Middle Mesial Canal of the Mandibular First Molar: a case report
10/05/2020
João Meirinhos
Warning: Undefined variable $post in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
With increasing reports of aberrant canal morphology, the clinician needs to be aware of the possibility of having a middle mesial canal in mandibular first molars.
The purpose of this article is to report the successful treatment of a clinical case of a mandibular molar with three mesial and two distal canals.
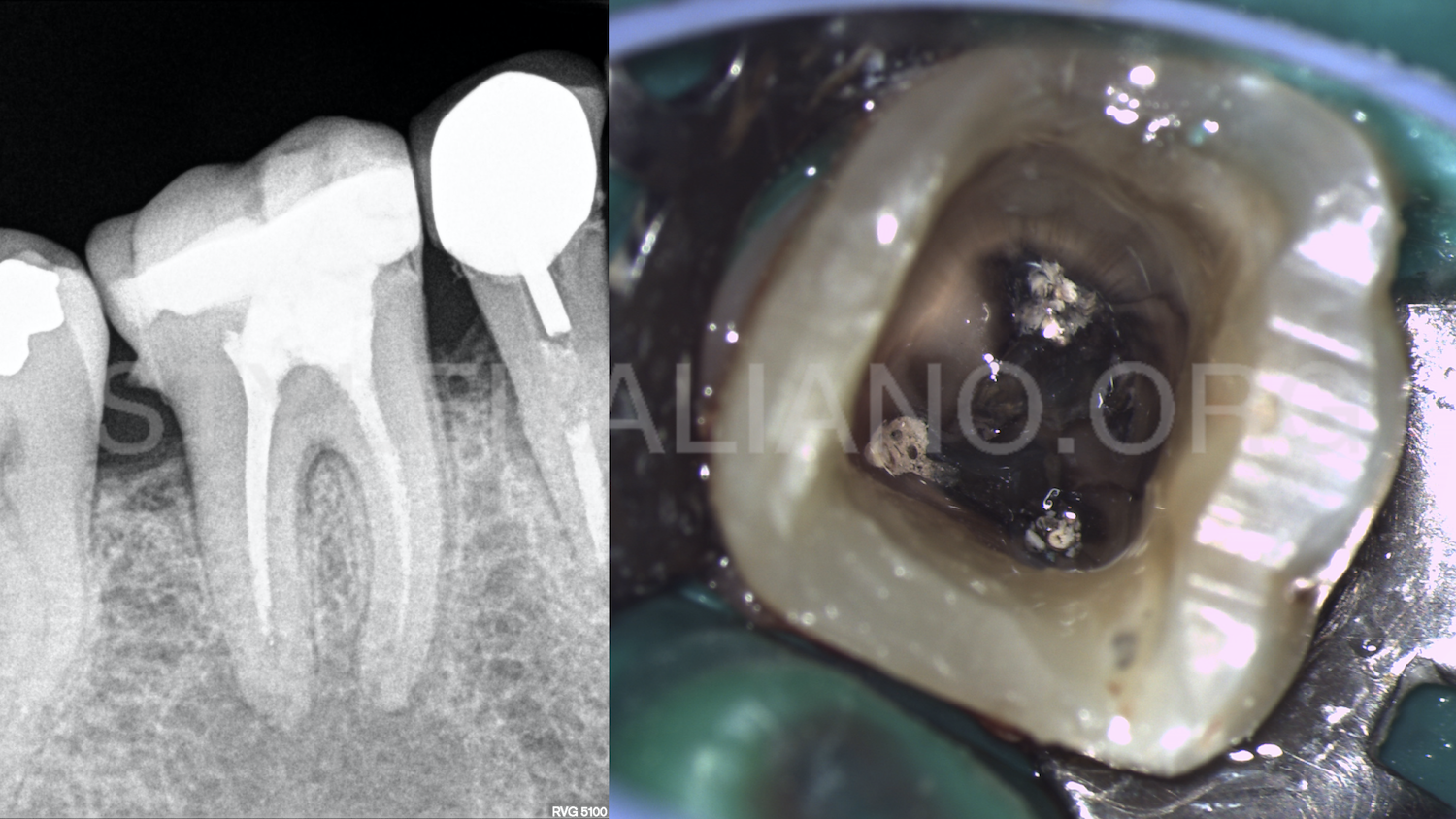
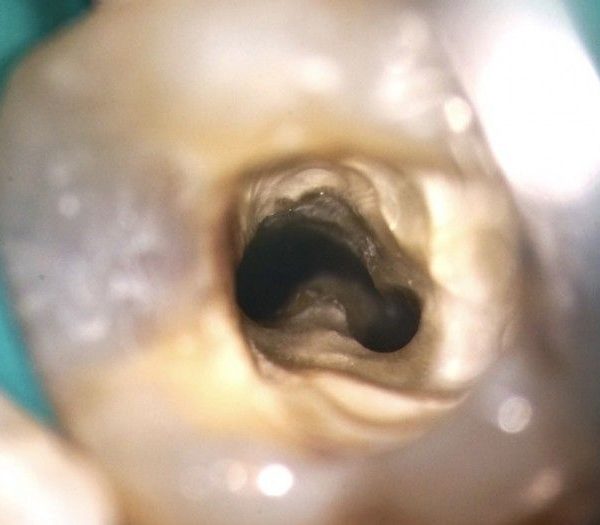
Fig. 1
A 47-year-old female patient was referred to the Postgraduate Specialization Course in Endodontics at the Faculty of Dental Medicine of the University of Lisbon (FMDUL), by a colleague from Oral Hygiene, to perform non-surgical endodontic retreatment in the first right lower molar.
