A Multi-Disciplinary Approach in Non-Surgical Re-treatment of Mandibular Right First Molar
28/06/2021
Ahmed Alwaidh
Warning: Undefined variable $post in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Endodontic re-treatment is a usual scenario in daily practice. Though, it can be challenging due to many related factors. Therefore, it requires good assessment of the case through systematic approaches in terms of diagnosis, treatment plan, and the execution of the procedure.
A 40 years old male patient presented complaining of discomfort and food impaction during eating in his lower right posterior area. Upon clinical examination, LR6 had defective composite restoration leading to food stagnation between LR6 and LR7. LR6 was negative to cold test, unlike LR5 and LR7. While LR6 had mild tenderness to percussion compared to LR5 and LR7.

Fig. 1
A pre-operative clinical situation; showing defective composite restoration.
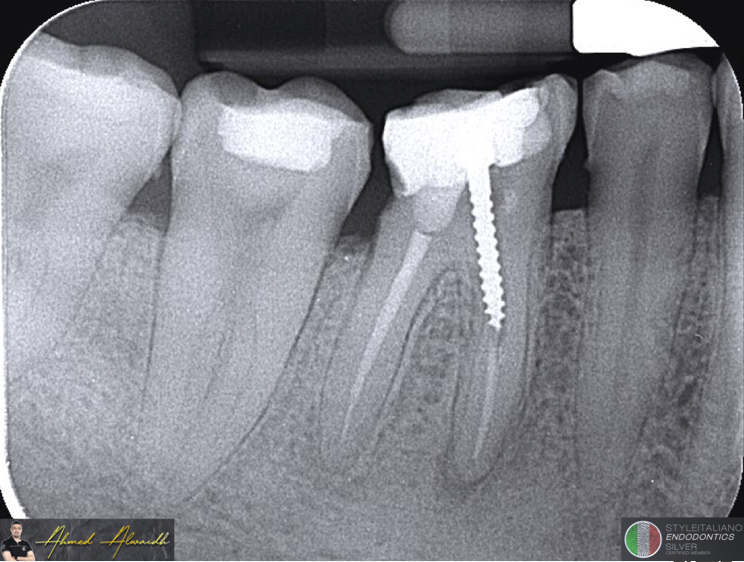
Fig. 2
A pre-operative IOPA showing an existing root canal treatment with a large screw post in the mesial root of LR6. There was also a peri-apical radiolucency around the mesial root, suggesting an ongoing peri-apical disease. Patient reported that he did the treatment around three years ago.
Diagnosis: Previously treated LR6 with symptomatic apical periodontitis (SAP).
After removal of the existing composite restoration, screw post been removed with ultrasonic tip.

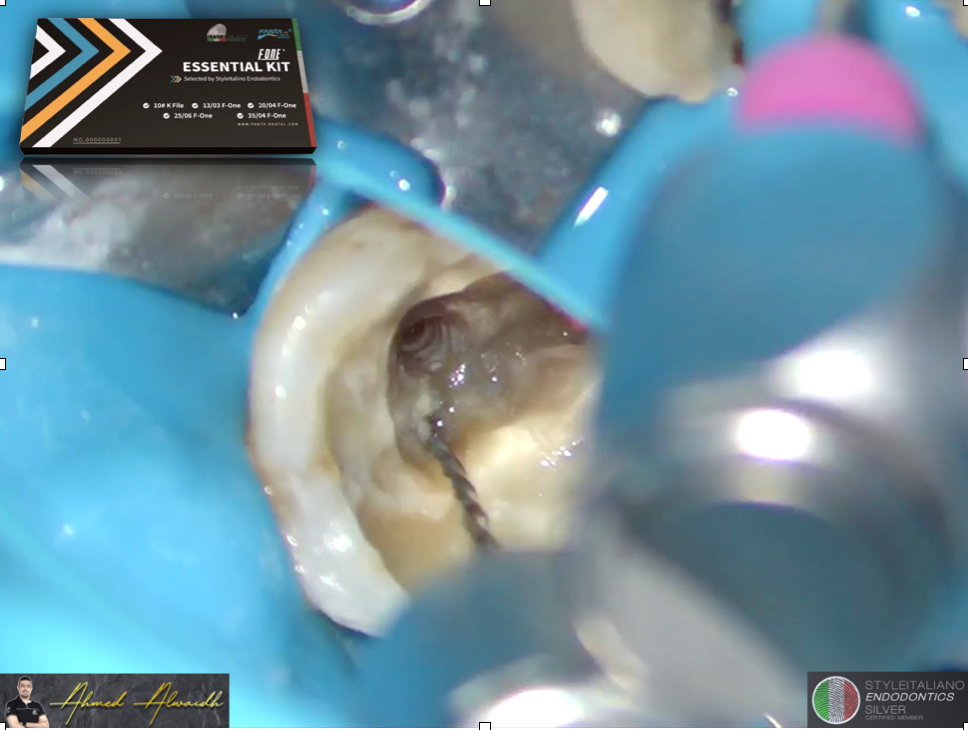
Fig. 3
After removal of screw post, it was evident that MB canal was missed.
MB canal firstly been negotiated with F One GliderST file #13/03, then prepared with F One #25/06 (Fanta Dental, Shanghai, China).
ML canal been retreated with F One #25/06 up to working length, by the use of integrated apex locator in the endomotor.
Distal canal also been retreated with F One #25/06 up to working length, by the use of integrated apex locator in the endomotor.
The remaining old root filling material been removed with the use of ultrasonic tip accompanied with copious irrigation.
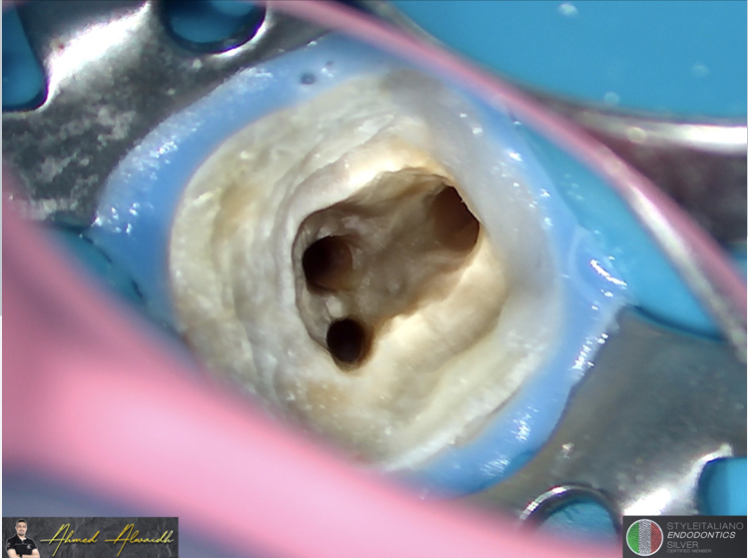
Fig. 4
All of the three canals of LR6 been prepared and disinfected with NaOCl 5.25%, EDTA 17%, and activated with passive ultrasonic, and ready for obturation.

