

The endodontic ledge: causes and management
07/08/2024
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
As endodontists we often encounter retreatment cases with procedural errors such as canal blockages, ledges, instrument fractures and perforations.
The ledge is defined as an iatrogenic deviation from the original canal path that does not communicate with the periodontal ligament. The presence of a ledge prohibits the files from reaching the canal terminus, resulting in an underprepared canal. The apical part will then harbor bacteria, leading to development or persistence of apical periodontitis, which means failure of the treatment.
A ledge is formed due to several reasons:
-presence of coronal interferences that direct files in the wrong direction. These interferences can be in the access cavity or in the coronal part of the canal.
-incorrect working length leading to the accumulation of debris in the apical part and the formation of a ledge if stiff instruments are used to try to overcome the blockage.
-Shaping errors such as using rigid non flexible instruments and/or forcing them into the canal.
-presence of a curvature.
This article aims at describing the management of retreatment case where the challenge was the presence of a ledge.
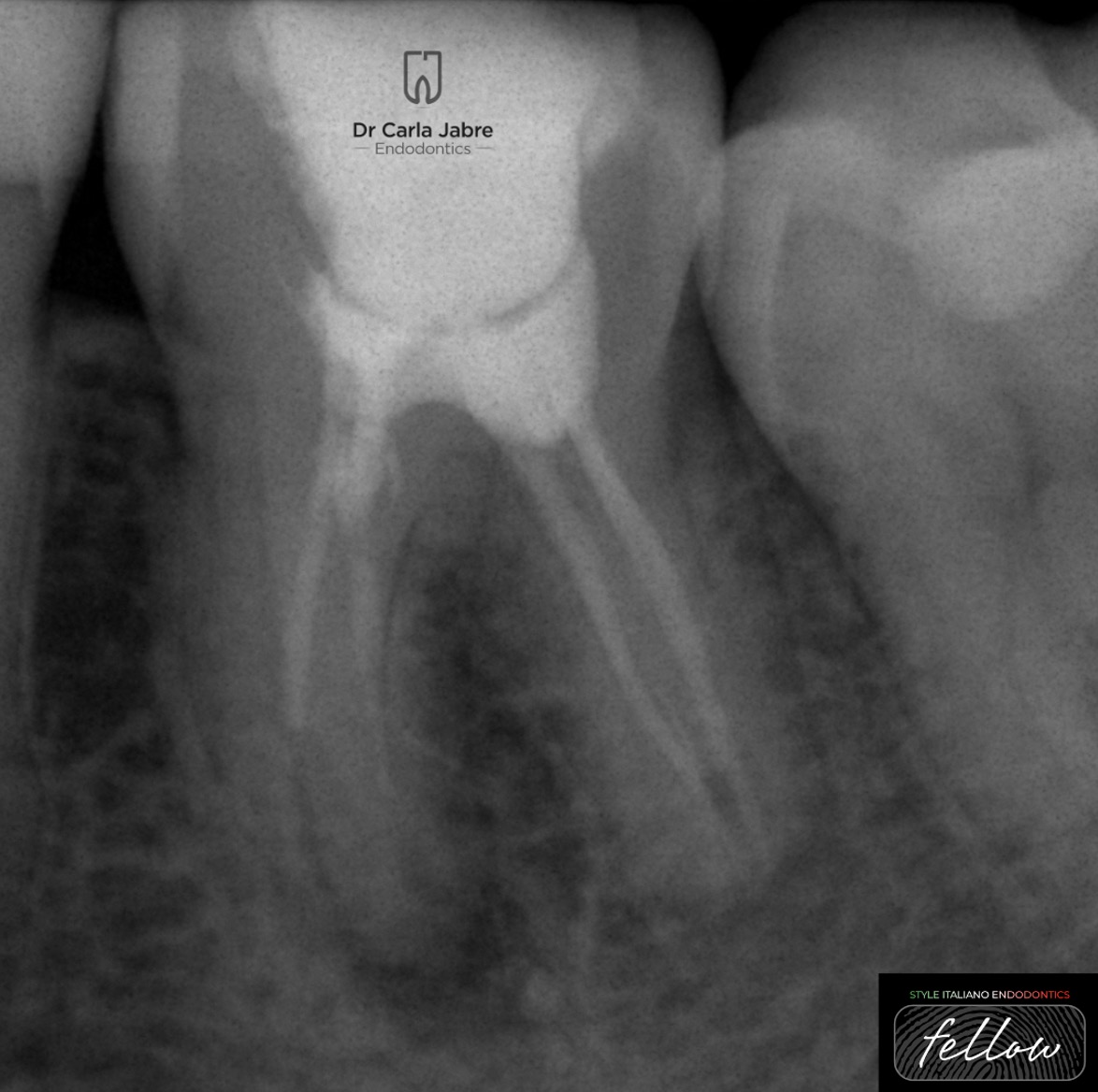
Fig. 1
A 30 year old female patient was referred for the retreatment of tooth 36. The tooth was asymptomatic. The patient recalled having a root canal treatment almost 3 years ago.
