

Vital Pulp Therapy: Part 1: Direct Pulp Capping for A Traumatic Exposure of Permanent Maxillary Right Central Incisor
22/04/2021
Ahmed Alwaidh
Warning: Undefined variable $post in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Pulp inflammation or exposure may occur as a result of many reasons like carries, trauma, or over-zealous preparation. However, if left untreated, this may lead to pulpits, pulp necrosis, and then apical periodontitis, which means more cost and chair-time spent. In addition, more tooth structure loss would jeopardise the survival rate and the outcomes of the treatment.
A 9 years old female presented with her father complaining of a fractured maxillary central incisor (UR1) due to trauma. They reported that she felt out a half hour ago when she was playing, and they came straight away.
Clinically, UR1 was with fractured crown, while UL1 was intact.

Fig. 1
Occlusal view, pin point pulp exposure of UR1. Both central incisors had no mobility, but both were tender to percussion and palpation.
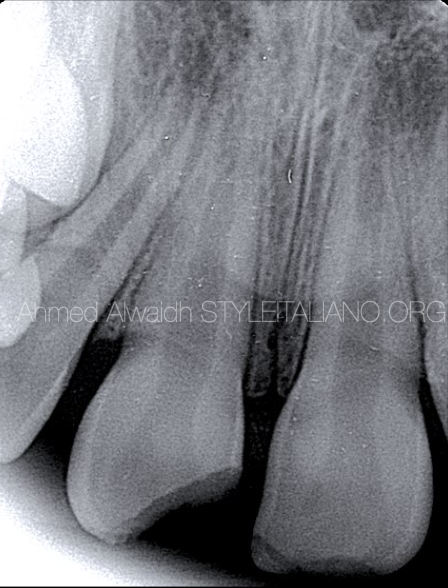
Fig. 2
Pre-operative IOPA showing incomplete root formation of UR1. There was no evidence in the radiograph of root fractures.

Fig. 3
After isolation with rubber dam, the borders were polished with a rubber cap to smoothen the edges and removing any sharpness.

Fig. 4
The exposure site was disinfected with NaOCl 2%, then and a small sterile cotton pallet soaked with NaOCl 2% was applied on the exposure site for 3 minutes. There was no bleeding after that.

Fig. 5
The exposure site was capped with White MTA (Produits Dentaires SA, Vevey, Switzerland).

Fig. 6
After its primary setting, The white MTA been covered with a layer of Glass ionomer cement (GIC) and left for 10 minutes to set.

Fig. 7
Luckily the patient brought the tooth fragment, which has been disinfected with NaOCl 2%. A small cavity been prepared in the inner aspect of the fragment to allow space for the capping material.

Fig. 8
The fragment then been cemented into its place using dual cure composite.

Fig. 9
Clinical situation of two weeks recall. The patient was symptom free, no tenderness to percussion, and UR1 responded normally to cold test.
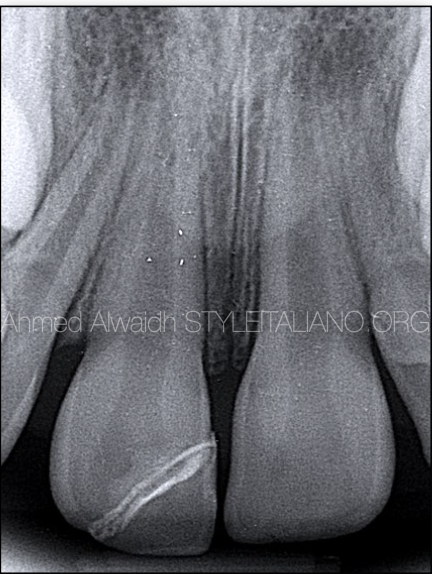
Fig. 10
wo weeks IOPA recall of UR1, showing the pulp capping material and no PA changes around the apex of UR1 compared to UL1.

