
Retreatment of a maxillary premolar with missed canal
11/02/2021
Viresh Chopra
Warning: Undefined variable $post in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Success of Endodontic therapy depends upon the triad of thorough cleaning and shaping, disinfection & adequate obturation up-to the calculated working length of the root canals. Failure to follow the protocol in any of the above steps can lead to failure of the endodontic treatment. Interpretation of a preoperative radiograph is an important step in laying out a correct treatment plan. Though, they are 2 dimensional but do give us an idea of what approximate type and number of root canals we will be dealing with in a particular case. Missed canal is one of the major factors that lead to failure of the endodontic therapy. Failure to locate all the canals lead to inadequate cleaning and shaping followed with incomplete 3D obturation of the root canal system.
This case report shows a Case of Symptomatic Apical Periodontitis (SAP) with chronic abscess associated with a previous root canal treatment with inadequate obturation in a maxillary premolar.

Fig. 1
Description of the case
Patient information
- Age:30-year old
- Gender: Male
- Medical history: non-contributory
- Identification: Left maxillary second premolar (Tooth 24)
- Dental history :
Chief complaint: I am having pain when I eat or put pressure on my tooth. History of previous root canal treatment done on left upper maxillary second premolar almost 1 year back.
- Clinical examination findings: The tooth 24 is tender to percussion and had a full coverage crown.Buccal vestibule had no intraoral swelling but was tender to touch.
Preoperative radiological assessment:
The periapical radiograph revealed previous root canal treatment in 24.
The obturation is short of the radiographic apex.
Periapical radiolucency associated with the roots.
The apical part of the canals (which are unobturated), are suspected to be calcified (Fig 1).

Fig. 2
Buccal infiltration anesthesia was administered, the tooth was isolated with rubber dam isolation and the tooth was seen under the microscope preoperatively

Fig. 3
Endodontic access was prepared through the ceramic crown and older gutta perchas located.
The endodontic access cavity and the coronal part of the gutta perchas in the pulp chamber were removed with ultrasonic scaler
Gutta perchas inside the root canal were removed with the help of rotary file used at 2500rpm.
After the removal of gutta percha intracanal medicament was placed and patient recalled for second appointment

Fig. 4
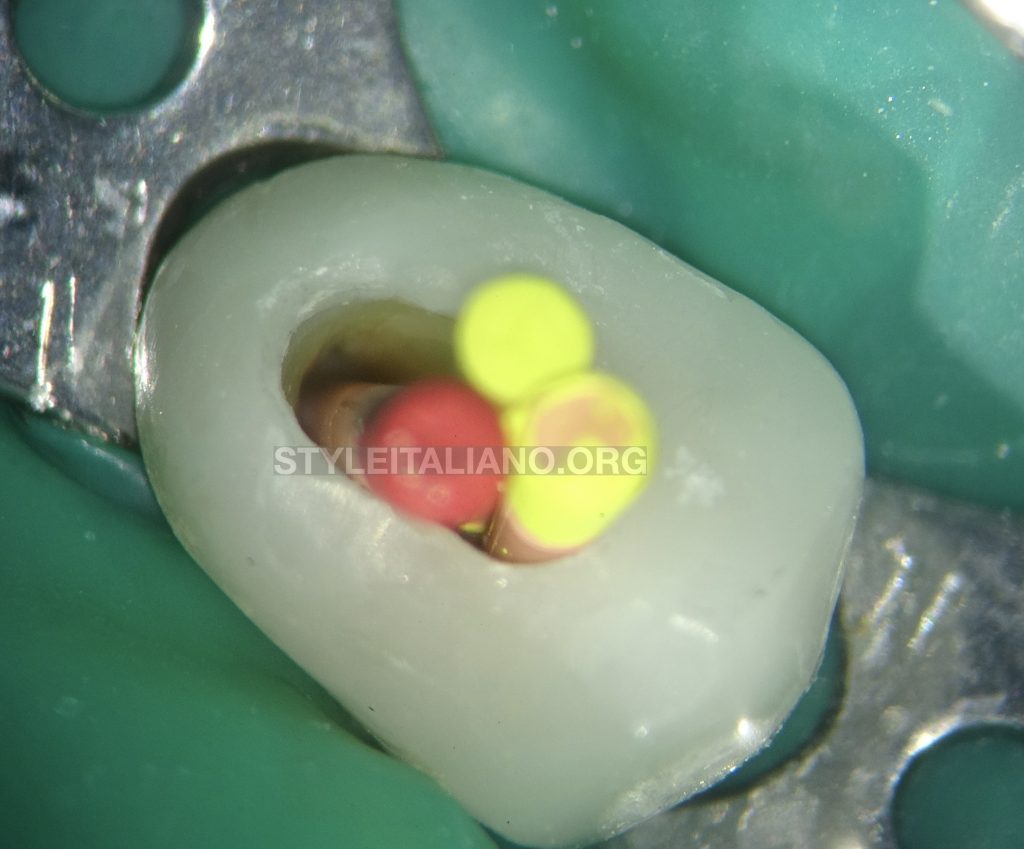
Irrigation was done to remove the intracanal medicament from the canals. 08K and 10K endodontic files were pre curved and used in an attempt to open the calcified canals. C+ files were also used in order to open up the apically calcified part of the root canals. These files were used with passive motion in presence of the irrigants. The shape of the buccal orifice was observed, and it seemed larger than the normal size and also a blood spot was visible
The buccal orifice was enlarged with ultrasonics (video 4) and an extra orifice located.