Tooth 4.6 had a previous endodontic treatment and asymptomatic apical periodontitis. Probing was within normal depths in all surfaces except distolingual, where there was a localized pocket of 7mm.
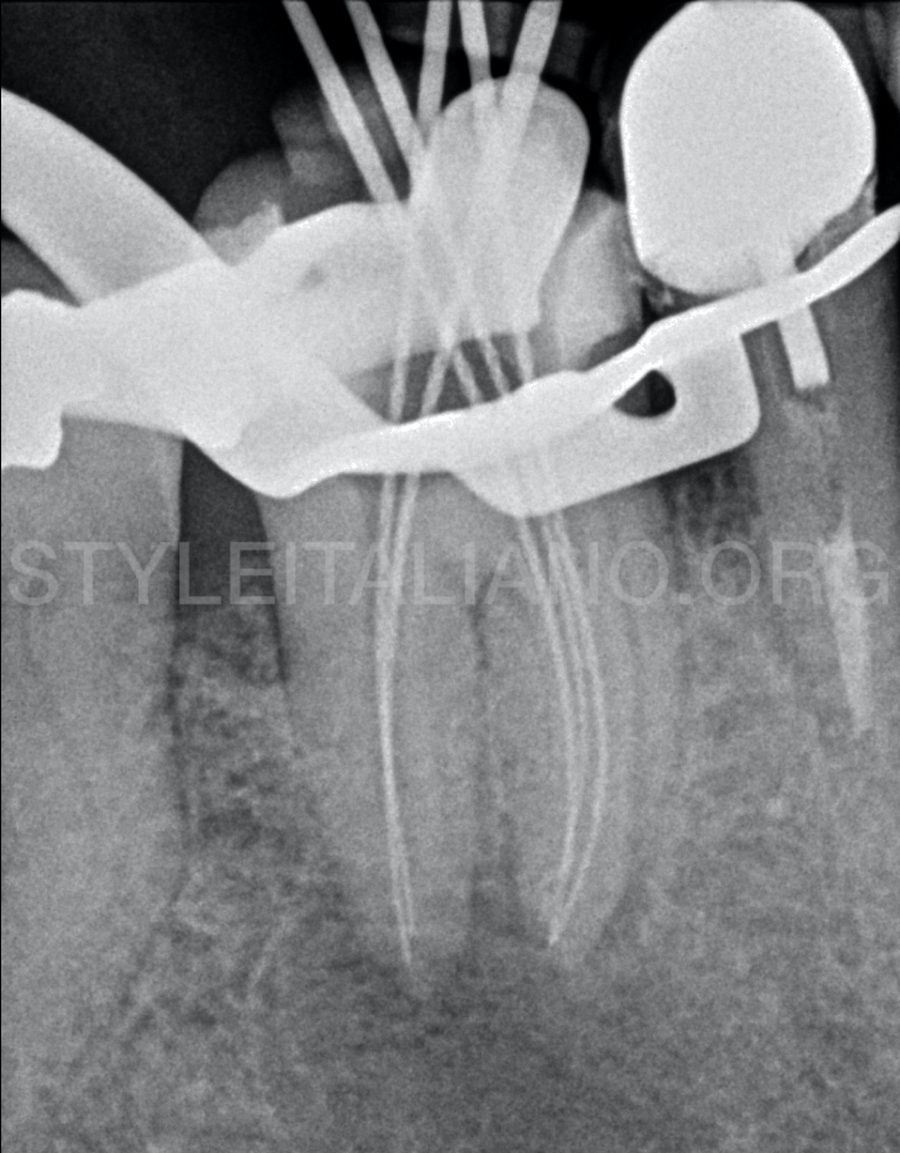
Fig. 2
As a treatment plan, non-surgical endodontic treatment was suggested. The treatment was performed under an operating microscope, in 4 appointments. Upon establishing access with Ultrasonic tips, three mesial canals were found. The canals were scouted with 10k and 15k stainless-steel hand files. To determine the working length, an electronic apex locator was also used.
