
Managing a maxillary second molar with C shaped anatomy
25/11/2020
Garima Poddar
Warning: Undefined variable $post in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
For a more predictable root canal treatment, a good knowledge of root canal systems, their anatomy and variations, serves a vital role. A failure to identify and manage a varied anatomy could lead to failure of successful endodontic treatment.
The “C- shaped” anatomy was first described by Cooke and Cox in 1979. It is named so, due to the resemblance of the root canal cross section with the alphabet “C”. The failure of Hertwig's epithelial sheath to develop or fuse in the furcation area in the developing stage of the teeth, results in this configuration in a tooth. A clinical research study published in JOE in 2016,reported the global prevalence as 1.1% for first maxillary molars and 3.8% for second maxillary molars. (3)
Using a CBCT for evaluation of such varied anatomy is helpful in predictable outcome of the endodontic therapy for such teeth.
A C shaped anatomy of maxillary molar has been found in five different types-
Type A- When there is fusion between mesiobuccal and palatal roots.
Type B- fusion between mesiobuccal and distobuccal roots.
Type C-Fusion between distobuccal and palatal roots
Type D- with 2 possible palatal roots.
Type E- mesiobuccal and palatal roots connecting with an independent distobuccal root canal at apical or between distobuccal and palatal roots connecting with an independent mesiobuccal root canal at apical level.(3)
Also, a thorough irrigation protocol for a C shaped root canal configuration is very important during root canal treatment of such teeth.
This case report is about the management of one such tooth with C shaped anatomy(type B) undergoing endodontic therapy.
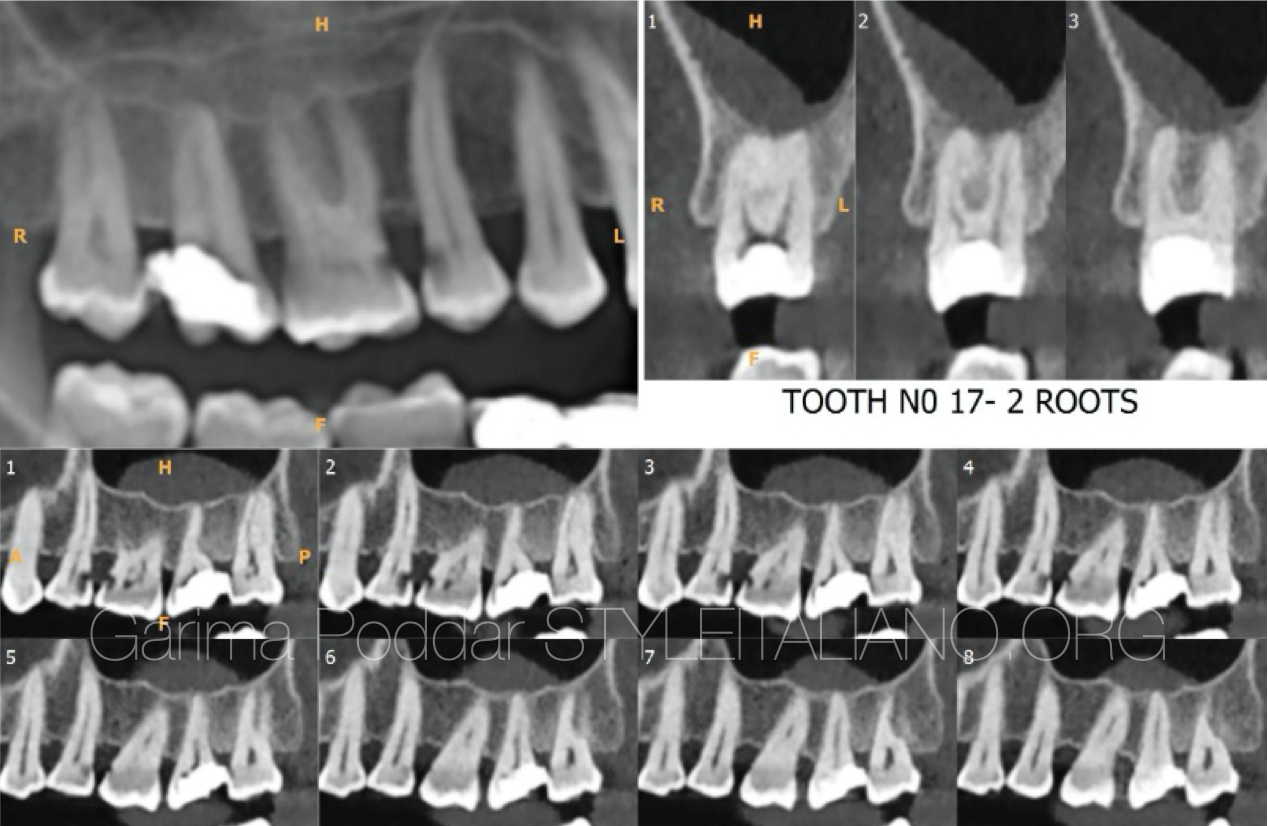
Fig. 1
A 38 years female patient was referred to our dental office by a dentist who had initiated a root canal treatment for tooth number 17 and could not find canals properly.