Fig. 5
10k file was used to explore the catch and radiograph taken to verify the presence of an extra canal. (DB canal)
Video of the procedure
The canals were shaped and cleaned with 25/06 size with Race Evo files (Fig 8) (video 6)
The files had to be pre-curved to clean and shape the missed DB canal. (video 7)
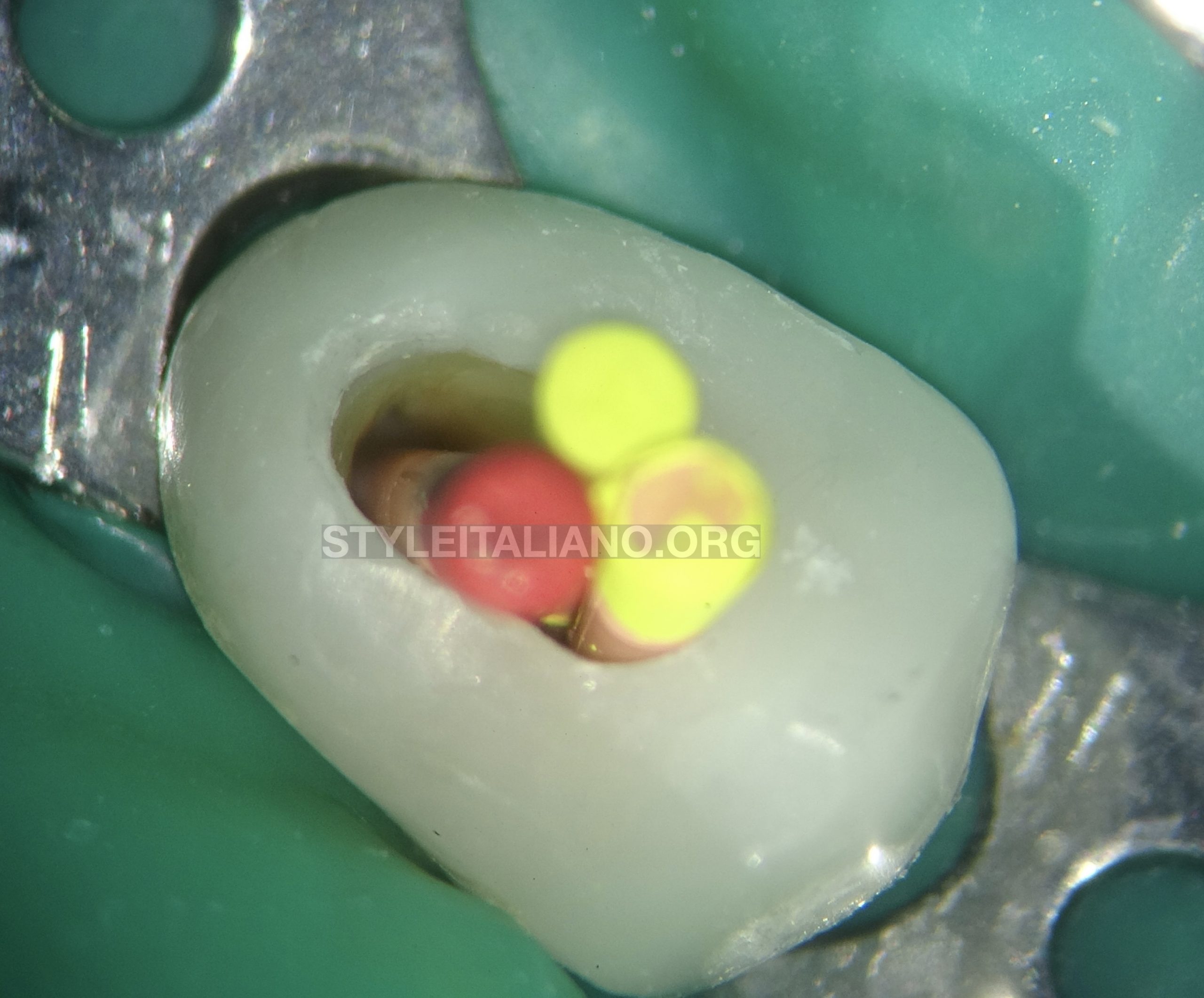
Fig. 6
Master cone verified for the cone fit. The master cones were verified on the periapical radiograph.
AH plus sealer was used and applied inside the canals. The master cones were coated with the sealer and placed inside the canals.
Warm vertical condensation technique was used to obturate the canals (Fig 9) followed with backfill filling with thermoplasticised gutta percha. (Video 8).

