Re-treatment Decoding part 2: MB2, the most hated canal
23/09/2024
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Root canal treatment usually fails when the treatment is carried out inadequately. The most common reason for failure is usually missed anatomy and the most missed canal is the MB2 related to upper first molars, especially when it have a separate portal of exit.
The clinical should have the knowledge and equipment to deal with such cases in a proper way for a long-term successful treatment.
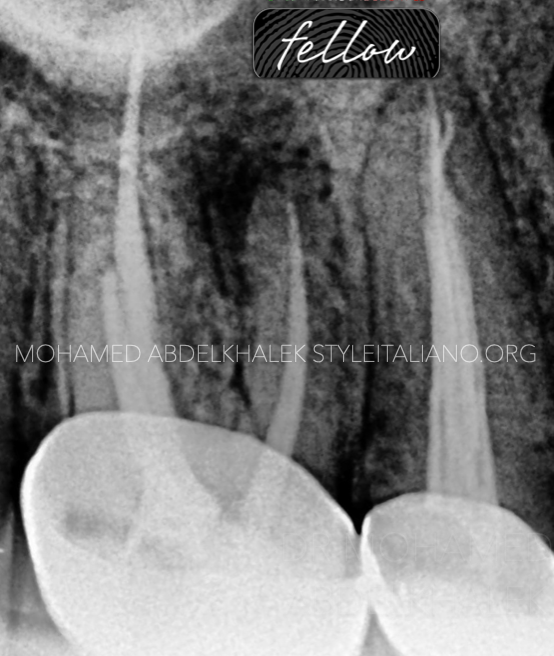
Fig. 1
A patient came to my office complaining about tenderness on chewing related to the upper first molar.
We start with a pre-operative radio-graph to diagnose in a proper way and find out the following.
1. Large peri-apical lesion related to the mesial system
2. Short obturation related to the distal system
3. Non-hygienic crown as a final restoration
4. Short obturation of the palatal canal

Fig. 2
Crown removal was the first step in the treatment showing improper cutting level of the gutta-percha and un-removed caries and severe gingival inflammation.
Upon the following givens our usual suspect here is a missed MB2, one of the most helpful tools is the CBCT radio-graph was done for precise location of the missed canal

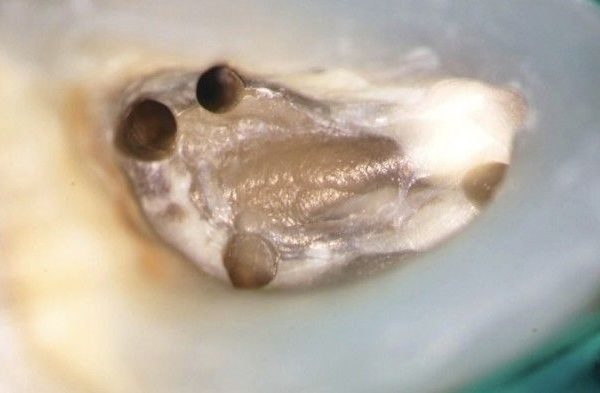
Fig. 3
Once we are sure of the missed MB2, the next step is locate them to clean it mechanically and chemically.
First of all, we remove all excess of gutta-percha from the floor, then we correct the access cavity for better visualization (this step is carried out with ultrasonics to be more precise and conservative).
Secondly, a manual file is used in a pecking motion in the suspected canal location, k-file size #10 is mostly used but I prefer short 18mm canal locators as D-finder for better tactile sensitivity in this cases.
Once the file drop in the canal, I confirm with a peri-apical x-ray
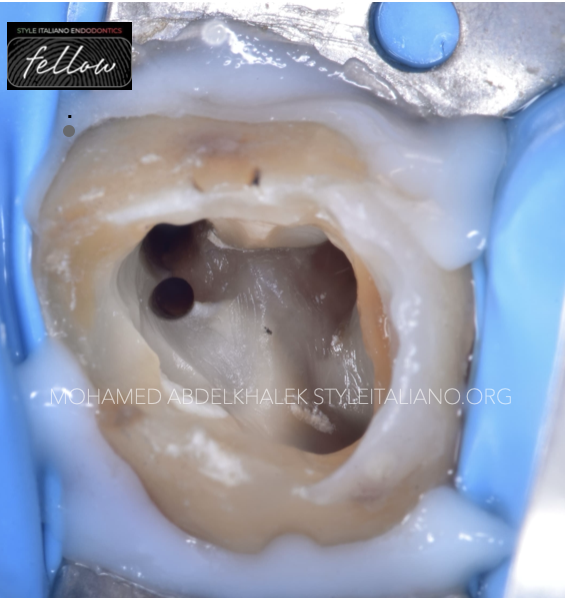
Fig. 4
MB2 shaping must be done carefully to avoid file separation, ledges or incomplete shaping. A dentinal shelf is usually present in the coronal part of the canal, preventing the clinician from achieving glide-path; to overcome this obstacle, coronal flaring using orifice openers or large tapered files in the first 3 mm will help in getting the patency easier.
