

Print & Try - Endodontic management of a rare case of dilacerated maxillary first molar: case report and clinical strategy
06/04/2020
Massimo Giovarruscio
Warning: Undefined variable $post in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
How much technology can support us?
Print&Try technique represents a really useful method in order to simulate the root canal treatment. Using CBCT Scan images, it is possible to extrapolate file that can be transformed into an STL model and then printed with a high definition 3d printer.
Clinicians can train on a 3D printed tooth and find the best approach in order to be more confident during the real treatment. In this article the management of a complex molar with extremely curved and long canals using Print&Try Technique will be described.

Fig. 1
Dilaceration is the result of a developmental anomaly in which there has been an abrupt change in the axial inclination between the crown and the root of a tooth3. The prevalence of root dilaceration in maxillary first molar is 15,3%1. The criteria for recognizing root dilaceration vary in the literature. According to some authors1,2, a tooth is considered to have a dilaceration towards the mesial or distal direction if there is a 90-degree angle or greater along the axis of the tooth or root. Although periapical radiographs are the most common way to diagnose the presence of root dilacerations, CBCT Scan images are very useful to understand properly the tooth anomaly and the exact position and angulation of the dilaceration4. The management of curved canals is always a challenge in endodontics due to the great difficulty with cleaning, shaping and obturating the root canal system. Predictability of treatment is ensured from knowledge and skill of the operator.
The aim of this article is to present a challenging case and endodontic explantation of the dilacerated maxillary first molar using a new generation of rotary file and Bioceramic obturation technique.
16 years old patient with 1.6 with a typical aspect of dilacerated root morphology .
The tooth responded negatively to vitality tests
The presence of lump on buccal side confirms the chronic periapical periodontitis

Fig. 2
Pre operative periapical image confirms the presence of dilacerated root and a periapical radiolucent lesion on mesio buccal root.
Radiography has an important role in the diagnosis and assessment of the irregular morphology of the root canal system, but conventional periapical provides only a 2D representation of the complex anatomy
Cone Beam Computed Tomography Scan (CBCT) provides tridimensional images of the dilacerated tooth and its surrounding tissues. This helps to determine the exact position and angulation of the dilaceration
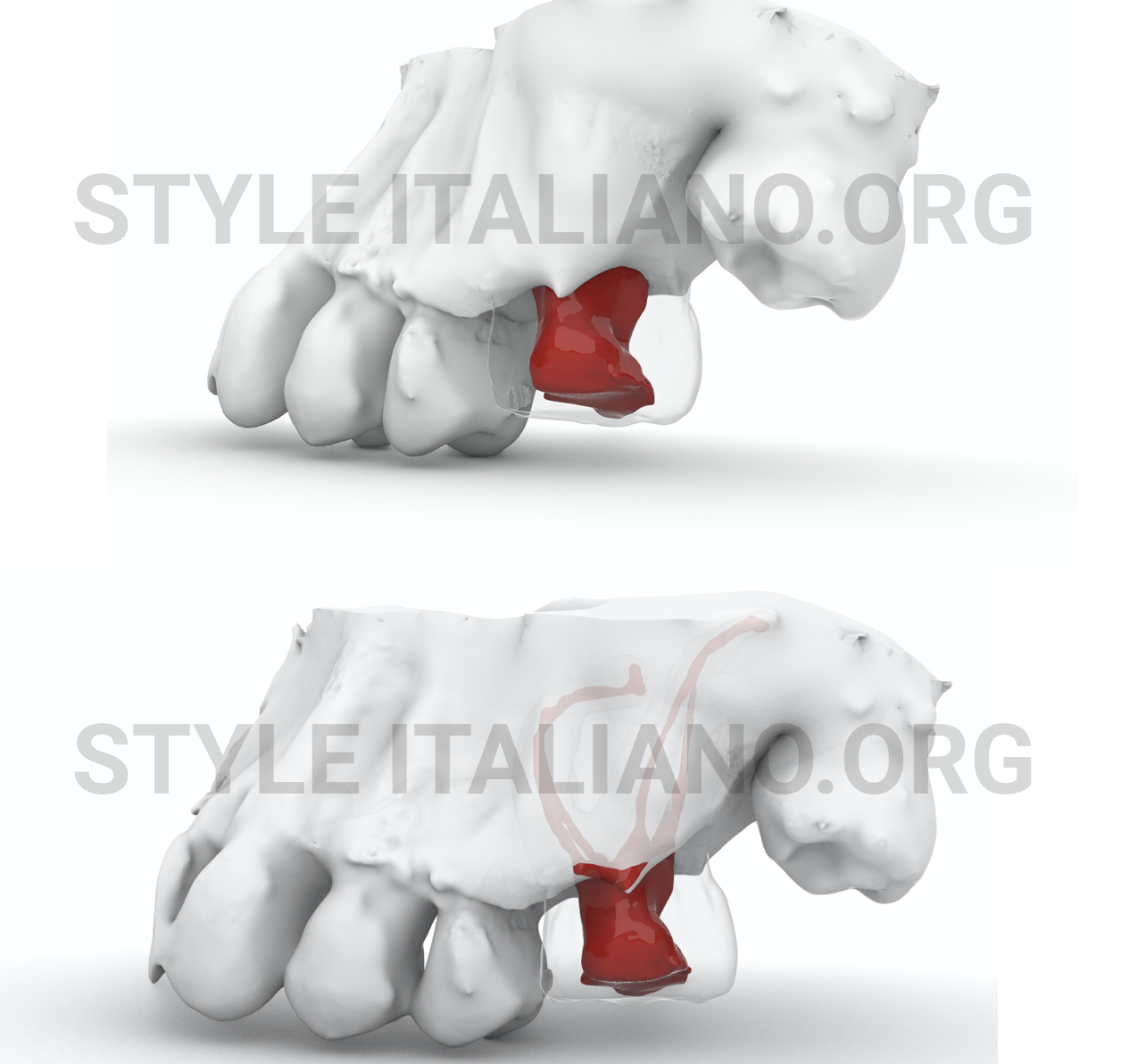
Fig. 3
The scanned volume derived from the CBCT software may allow generation of images in three planes that can be continuously scrolled through, thus allowing a three- dimensional understanding of the structure involved. They can also be converted into additional types of files.
The new types of files that can be derived from the CBCT scan is the stereo litography (STL) file. An STL file is a format used by stereoli- thography software to generate information needed to produce 3D plastic models using stereolithography machines or printers
Thanks to CBCT it is also possible to measure properly length an diameter of root canal anatomy
The CBCT data were used to produce precise 3D plastic models of the tooth. These models facilitated the treatment planning process and the trial of treatment approaches.
One can train on the plastic model in order to understand the difficulties of the case and to get ready for the real treatment.
First appointment
Access cavity design and a proper location of MB, DB and P orifice.
Ultrasonic tip has been used to remove pulp calcifications and to design carefully all the chamber anatomy. Micro Opener is also useful to find the orifices.
First appointment
Using TruNatomy Orifice Modifier, all the orifices are enlarged. TOM is a size 20/.08 at the tip. The shorter handle instruments is particularly appropriate in the earliest stages of root canal shaping. This instrument is especially useful when the canal is not vertically oriented.
Aquacare is also used to clean the chamber, in order to visualize better the entire chamber anatomy
The temporary filling has been placed and patient has been discharged
Second appointment
Canal scouting is the most important step during root canal treatment. When we scout canals it is my advice that we use a viscous chelator. This does 3 very important things: it is a lubricant, emulsifier and the debris produced is stored more affectively. The 10K-file has been used giving it a little wiggle back and forth, and that begins to pull the file down into the canal. When the handle is just snug, not tight, pull it. When you pull, you are cutting on the out stroke. You are cutting away from the terminus and importantly you are cutting the diameters.
Working Length:
D> 30mm
MB1> 27mm
P>28mm