A CBCT was advised for this tooth, on which it was confirmed to have two roots.
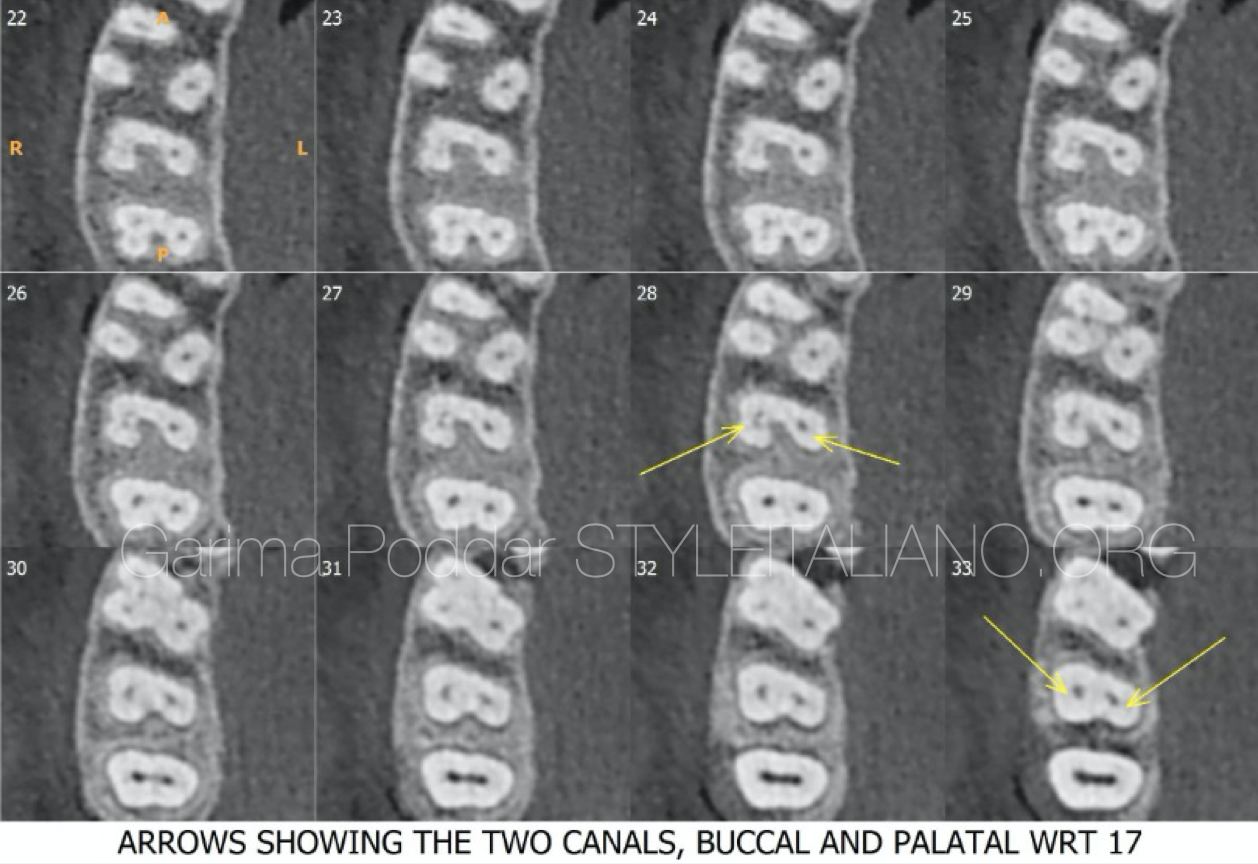
Fig. 2
The cross sectional view of cbct revealed the following details-
- In the coronal slices of cbct, two canals could be appreciated, namely – buccal and palatal.