Fig. 7
The canals were obturated till the orifice and the pulp chamber cleaned of any gutta percha or sealer.

Fig. 8
Immediate postoperative radiograph was taken to verify the final obturation.

Fig. 9
Another PA taken after complete 3D obturation
Conclusions
In order to achieve success in endodontic treatment, root canal system needs to be thoroughly cleaned, shaped, disinfected and a 3-dimensional obturation of the root canal system should be achieved.
Inability to locate all the canals will lead to inadequate cleaning and shaping leaving residual microorganisms behind which will cause failure of the root canal treatment as seen in this case.
Therefore, all the root canals should be locate and coronally & apically sealed up to the full working length in order to achieve success in endodontic treatment.
- Learning Objectives: The reader should be able to understand:
- The importance of magnification in Endodontics.
- The significance of proper reading of the preoperative radiograph.
- The significance of a missed canal and importance of finding all the canals and treating the whole root canal system adequately to achieve success.
- The importance to use endodontic ultrasonic tips to gain reentry in the pulp chamber for retreatment.
- Not only to observe the number of canals but also to observe the shape of canal orifices.
- The need to plan/modify the treatment steps as per the clinical findings during the procedure (like in this case: the moment doubt was there because of orifice shape, ultrasonics were used to explore).
- How to decide clinically, which instrument to be used for a particular step during an endodontic treatment or retreatment.
- The importance of using the right kind of instruments to locate and negotiate the canals.
- The concepts of understanding the prognosis of the tooth and giving a try to save the tooth instead of straight away extracting it.
Bibliography
- 1.Retreatment of Endodontic fillings: Gunnar Bergenholtz Ulf Lekholm, Ralph Milthon, Gunnar Heden , Björn Ödesjö , Bure Engström;
- 2.The Outcome of Endodontic Retreatment: A 2-yr Follow-up: Fabio G.M.Gorni, Massimo M.Gagliani; https://doi.org/10.1097/00004770-200401000-00001
- 3.Nonsurgical Retreatment: Clifford J.Ruddle; https://doi.org/10.1097/01.don.0000145033.15701.2d
- 4.Determination of the Minimum Instrumentation Size for Penetration of Irrigants to the Apical Third of Root Canal Systems: Abbasali Khademi, Mohammad Yazdizadeh, Mahboobe Feizianfard;


