Well lodged-in
08/11/2024
Federico Foschi
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Nickel-titanium (NiTi) files are an essential component of modern Endodontics, primarily used for root canal shaping due to their flexibility, shape memory, and efficiency in navigating complex root anatomies. However, one of the main issues affecting NiTi files is their potential to fracture or “separate” within the canal, a complication that can impact the treatment outcome and, in severe cases, lead to the need for additional procedures or even tooth extraction.
The separation rate of NiTi files is relatively low, with studies reporting incidences between 0.4% to 5%, depending on the technique, instrument type, and operator skill. These files generally fracture due to cyclic fatigue, which occurs when the instrument undergoes repeated stress in curved canals, or torsional stress, which happens if the file binds in the canal while the handpiece continues to rotate. The repeated usage of NiTi files also induces accumulation of cycling fatigue stress, for this reason single usage is highly recommend.
Modern NiTi file systems aim to reduce separation risks with design innovations such as heat treatments, variable tapers, and controlled memory technology. For example, heat treated NiTi files, reaching the martensitic state have shown improved flexibility and resistance to cyclic fatigue, enhancing safety. However torsional stress resistance may be reduced for martensitic NiTi files especially when the file developed distortions of the helical blade or when the file is significantly pushed during the pecking motion becoming engaged onto the root canal walls or even at the foramina contrsction.
Understanding the factors contributing to NiTi file separation, combined with advancements in file design, continues to help clinicians minimize risks and improve treatment success rates in endodontics.
The novel martensitic files also requires adjustment to the removal techniques as the file may shatter in smaller shards when ultrsonic removal is attempted at moderate to high power.

Fig. 1
A local general practitioner referred a 36yo female fit and healthy as in the course of primary treatment of the lower left second molar (37) a file separation occurred rendering impossible to carry on. The patient was asymptomatic, however she was highly concerned about the possibility of losing her tooth. The original referral requested removal of the file only without completing the root canal treatment. It was advised that also the medial root may have presented with potential difficulties, also the patient opted for the treatment to be finalised and completed in specialist settings.
To be noted the original status with a relatively small caries on the medial aspect of the 37 and some minimal radiolucency indicative of secondary caries on the distal aspect of the 36.

Fig. 2
The referring dentist reported that the file that had separated was a WaveOne gold primary. Knowing the characteristic of the file does help to understand the best approaches to determine the armamentarium required. Upon clinical assessment it became apparent that the access cavity needed to be slightly enlarged as the patient had minimal mouth opening, which may have contributed to the separation almost at the shaft of the instrument.
The initial attempt to remove was using carried out using Stieglitz forceps, however the significant engagement suggested the need for some ultrasonication to favour the disengagement.
Despite minimal power utilised (<6 on Action P5 XS), as aware of the malleability of the the martensitic alloy, small shards of files started to separate. This occurrence can reduce the chances to remove the file with the main approach which is the pulling technique.

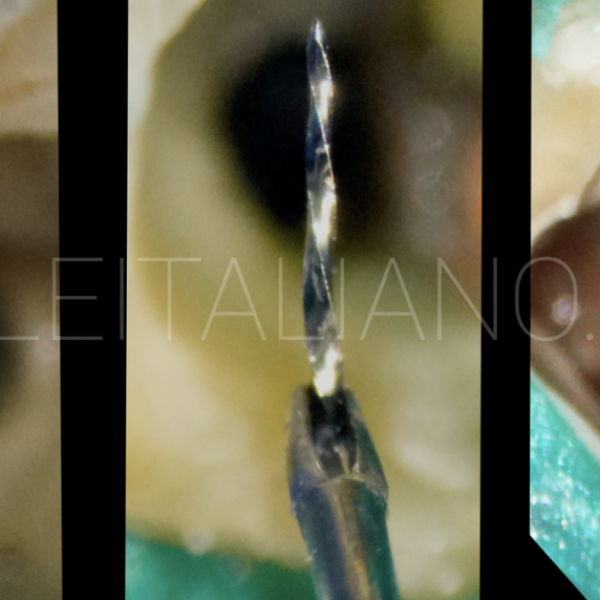
Fig. 3
Ultimately the removal was achieved with careful ultrasonic troughing around the file avoiding contacting it using an et20 (more indicated than the usual et25 as limited mouth opening and orifice level preparation). This allowed enough grasping with an hollow cannula and reverse screw type system to engage the corona/portion of the fragment. Compared to the Stieglitz approach this approach allows lesser slippage due to the malleability of the martensitic alloy.

Fig. 4
Once the file was removed the root canal treatment has been completed fairly uneventfully, the medial canals being significantly curved on the clincial and non-clinical plane. As recommended to the referring dentist the chances of separation were still high also on the mesial root ( to err is human, to persist is diabolical).

Fig. 5
The post-operative long cone periapical revealed a certain dentine removal at the orifice level of the distal canal to facilitate with the troughing the engagement with the hollow needle systems, otherwise the tooth appeared not compromised and has been asymptomatic for 3 years now.
Conclusions
When approaching file removals it is important to try and understand the type of file that separated. In case the referring dentist can provide this information the selection of the best armamentarium is facilitated.
Nevertheless the armamentarium should be comprised of all the main systematics (i.e. Stieglitz, ultrasonic unit with tips of various length, loops and hollow needle systems)
The characteristics of martensitic NiTi discourage the use of ultrasonic at high power as this can lead to further separation in to smaller fragments.
Bibliography
Sattapan, B., Nervo, G. J., Palamara, J. E., & Messer, H. H. (2000). Defects in rotary nickel-titanium files after clinical use. Journal of Endodontics, 26(3), 161-165.
Parashos, P., & Messer, H. H. (2006). Rotary NiTi instrument fracture and its consequences. Journal of Endodontics, 32(11), 1031-1043.
Iqbal, M. K., & Kohli, M. R. (2007). A retrospective clinical study of incidence of root canal instrument separation in an endodontics graduate program: A PennEndo database study. Journal of Endodontics, 33(5), 591-594.