- The buccal canal showed a C shaped cross section in the sections of middle third region and in apical region.
CBCT is a helpful tool in such cases of viaried anatomies, where certain details might be unclear on an intraoral radiograph.
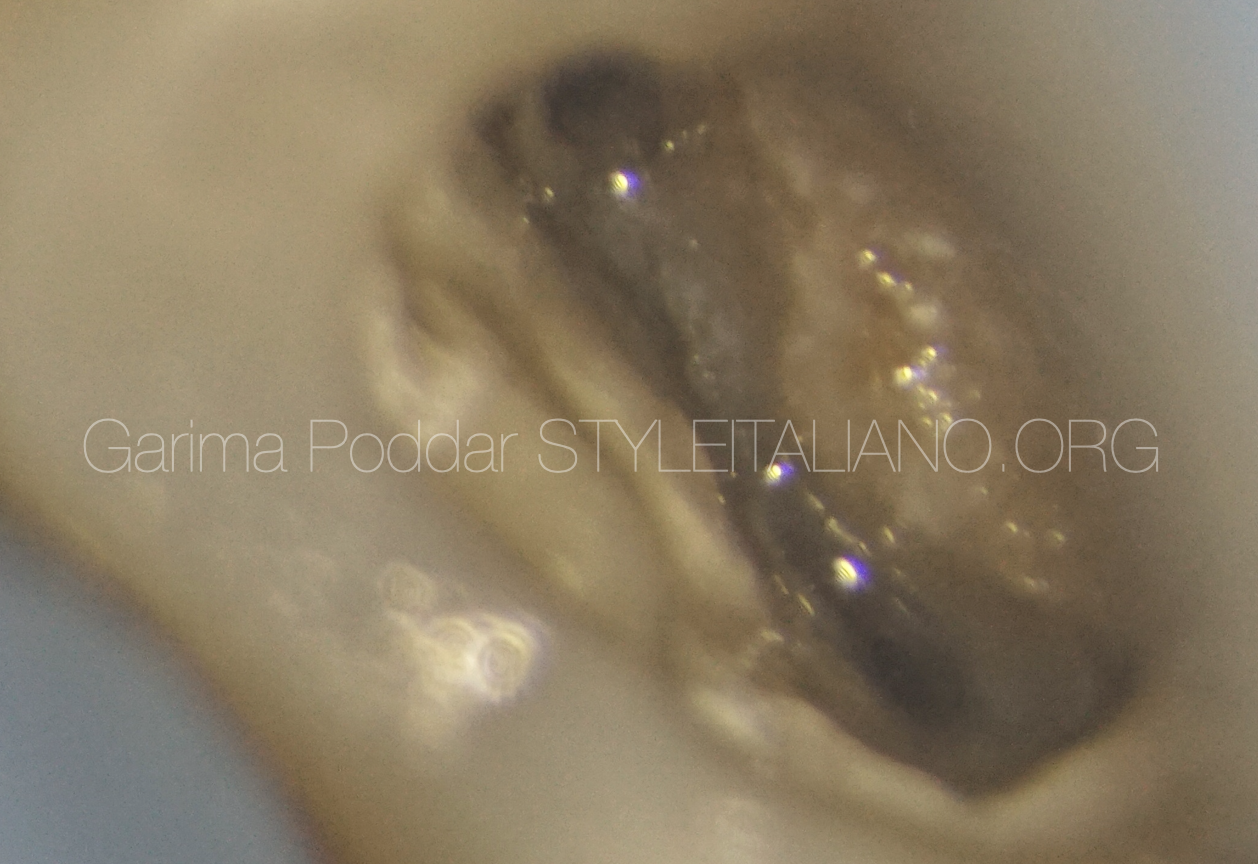
Fig. 3
Old temporary restoration was removed.
A pre endo build up was done and isthmus area was cleaned using ultrasonic tips.
Shaping of the two canals was initiated.