Fig. 5
All of the three canals of LR6 been obturated with hydraulic bioceramic cement.
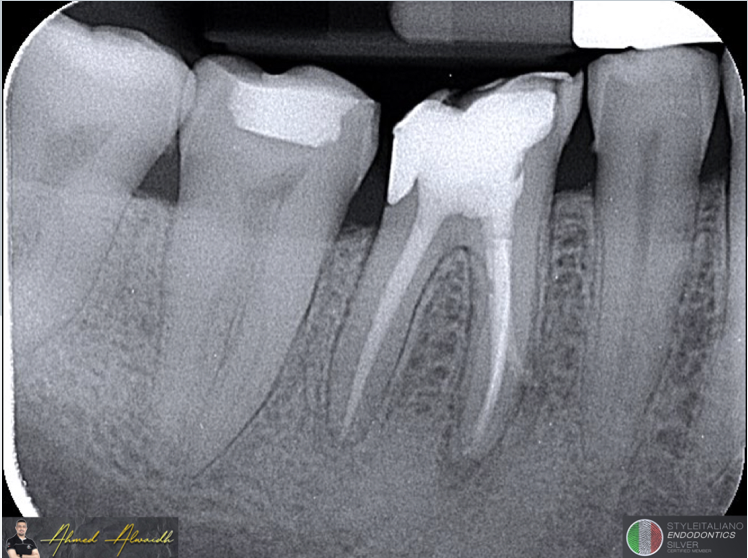
Fig. 6
Immediate post-operative IOPA of LR6; showing extent of the bioceramic cement at the site of end point of previous screw, indication a possible perforation which was not evident intra-operatively.

Fig. 7
6 months recall IOPA of LR6 with disappearance of almost all radiolucencies. LR6 was functional and symptom-free.
Conclusions
Root canal treatment does not end when the canals are filled, rather it is a systematic approach that comprises of brief data collection, formulation of diagnosis, making a proper treatment plan after discussing treatment options, and most importantly, observation of treatment outcome to justify the success of the procedure.
The SIE kit selection of F One files is a great set that gives the advantage to suit almost all situations of primary and secondary root canal treatments; due to the carefully selected sizes and tapers by many experts. On the other hand, the unique feature of the flat side design of the F One file gives it the superiority in managing difficult situations like very narrow and calcified canals in primary treatment, and efficient removal of existing root filling materials in secondary treatment, with minimum prone of file separation.
For more info about the advantages and uses of the flat side design of the F One file, you may watch the free webinar on Style Italiano Endodontics profile on Instagram through the link:
https://www.instagram.com/tv/CIsfxGdoMvG/?utm_medium=copy_link
Bibliography
European Society of Endodontology (2006) Quality guidelines for endodontic treatment: consensus report of the European Society of Endodontology. International Endodontic Journal, 39(12),921-930.
Reit C. On decision making in endodontics (1986) A study of diagnosis and management of periapical lesions in endodontically treated teeth. Swed Dent J. 41, 1–30.
Seltzer S, Bender IB, Zionitz M (1963) The interrelationship of pulp a periodontal disease. Oral Surg Oral Med Oral Pathol. 16, 1474–1490.
Sjögren U, Hagglund B, Sundqvis G, Wing K (1990) Factors affecting the long-term results of endodontic treatment. J Endod. 16: 498–504.
Strindberg LZ (1956) The dependence of the results of pulp therapy on certain factors. An analytic study based on radiographic and clinical follow-up examinations. Acta Odont Scand. 14, 1177–1180.