The diagnosis was made: previously treated tooth with asymptomatic apical periodontitis.
After anesthesia and rubber dam placement, the composite filling was removed and the access cavity refined using ultrasonic tips.
Gutta-percha removal was done using rotary files while copiously irrigating with sodium hypochlorite to flush away debris.
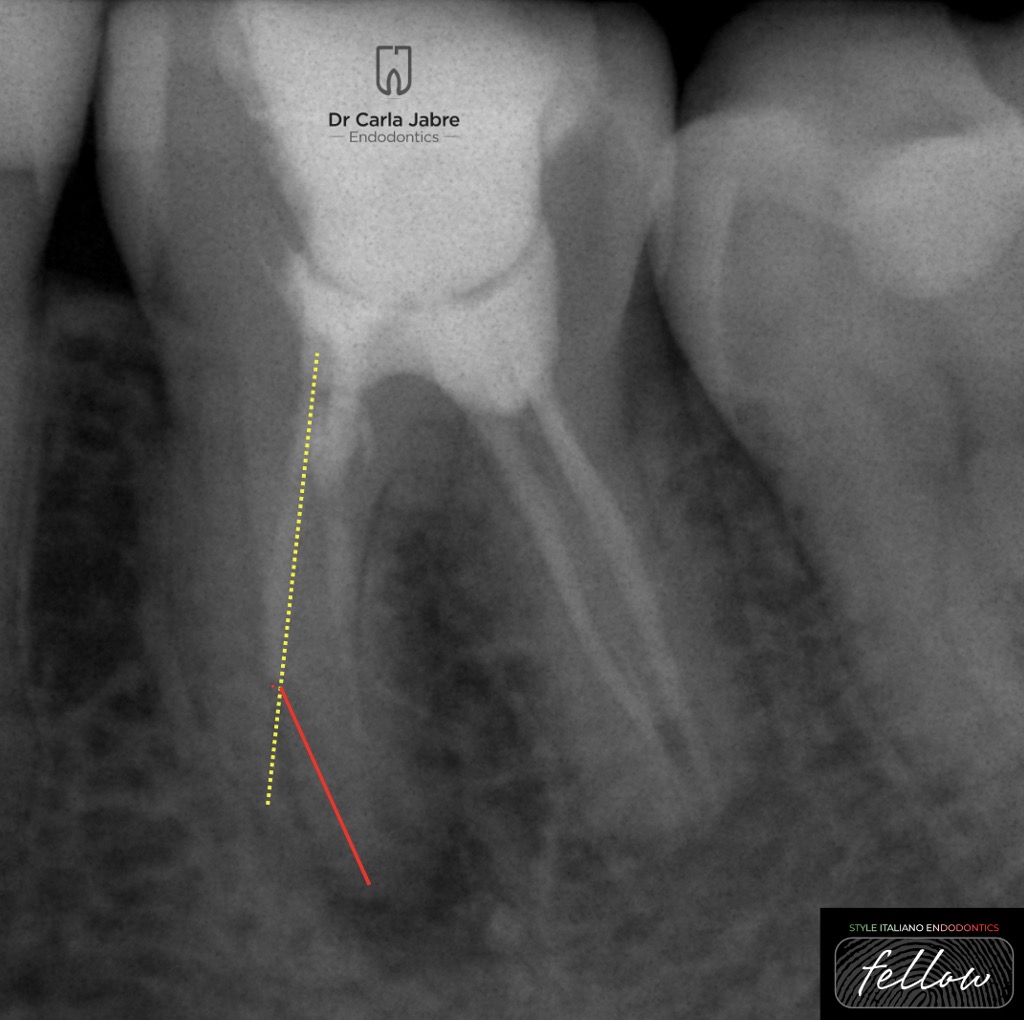
Fig. 2
Looking at the initial radiograph, the presence of a ledge can be predicted because the filling material seems to be going in a straight line, not following the root’s curvature.
After removal of the old filling material, a 10 k file was used to scout the canals to the foramen. The DL, DB and MB were easy to negotiate. However, a blockage was felt in the ML canal as if the instruments were hitting a solid wall.