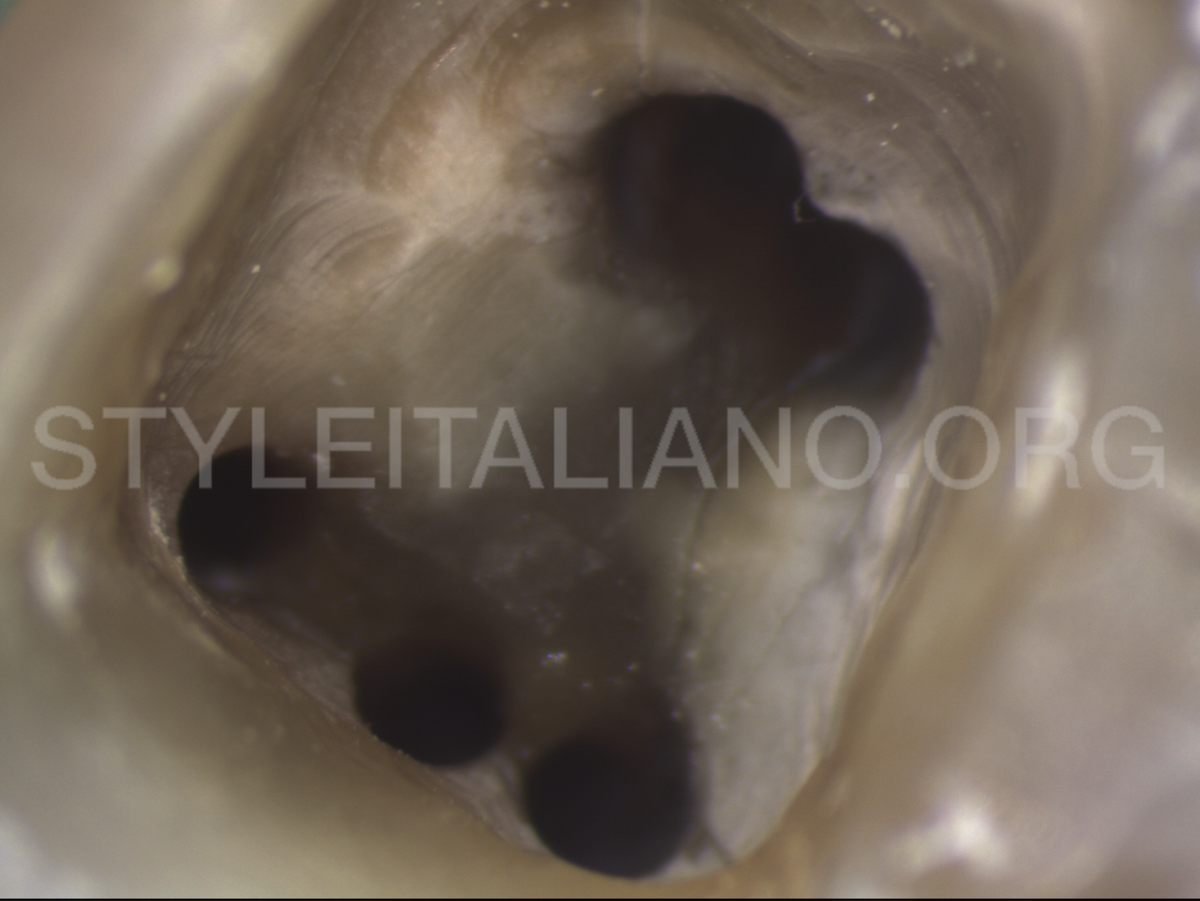
Fig. 3
All the canals were shaped with Reciproc files (r25, r40) (VDW, Germany) according to the manufacturer’s instructions.
Copious irrigation with 5mL syringe and a 27G notched needle with 5,25% sodium hypochlorite was done all throughout the endodontic treatment.
Fig. 4
The canals were dried with paper points.

Fig. 5
The root canal obturation was done with gutta-percha and resin sealer with a continuous wave of obturation technique.
