 6
After drying the canal bleeding is promoted using a #10 K-file in patency
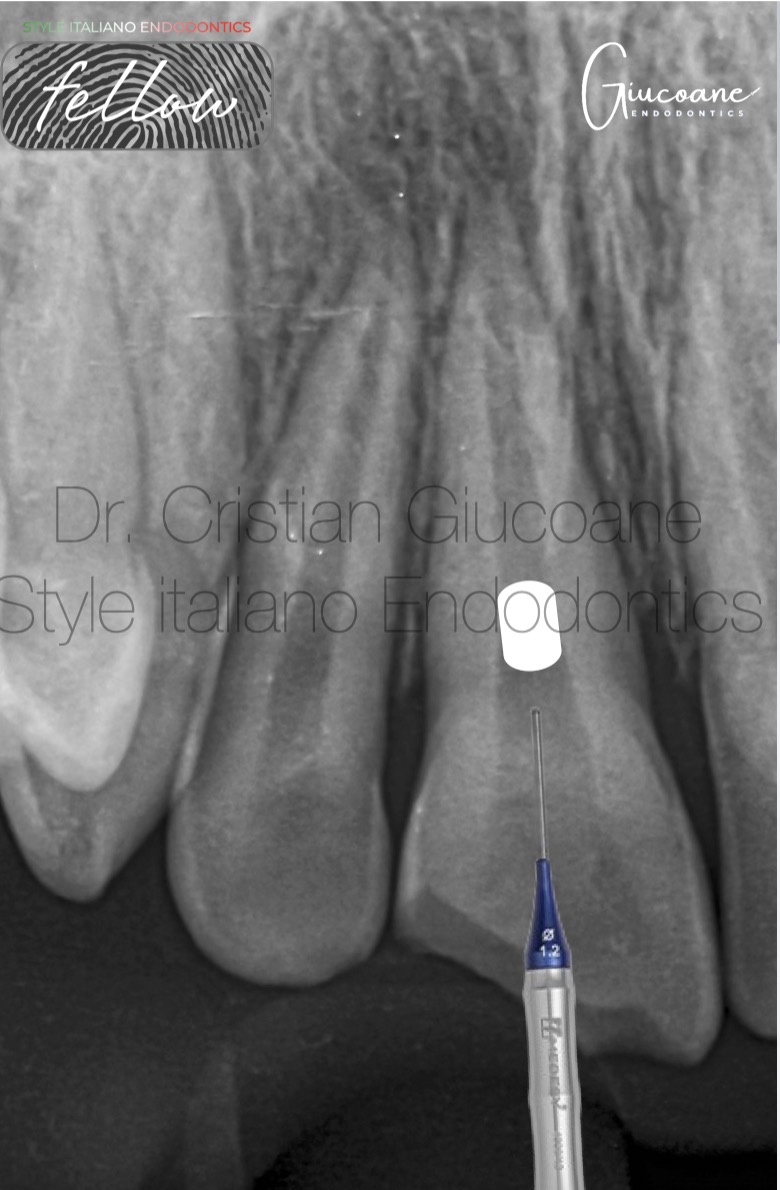
Fig. 7
A coronal plug of bioceramic putty material is placed before restoring the tooth