In the canal enlargement procedure, the first file is usually glide-path file size 14 taper 4 then gradually 20,25 and finally 30 taper 4 respectively.
Now, after doing the most essential part in the treatment, disassembling all the filling materials in all the canals, proper shaping and cleaning protocol have to be done to achieve optimum outcome.
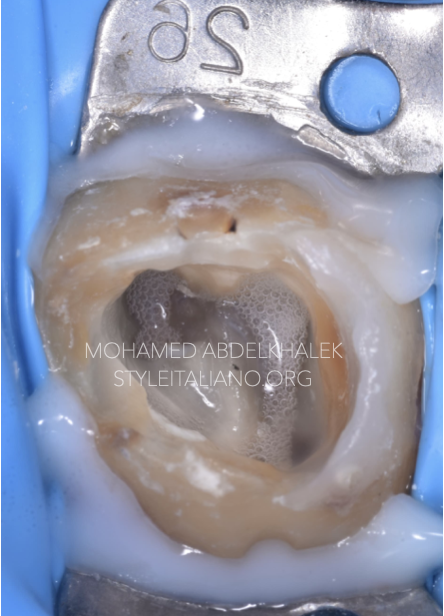
Fig. 5
30 taper 4 was the master file in the mesial and distal system while 35 taper 4 was in the palatal canal.
Copious irrigation using sodium hypochlorite fully concentrated was held along the treatment.
Final irrigation for proper chemical cleaning using sodium hypochlorite, EDTA and sterile water between each one for separation was done twice and sonic activation for 30 seconds.
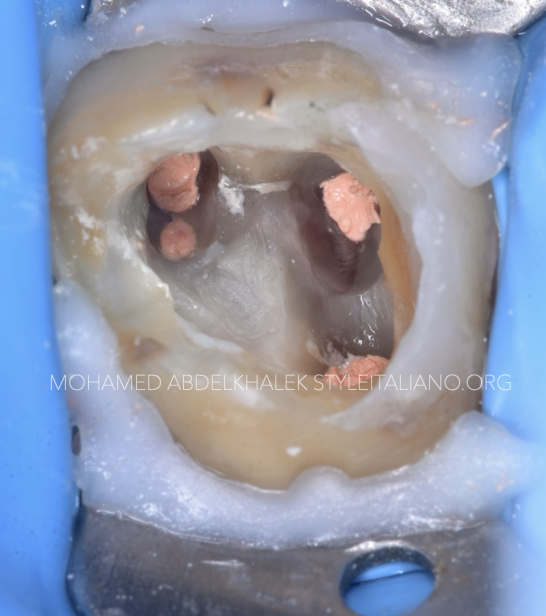
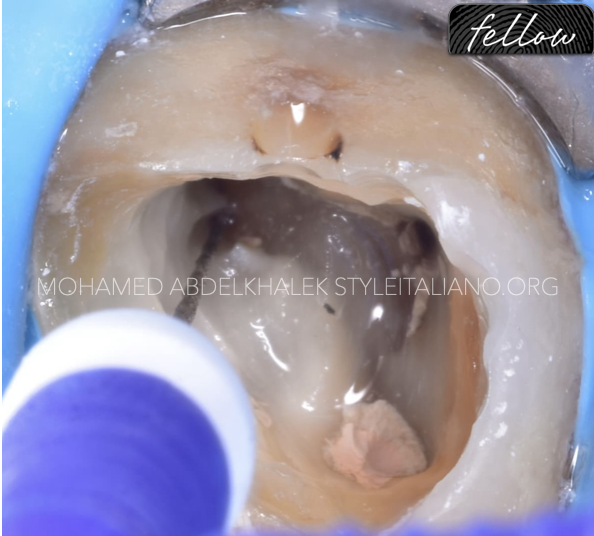
Fig. 6
Obturation was done using resin-based sealer by warm vertical compaction ( WVC ) technique in all the canals. The pulp chamber floor is clean and ready for coronal seal.