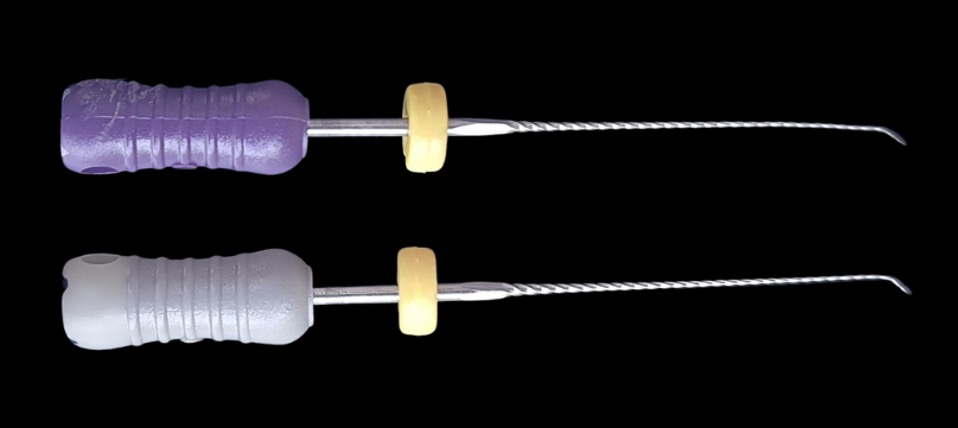
Fig. 3
The first step was to enlarge the coronal part 1mm shorter of the length reached by the 10 K file to remove all coronal interferences.
Then a pre-bent 08 K file was used to locate the canal lumen.
The search for the canal lumen was made by directing the tip of the file towards the inner wall, because ledges are usually located on the outer wall of the canal. It is advised to have rubber stoppers with directional signs to be able to direct the files toward the inner wall.
When the canal lumen was found, and without removing the K file from the canal, the 08 K file was used in a watch winding motion to reach the WL. At that level, pull push movements of small amplitude were applied in order to soften the ledge.
Then a 10 K file, with the same pre-bending as the previous file, was also inserted until it bypassed the ledge, and pull push motion was applied as previously described.
The pull-push motions were stopped when the file became loose in the canal.

Fig. 4
Then to shape the apical part, controlled memory NiTi files were used because they provide less canal transportation and more centering ability when compared to stainless steel manual files. In addition to that, it is less time consuming.
It is important to note that not all NiTi files can be used to bypass a ledge. The choice of instruments should be based on their ability to stay in a martensitic phase at body temperature. In this phase, the files do not return to their initial shape and can maintain the bending they are given.
To start, a rotary file of small diameter was prebent, and inserted manually past the ledge.
Inserting rotary files manually allows for better tactile sense. When the file bypasses the ledge, the endo motor is attached to it and activated.
The same process is repeated with the shaping files up to a size 25/.04

Fig. 5
After shaping, gutta percha cones were adapted and the warm vertical condensation technique was used to fill the canals.
The patient was referred back to her dentist for a final restoration.