Fig. 8
One year follow-up shows the closing of the apical foramina
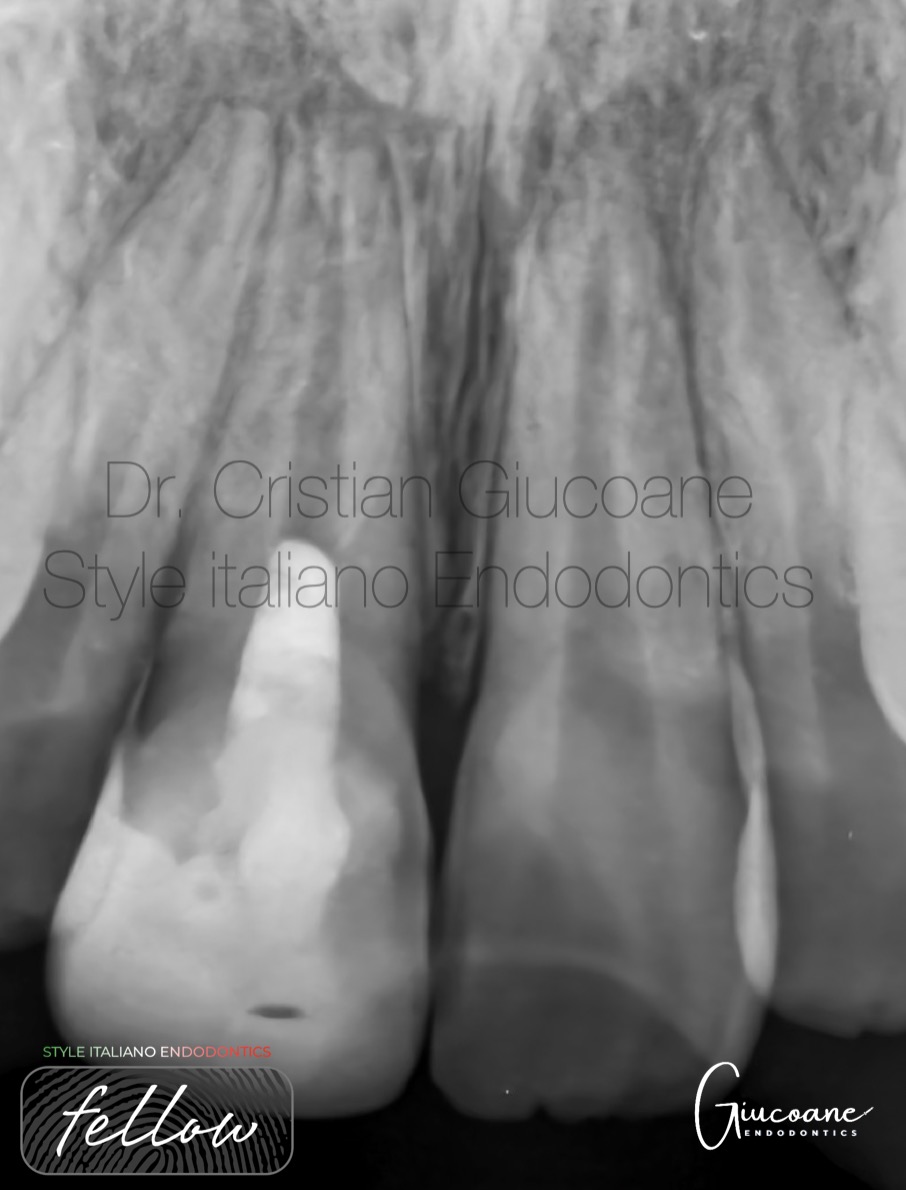
Fig. 9
3 years follow-up shows a thickening of the root canal walls.

Fig. 10
1.1 responded after 3 years to both cold test and electric test at similar values to 2.1

Fig. 11
Conclusions
Regenerative endodontics can be performed with everyday materials being a good treatment option for immature teeth where the pulp isn’t viable.
This treatment should be performed in the most aseptic conditions to offer a successful outcome.
The procedure isn’t standardized, different clinicians can use many different materials and grafts in order to obtain success in these cases.
Bibliography
1. Henry F Duncan, Lise-Lotte Kirkevang, Ove A Peters. Treatment of pulpal and apical disease: The European Society of Endodontology (ESE) S3-level clinical practice guideline. Int Endod J. 10.1111/iej.13974
2. Thanawan Jeeruphan, Jeeraphat Jantarat, Kallaya Yanpiset, Lalida Suwannapan, Phannarai Khewsawai, Kenneth M Hargreaves. Mahidol study 1: comparison of radiographic and survival outcomes of immature teeth treated with either regenerative endodontic or apexification methods: a retrospective study. J Endod. 10.1016/j.joen.2012.06.028
3. Jiacheng Lin, Qian Zeng, Xi Wei, Wei Zhao, Minyi Cui, Jing Gu, Jiaxuan Lu, Maobin Yang, Junqi Ling. Regenerative Endodontics Versus Apexification in Immature Permanent Teeth with Apical Periodontitis: A Prospective Randomized Controlled Study. J Endod. 10.1016/j.joen.2017.06.023