Fig. 4
Canals were negotiated with 10 K hand file. After coronal flaring, working length of the two canals was determined using both electronic apex locator and radiographic method.
Following this, glide path was prepared using one G file from micro mega.
The canals were shaped up till 25-06 size with TS1 and TS2 files from micro mega.
Since Buccal canal had a C shaped configuration, along with use of rotary instruments, attempt was made to scout the buccal canal using K files to clean some areas which might not have got instrumented with rotary files.
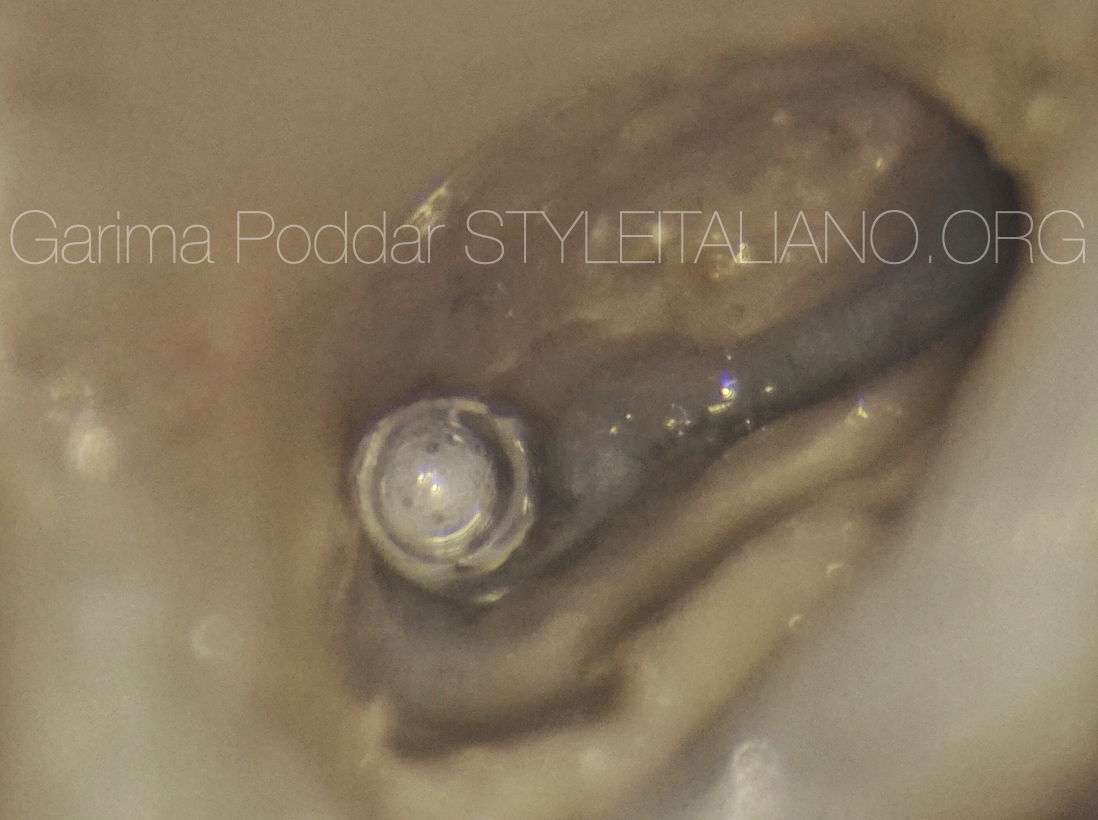
Fig. 5
Thorough irrigation and activation protocol was followed.
The irrigation protocol was as follows-
The canals were irrigated with 5.25% sodium hypochlorite during instrumentation.
After shaping was completed, fresh batch of NaOCl was introduced in the canals. Intra canal heating of the solution was performed and then the solution was activated using an ultrasonic activation device – Endo ultra . In each canal 5 such cycles were repeated with fresh introduction of NaOCl.
Then canals were flushed with distilled water, followed by which Bioakt was introduced in the canals and was activated using end ultra. And then its was rinsed off using distilled water.