Fig. 6
Angulated x-rays
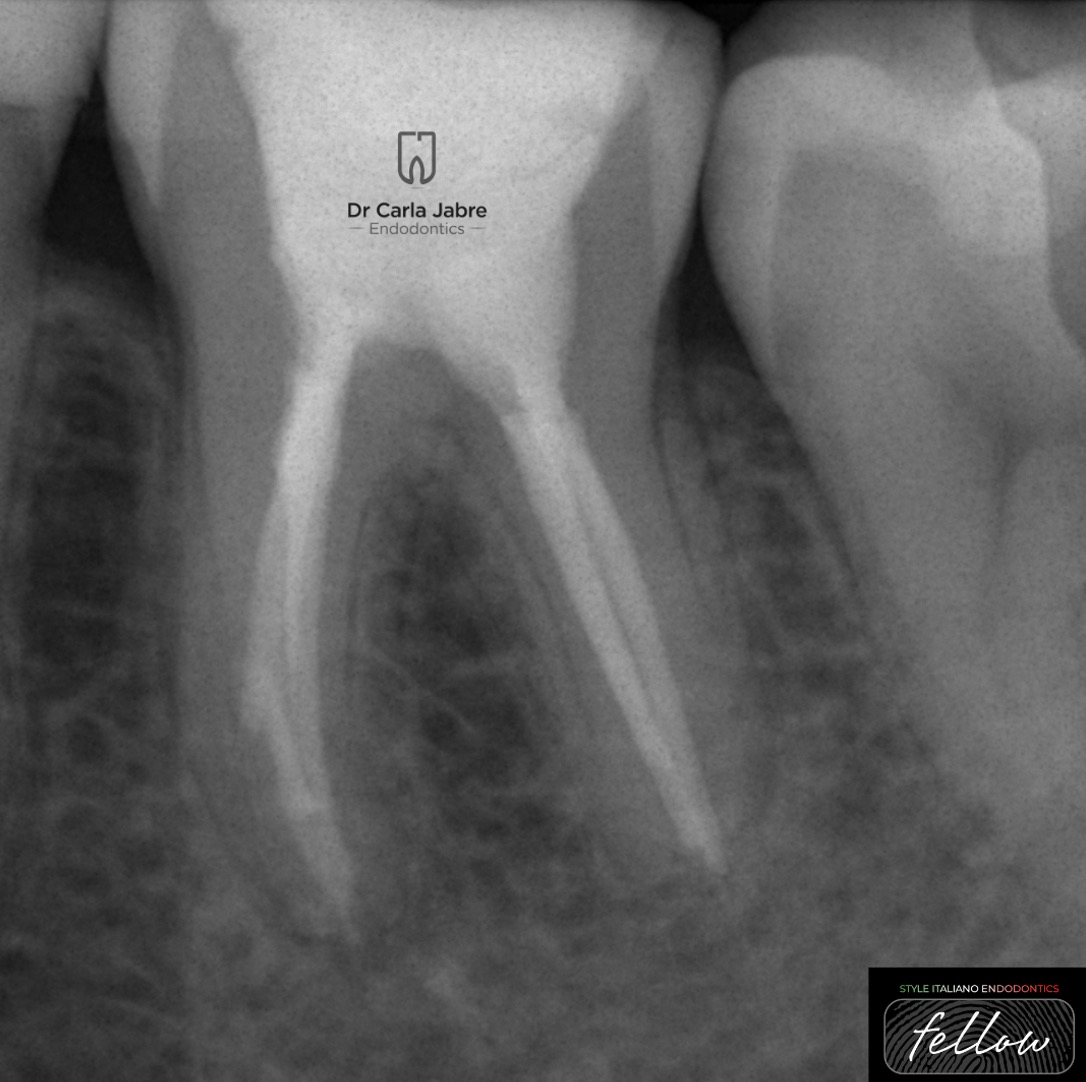
Fig. 7
Follow up at 1 year post-op shows complete healing of the lesions. The patient had refused a crown for financial reasons and only agreed to a composite filling.

Fig. 8
Fig. 7
Dr Carla Jabre
2008-2013: Undergrad studies at the faculty of Dentistry at Saint Joseph University, Beirut, Lebanon.
2013-2016: Masters in Endodontics at the faculty of Dentistry at Saint Joseph University, Beirut, Lebanon.
2018-2019: Masters in Biomaterials at Saint Joseph University, Beirut, Lebanon.
Dr Jabre has been a clinical instructor, guiding undergraduate students, in the department of Endodontics at Saint Joseph University, since 2016.
She is a member of the Lebanese Society of Endodontics, and a fellow in the Style Italiano Endodontics group.
Her private practice is limited to endodontics.
Conclusions
In conclusion, managing the presence of a ledge can be time consuming and requires a certain level of expertise. But following a step by step technique (removal of coronal interferences, finding the canal lumen with pre-bent manual files, progressive softening of the ledge, shaping) and choosing the correct instruments are keys to making the retreatment as predictable as possible.
Bibliography
Berutti et al. Micro-computed tomographic evaluation of endodontic ledge position in relation to canal curvatures. BMC Oral Health, 2022. 22:482. https://doi.org/10.1186/s12903-022-02531-5
Jafazradeh Hamid, Abbott Paul V. Ledge Formation: Review of a Great Challenge in Endodontics. J Endod 2007; 33:1155–1162. doi:10.1016/j.joen.2007.07.015
Ünlü Osman, Gürkan Güneç Hüseyin, Güneç Gürkan, Haznedaroğlu Faruk. Investigation of the efficacy of different Ni-Ti systems on acrylic blocks for correcting ledge formation. BMC Oral Health, 2023. 23:174. https://doi.org/10.1186/s12903-023-02865-8
Zanza Alessio, Reda Rodolfo, Testarelli Luca. Endodontic Orthograde Retreatments: Challenges and Solutions. Clinical, Cosmetic and Investigational Dentistry 2023:15 245–265.



