Efficient cleaning and proper sealing of root canals, the key to endodontic success- a case of non-surgical endodontic management of tooth number 21 and 22.
08/09/2021
Garima Poddar
Warning: Undefined variable $post in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
The target of an endodontic treatment, is to prevent and intercept pulpal / periradicular pathosis, to conserve a tooth affected by pathosis and to prevent recontamination after the treatment. After careful examination and diagnosis, a treatment plan should be made for the patient which would be predictable.
Case Report-
Patient information –
Age- 31
Gender- Male
Medical history- Non contributory.
Tooth identification- Maxillary left central and lateral incisors ( tooth number 21, 22).
Chief complaint-
Patient complained of swelling and pain in maxillary left anterior region since 15 days.

Fig. 1
Intraoral examination-
On clinical examination, the following observations were made-
- An intraoral swelling in between 21 and 22 was seen closer to tooth number 22, which had a draining tract present. The tooth was tender on percussion.
- Tooth number 21 was discolored and patient gave history of trauma during childhood.

Fig. 2
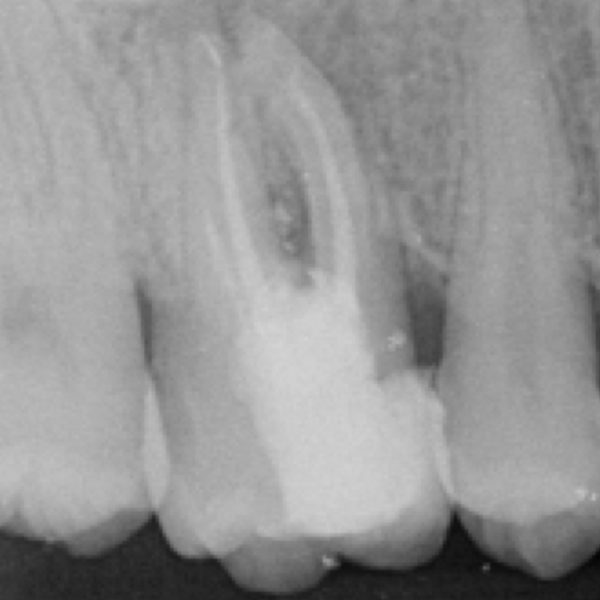
Radiographic examination-
On pre-operative radiographs, the following details were observed-
- Peri apical radiolucency in relation with tooth number 21.
- Irregular margins of root apex of 21 with widened apex.
- Peri apical radiolucency extending up till the middle third region of root length of tooth number 22.
Diagnosis-
Pulpal necrosis with chronic suppurative periradicular periodontitis in 21.
Symptomatic periapical periodontitis (dental abscess) in 22.

Fig. 3
Peri apical radiolucency extending up to the middle third region of root length of tooth number 22.

Fig. 4
Sinus was traced using a blunt gutta percha cone, after administration of local anesthesia.
On radiograph, it was confirmed that the intraoral swelling was associated with tooth number 22.
Preliminary procedures:
- Local anesthesia- Infiltration in 21 and 22 tooth region was done using 2% lignocaine with adrenaline injection.
2. Rubber dam isolation- Segment isolation from tooth number 23 to 11 was done using rubber dam, clamp on 23 and wedget inter proximally between 11 and 12.
3. Magnification- The root canal treatment was done under a dental operating microscope for better visualization.
4. Access preparation was done for 21 and 22.
5. Pus and other exudates oozed out of the central incisor.

Fig. 5
Working length was determined.
File number 60 was going beyond the apex in tooth number 21.

Fig. 6
Tooth number 22 was shaped using K files number 10 and 15, one flare files and one Reci files ( Coltene-Micromega, France).

Fig. 7
Proper cleaning and shaping was done for tooth number 21 also. The shaping was done using K files for this tooth. Thorough irrigation was performed using 5.25% sodium hypochlorite solution during shaping, after withdrawal of each file from the canal.

Fig. 8
A water based calcium hydroxide dressing was placed in the canals of tooth number 21 and 22 for 1 week.

Fig. 9
After one week, on next appointment, it was observed that the intraoral swelling had subsided.
The dressing was removed and thorough irrigation was done using 5.25% sodium hypochlorite which was activated ultrasonically. Then canals were flushed with distilled water which was followed by irrigation using 17% EDTA.
Once canals were properly irrigated, the obturation procedure was started. An apical plug with MTA was decided to be placed in 21.
The MTA carrier was selected and fit of carrier and vertical pluggers were checked in the canals. An MTA plug was placed using Map one delivery system and MTA (from Produits Dentaires SA).

Fig. 10
A dense MTA plug was placed in tooth number 21 in the apical third which was confirmed with a radiograph.
A moist cotton pellet was placed over the MTA plug and canal orifice was closed using temporary restorative material.

Fig. 11
Next appointment was done after 72 hours, and it was observed that the MTA plug had set properly in the canal. Back fill with thermo plasticized gutta percha was done in 21.
Tooth number 22 was obturated using bioceramic sealer ( Ceraseal – Meta biomed) and GP cone which was vertically compacted.
Both, central as well as lateral incisors were asymptomatic and the swelling had also subsided.
The patient was referred back to referring dentist for prosthetic phase.
Further follow up check ups have been planned for the patient periodically.
Conclusions
Proper cleaning and shaping followed by achieving a good apical seal is important while treating a tooth endodontically. MTA is a good material for creating an apical plug in cases of wide apex. Good irrigation and activation plays a vital role in such cases being treated non surgically. Use of magnification and precise tools also plays an important role in making the treatment precise and more predictable.
Bibliography
1. Güneş B, Aydinbelge HA. Mineral trioxide aggregate apical plug method for the treatment of nonvital immature permanent maxillary incisors: Three case reports. J Conserv Dent. 2012;15(1):73-76. doi:10.4103/0972-0707.92611
2. Giuliani V, Baccetti T, Pace R, Pagavino G. The use of MTA in teeth with necrotic pulps and open apices. Dent Traumatol. 2002 Aug;18(4):217-21. doi: 10.1034/j.1600-9657.2002.02107.x. PMID: 12442832.
3. Sheehan DJ, Potter BJ, Davis LS, Cutaneous Draining Sinus Tract of Odontogenic Origin: Unusual Presentation of a Challenge Diagnosis South Med J 2005 98(2):250-2.
4. Fernandes M, de Ataide I. Nonsurgical management of periapical lesions. J Conserv Dent. 2010;13(4):240-245. doi:10.4103/0972-0707.73384