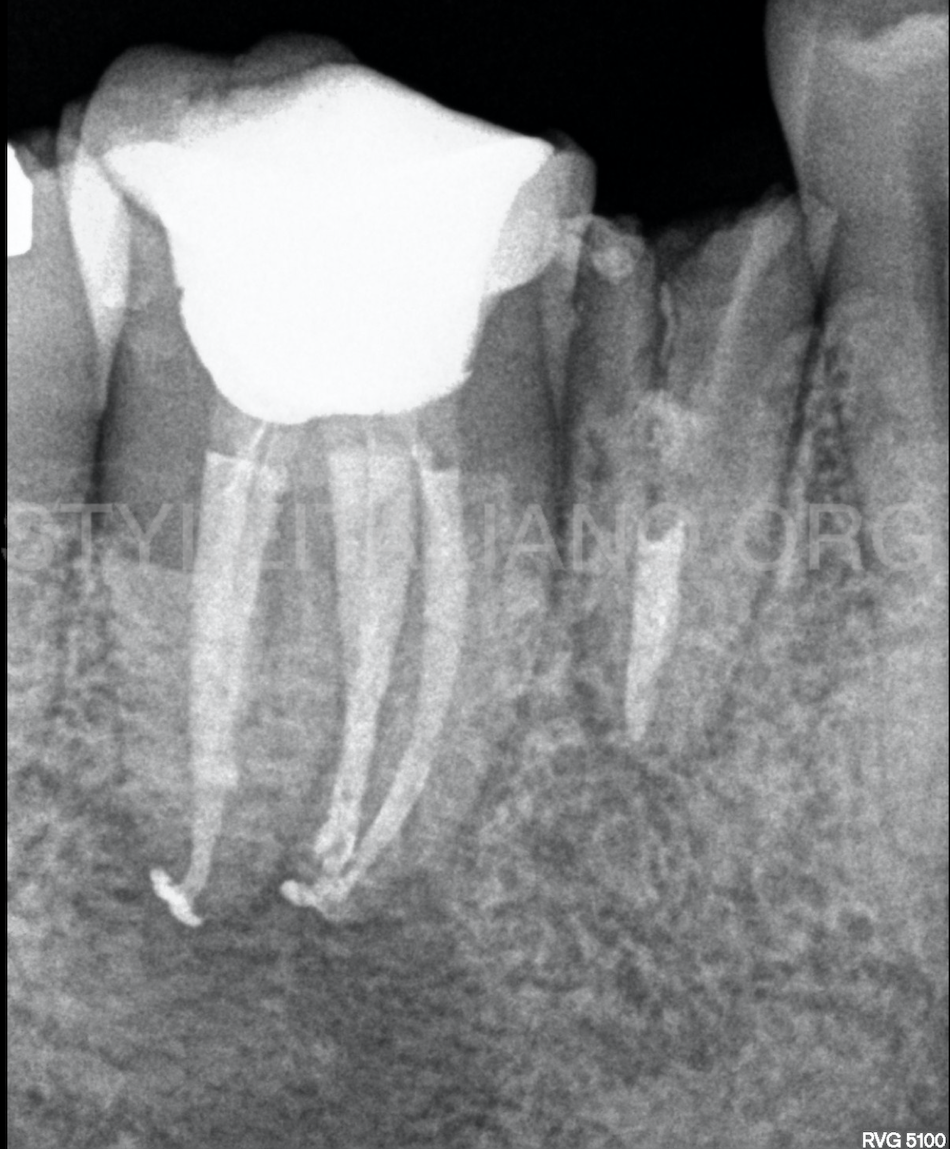
Fig. 6
A flowable composite resin was used to seal the root canal openings and the crown was subsequently restored directly with composite resin.

Fig. 7
At 12 months, the patient is completely asymptomatic and periapical radiography shows a significant decrease in the apical lesion associated to both roots.
Conclusions
Root canal morphology and configuration might present the clinician with a complex anatomy requiring more diagnostic approaches, access modifications, and clinical skills to successfully localize, negotiate, disinfect, and seal the root canal system.
Bibliography
- Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol 1984;58:589–599.
- Siqueira JF. Endodontic infections: Concepts, paradigms, and perspectives. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2002;94:281-93
- Karapinar-Kazandag, M., Basrani, B. R., & Friedman, S. (2010). The Operating Microscope Enhances Detection and Negotiation of Accessory Mesial Canals in Mandibular Molars. Journal of Endodontics, 36(8), 1289–1294.
- Gu, Y., Lu, Q., Wang, H., Ding, Y., Wang, P., & Ni, L. (2010). Root canal morphology of permanent three-rooted mandibular first molars – part I: pulp floor and root canal system. Journal of Endodontics, 36, 990–994.
- De Pablo, Ó. V., Estevez, R., Péix Sánchez, M., Heilborn, C., & Cohenca, N. (2010). Root Anatomy and Canal Configuration of the Permanent Mandibular First Molar: A Systematic Review. Journal of Endodontics, 36(12), 1919–1931.
- Akbarzadeh, N., Aminoshariae, A., Khalighinejad, N., Palomo, J. M., Syed, A., Kulild, J. C., … Mickel, A. (2017). The Association between the Anatomic Landmarks of the Pulp Chamber Floor and the Prevalence of Middle Mesial Canals in Mandibular First Molars: An In Vivo Analysis. Journal of Endodontics, 43(11), 1797–1801.