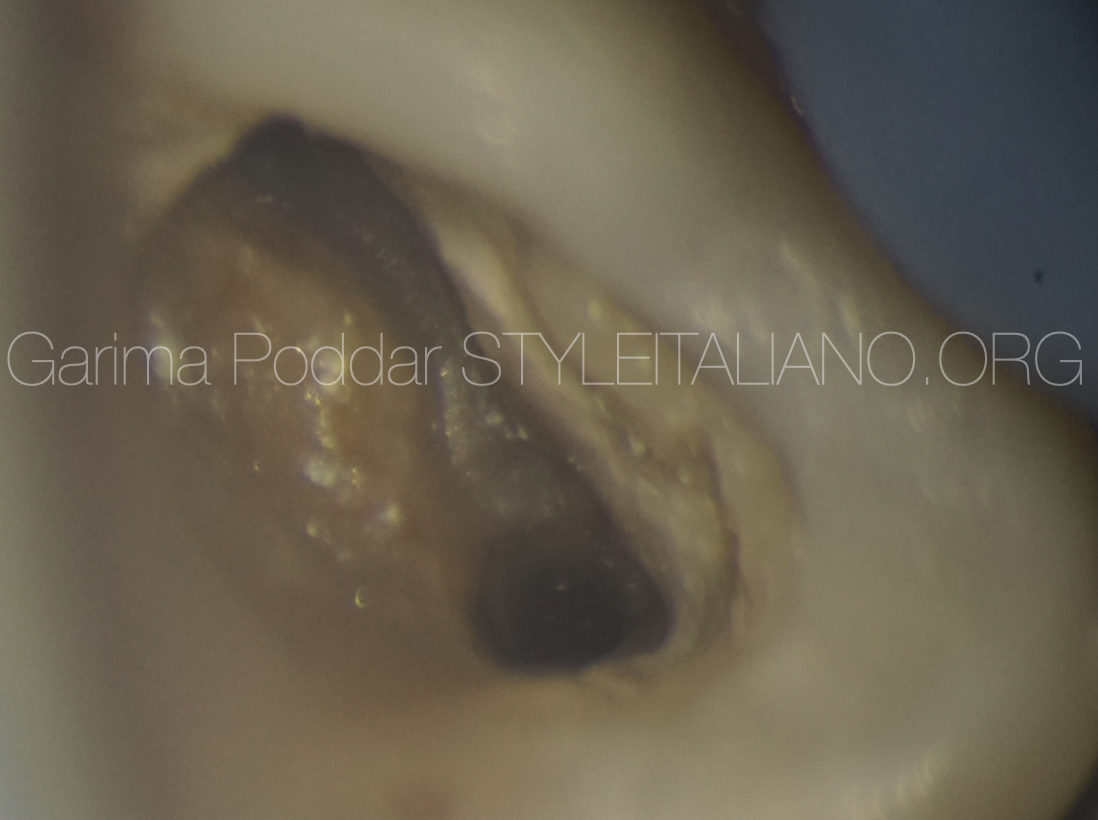
Fig. 6
The canals were dried using paper points

Fig. 7
Cone fit X –ray of the tooth was made.
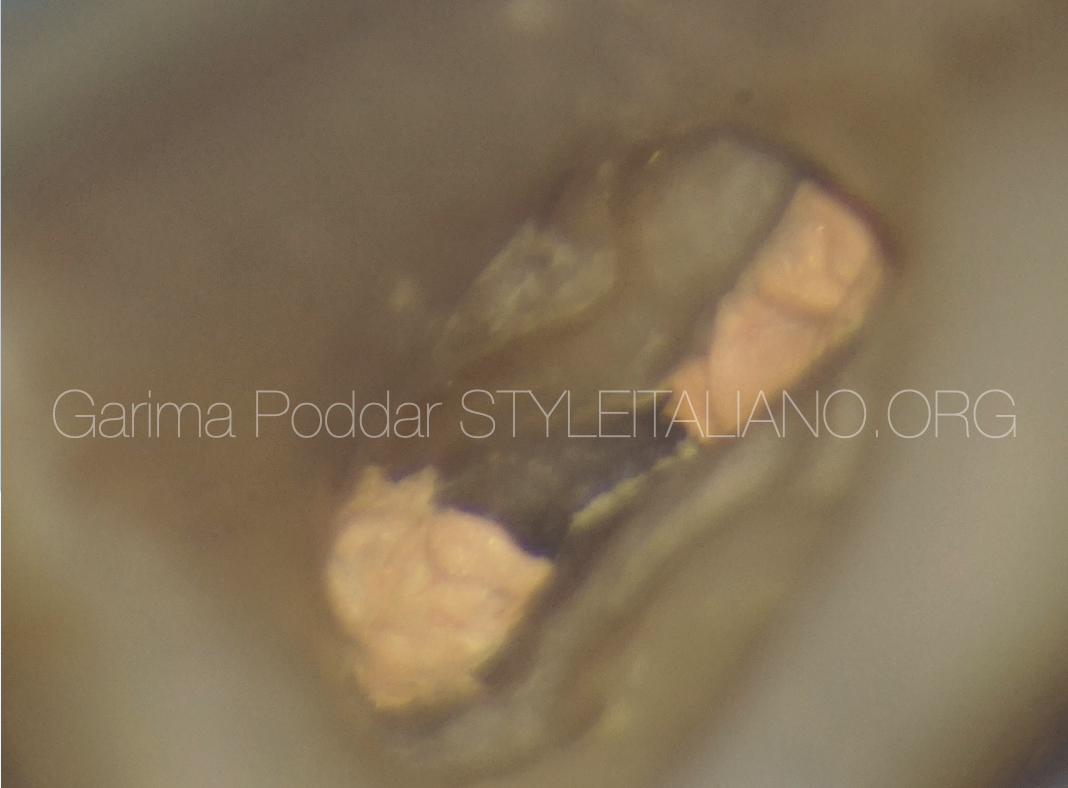
Fig. 8
The canals were obturated using warm vertical compaction technique.
The canals were coated with a resin based sealer ( AH plus from DENTSPLY maillefer).

Fig. 9
Interesting root canal system anatomy revealed after obturation.
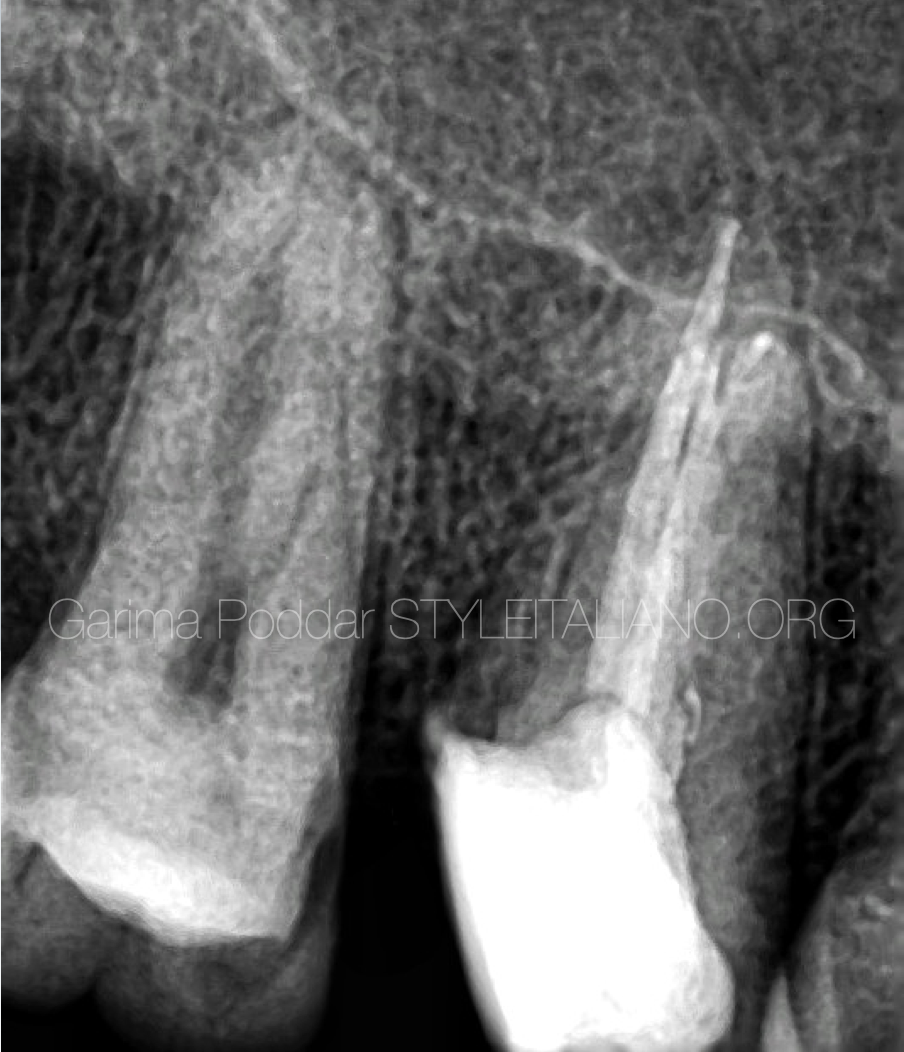
Fig. 10
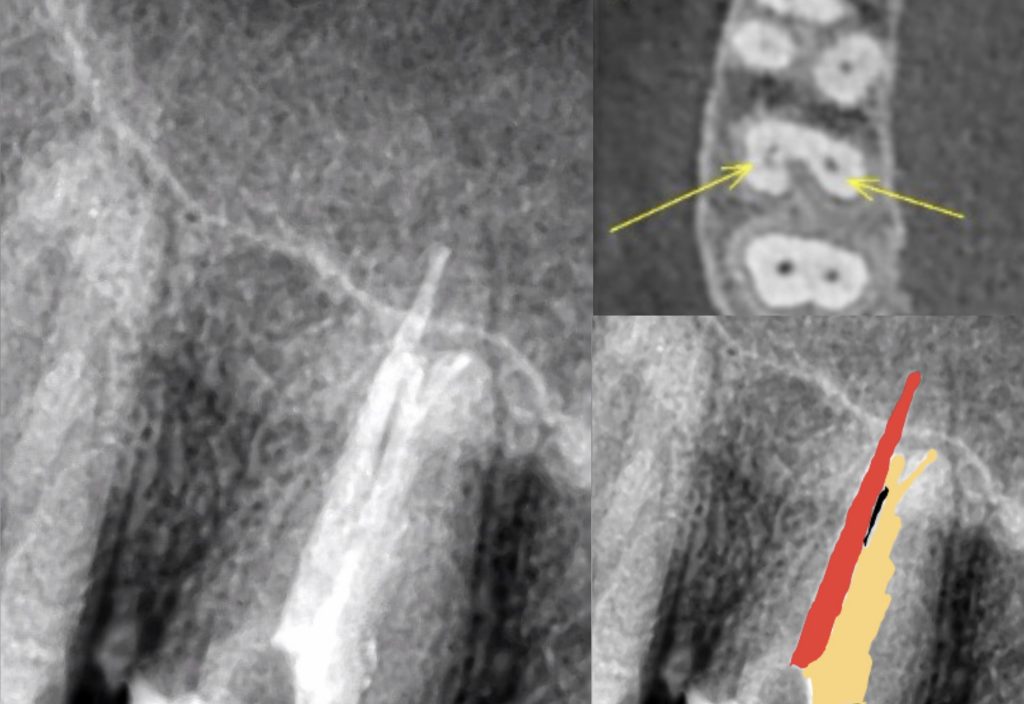
Post-op x-ray – slightly angulated view revealed an interesting root canal system for this tooth along with an apical split.

Fig. 11
Post-op angulated x-ray revealed an apical split in buccal canal which got filled up during obturation.

Fig. 12
Close up of the apical split in buccal canal.
Conclusions
Maxillary molars with C shaped configuration present with a very different anatomy. Although, they have lower prevalence rate, but a thorough understanding of variations helps in ensuring proper treatment of such teeth. The anatomy of a C shaped maxillary molar is different from a mandibular molar.
Use of magnification and following proper irrigation protocols prove to be helpful in such cases.
Bibliography
1.Jafarzadeh H, Wu YN. The C-shaped root canal configuration: a review. J Endod. 2007;33:517–23. 10.1016/j.joen.2007.01.005.
2.Lopes DS, Câmara AC, Aguiar CM, do Nascimento MD, Farias de Araújo L. A C-Shaped Canal in a Maxillary Second Molar: Prexion 3D Cone-Beam Computed Tomography Analysis. Acta Stomatol Croat. 2016;50(4):354-358. doi:10.15644/asc50/4/9 .
3. Martins, Jorge N.R. et al. Prevalence and Characteristics of the Maxillary C-shaped Molar. J Endod, 2016; 42(3):383–9.