Fig. 11
Clinical situation of 18 months recall, patient was symptom free, UR1 had no tenderness to percussion, normal response to cold test as compared to UL1 and UR2. Teeth were aligned properly with normal teeth eruption and development.
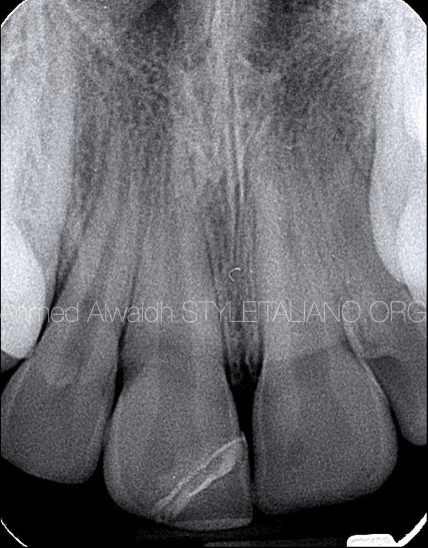
Fig. 12
18 months recall IOPA showing complete root formation of UR1 and as compared to UL1, also no evidence of peri-apical changes.
Conclusions
Vital pulp therapy (VPT) can be defined as procedures directed to preserve health of all or part of the dental pulp and aiming to maintain pulp vitality and function on one hand, and to prevent coronal and radicular tooth structure loss associated with root canal treatment on the other hand (ESE 2019).
VPT has a high success rate, but many factors have been considered critical for having favourable outcomes like a proper clinical diagnosis of the dental pulp, the cause of exposure, time of exposure, age of the patient, any previous trauma, healing capacity of the pulp tissues, size of the exposure…etc. Another important consideration is that VPT is a technique sensitive; meaning that the procedure should be excused flawlessly like good infection control, good bleeding control, and choosing a proper capping material that offers a tight seal of the exposure and being biocompatible; as it will be in a direct contact with pulp tissues.
Hydraulic calcium silicate cements like mineral trioxide aggregate (MTA), is considered on of the best materials for sealing direct pulp exposure, as they offer superior seal of the exposure site and superior histological and clinical outcomes (Aeinehchi et al. 2003, Nair et al. 2008), compared to resin based-materials which offer poor clinical outcomes due to their cytotoxicity (de Souza Costa et al. 2000, Krifka et al. 2012), and also compared to calcium hydroxide cement (Cho et al. 2013, Hilton et al. 2013, Mente et al. 2014, Kundzina et al. 2017). The only issue with MTA in pulp capping is it causes future discolouration due its content of bismuth oxide. However, the new formula white MTA (Produits Dentaire, Switzerland) doesn’t contain bismuth oxide, making it a suitable material for DPC.
In this case, all the parameters met the requirements of DPC, and the procedure was performed in a systematic precision, therefore we got a favourable outcome.
Bibliography
Aeinehchi M, Eslami B, Ghanbariha M, Saffar AS (2003) Mineral trioxide aggregate (MTA) and calcium hydroxide as pulp‐capping agents in human teeth: a preliminary report. International Endodontic Journal 36, 225– 31.
Cho SY, Seo DG, Lee SJ, Lee J, Lee SJ, Jung IY (2013) Prognostic factors for clinical outcomes according to time after direct pulp capping. Journal of Endodontics 39, 327– 31.
De Souza Costa CA, Hebling J, Hanks CT (2000) Current status of pulp capping with dentin adhesive systems: a review. Dental Materials 16, 187– 97.
European Society of Endodontology (ESE) developed by: Duncan HF, Galler KM, Tomson PL, Simon, S., El‐Karim, I., Kundzina, R., Krastl, G., Dammaschke, T., Fransson, H. and Markvart, M., 2019. European Society of Endodontology position statement: Management of deep caries and the exposed pulp. International Endodontic Journal, 52(7), pp.923-934.
Hilton TJ, Ferracane JL, Mancl L; Northwest Practice‐based Research Collaborative in Evidence‐based Dentistry (NWP) (2013) Comparison of CaOH with MTA for direct pulp capping: a PBRN randomized clinical trial. Journal of Dental Research 92, 16– 22S.
Kakehashi S, Stanley H, Fitzgerald R. The effects of surgical exposures of dental pulps in germ-free and conventional laboratory rats. Oral Surg Oral Med Oral Pathol 1965: 20: 340–349.
Krifka S, Seidenader C, Hiller KA, Schmalz G, Schweikl H (2012) Oxidative stress and cytotoxicity generated by dental composites in human pulp cells. Clinical Oral Investigations 16, 215– 24.
Mente J, Hufnagel S, Leo M et al. (2014) Treatment outcome of mineral trioxide aggregate or calcium hydroxide direct pulp capping: long‐term results. Journal of Endodontics 40, 1746– 51
Nair PNR, Duncan HF, Pitt Ford TR, Luder HU (2008) Histological, ultrastructural and quantitative investigations on the response of healthy human pulps to experimental capping with mineral trioxide aggregate: a randomized controlled trial. International Endodontic Journal 41, 128– 50.
Kundzina R, Stangvaltaite L, Eriksen HM, Kerosuo E (2017) Capping carious exposures in adults: a randomized controlled trial investigating mineral trioxide aggregate versus calcium hydroxide. International Endodontic Journal 50, 924– 32.