Fig. 4
Working Length:
D> 30mm
MB1> 27mm
MB2> meets mb1
P>28mm
TruNatomy Glider (17.02) has been used in order to obtain a rotary reproducible Glide Path.
Due to the extremely curved and long canals, TruNatomy Small (20.04) has been used too.
All the canals are been prepared up to TruNatomy Prime (26.04)
Delivery of irrigating solutions is key to cleaning and debridement of the canal space. To aid in the flushing of the canal, a highly flexible plastic needle has been used. This needle has a unique, dual side-vented design. In tight spaces the needle can express fluids out either side or both. IRRIFLEX
Due to the complexity of the anatomy, the obturation technique used was Single Cone Technique and Bioceramic material.

Fig. 5
X-ray of the RCT
Post op CBCT

Fig. 6
6 months recall
Conclusions
Root canal treatment on dilacerated teeth often involves complicated procedures that require precise diagnosis, appropriate treatment planning and adequate implementation.
The printing of a transparent 3D plastic model of this tooth, with its complex anatomy, provided an effective means for defining the correct approach, surgical and not surgical.
In complex cases, 3D models can facilitate treatment planning and is also useful for education and teaching purposes.
Bibliography
1) Ana Malcˇic ́, Silvana Jukic ́, Valentina Brzovic ́, Ivana Miletic ́, Ivica Pelivan, and Ivica Anic ́. Prevalence of root dilaceration in adult dental patients in Croatia. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006;102:104-9
2) A.A. Hamasha, T. Al-Khateeb, A. Darwazeh. Prevalence of dilaceration in Jordanian adults. Int Endod J, 35 (2002), pp. 910-912
3 )Hamid Jafarzadeh, Paul V.Abbott. Dilaceration: Review of an Endodontic Challenge. Journal of Endodontics, Volume 33, Issue 9, September 2007, Pages 1025-1030
4 )A. Agnihotri, N. Marwah, S. Dutta. Dilacerated unerupted central incisor: a case report J Indian Soc Pedod Prev Dent, 24 (2006), pp. 152-154