Fig. 7
Post-operative radiograph showing good obturation adequate to the working length in all canals, with 2 separate portal of exits in the mesial root.
Coronal seal was done, the tooth is now ready for post- endodontic final restoration.

Fig. 8
About the author:
Mohamed Abdelkhalek
I'm a dentist was born and raised in Alexandri, I'm really passionate about endodontics and digital dentistry.
Proudly I'm providing elite services to my patient, also have been sharing knowledge with other colleagues in webinars and local conferences.
EDUCATION
2012- 2017
University of Pharos
WORK EXPERIENCE
Dental derma dreams
Full time conservative dentist related to microscopic and digital dentistry
Advanced endodontic in Mazen dental clinic
Microscopic dentist
Digital dentistry
ADA certificate in endodontics
Co-founder@dentaldermadreams.eg
Conclusions
Endodontic re-treatments are extremely strategy-based procedures.
MB2 may not be easy to find and treat, but with good knowledge and suitable tools it can be managed predictably and with good long-term results.
Bibliography
Louis J. Buhrley, DMD, Michael J. Barrows, DDS, MS, Ellen A. BeGole, PhD, and Christopher S. Wenckus, DDS , Effect of Magnification on Locating the MB2 Canal in Maxillary Molars, Journal of Endodontics 2002
Marcelo Santos Coelho, Mariane Floriano Lopes Santos Lacerda et Al. Locating the second mesiobuccal canal in maxillary molars: Challenges and solutions, Clinical,cosmetic and Investigational Dentistry 2018
Adham A.Azim BDS, Katharina A.Azim,MA,Med Allan S.Deutsch, DMD, and George T.-J. Huang, DDS, MSD,Dsc Acquisicion of Anatomic Parameters Concerning Molar Pulp Chamber Landmarks Using Cone-beam Computed Tomography, JOE 2014
Lieutenant Commander Bernard H. Hofmann, DC, USNR and Captain Jeffrey R. Thorpe, DC, USN, Location of the second mesiobuccal canal of maxillary molars in endodontic therapy, Naval Postgraduate Dental SchoolNational Naval Dental Center Bethesda, Maryland December 2002.
Paul Krasner, DDS, and Henry J. Rankow, DDS Anatomy of the Pulp-Chamber Floor, Journal of Endodontics
Mitchell H. Davich, DMD, FACD, FICD The MB2 Canal: Following the Map of the Pulpal Floor, Endodontic therapy Vol 5 Nr 2
Leena Smaldi, BDS, MDentSci, FDSRCS(Ed) and Ameen Khraisat, BDS, PhD, Detection of a second mesiobuccal canal in the mesiobuccal roots of maxillary first molar teeth, University of Jordan
Louis J. Buhrley, DMD, Michael J. Barrows, DDS, MS, Ellen A. BeGole, PhD, and Christopher S. Wenckus, DDS , Effect of Magnification on Locating the MB2 Canal in Maxillary Molars, Journal of Endodontics 2002
Marcelo Santos Coelho, Mariane Floriano Lopes Santos Lacerda et Al. Locating the second mesiobuccal canal in maxillary molars: Challenges and solutions, Clinical,cosmetic and Investigational Dentistry 2018
Adham A.Azim BDS, Katharina A.Azim,MA,Med Allan S.Deutsch, DMD, and George T.-J. Huang, DDS, MSD,Dsc Acquisicion of Anatomic Parameters Concerning Molar Pulp Chamber Landmarks Using Cone-beam Computed Tomography, JOE 2014
Lieutenant Commander Bernard H. Hofmann, DC, USNR and Captain Jeffrey R. Thorpe, DC, USN, Location of the second mesiobuccal canal of maxillary molars in endodontic therapy, Naval Postgraduate Dental SchoolNational Naval Dental Center Bethesda, Maryland December 2002.
Paul Krasner, DDS, and Henry J. Rankow, DDS Anatomy of the Pulp-Chamber Floor, Journal of Endodontics
Mitchell H. Davich, DMD, FACD, FICD The MB2 Canal: Following the Map of the Pulpal Floor, Endodontic therapy Vol 5 Nr 2
Leena Smaldi, BDS, MDentSci, FDSRCS(Ed) and Ameen Khraisat, BDS, PhD, Detection of a second mesiobuccal canal in the mesiobuccal roots of maxillary first molar teeth, University of Jordan