
Trace every tract!
23/03/2024
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Patient-reported symptoms following endodontic therapy are very subjective and variable. Clinicians often judge success by assessing the status of the periapical tissues surrounding the tooth in question, using periapical radiographs to detect the presence (or absence) of radiolucencies in this region. (Huumonen et al, 2017)
Chronic apical periodontitis (CAP) involves a host inflammatory response that develops over time, resulting in structural bone changes (bone resorption) and granulation tissue formation, which are characteristic of chronic inflammation. The quality of the endodontic treatment affects the extent of the lesion. While it is agreed that the technical quality of root obturation has a significant impact on the presence or absence of CAP, endodontic success can be achieved only if canal disinfection and coronal sealing have also been adequately performed (Estrela et al, 2014)
Intraoral sinus tract is one of the manifestations of chronic apical infections, which provides a path for drainage of pus, and infection.
Sinus tracking can assist clinician to identify the source of inflammation and differentiate between diseases of endodontic and periodontal origin. This technique is done by inserting a semi-rigid radiopaque material into the sinus track until resistance is met which commonly used materials include gutta percha cones. A radiograph will then be taken that reveals the course of the sinus tract and leads to source of infection. (Torabinejad et al, 1996)

Fig. 1
A 38-year-old gentleman was referred to my office. He was not in any discomfort. He said he had attended therapy for root canal treatment on the upper anterior central and lateral incisors 8 months ago at his dentist’s office.
His chief complaint was; “ I don’t feel that this tooth ( pin pointing to tooth 22) feels normal and sometimes I have a sore taste in the mouth”.
I took a periapical radiograph for the upper anterior teeth, that demonstrated a diffuse radiolucency at the apex of the lateral incisor.

Fig. 2
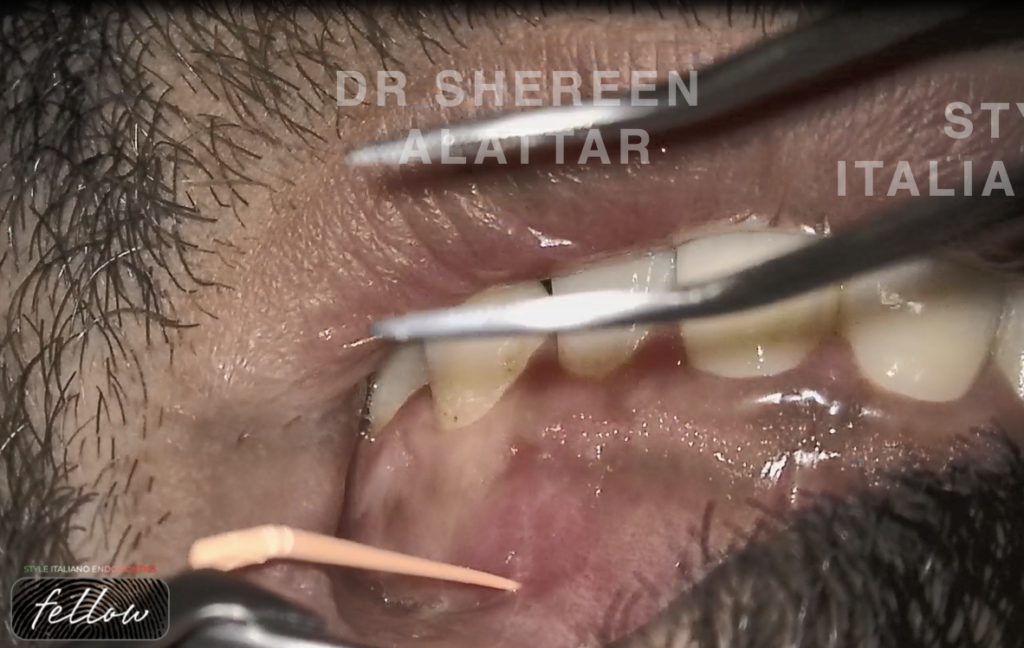
Clinical examination revealed a sinus tract labially to the lateral incisor and swelling at this level. There was tenderness to palpation and percussion.
With a size 25 gutta perch cone, sinus tract tracing was performed.
Sinus tracing can be done by inserting a gutta percha point into the sinus till resistance is felt and then exposing an intraoral periapical radiograph (Chapple et Al, 1999)
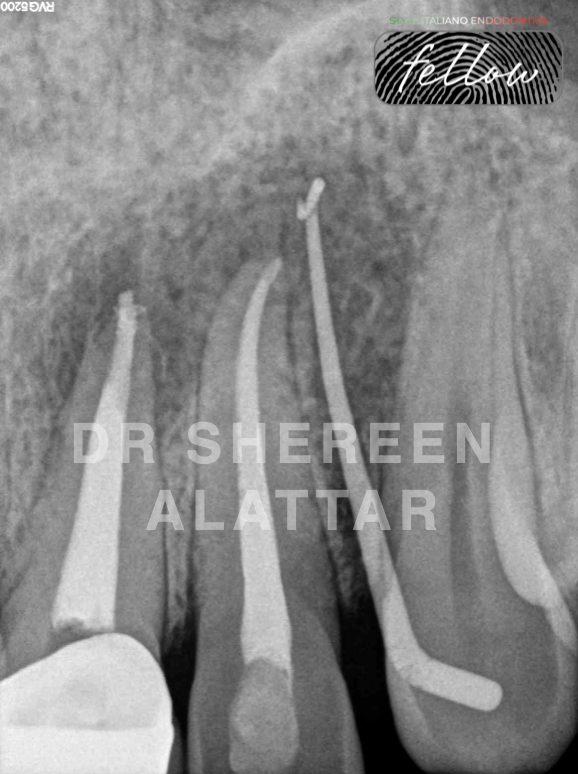
Fig. 3
The gutta percha tracing radiograph located the origin of the infection; the upper left lateral incisor.
The pulp diagnosis was previous endodontic treatment, and the periapical diagnosis was chronic apical periodontitis with sinus.
In this case, I walked the patient through everything I just described, including explaining how I used sinus tract tracing to link the infection to tooth #22. Now, we need to get retreat this tooth that he treated 8 months ago! To help him accept the treatment, I focused on the implications for his chief concern: the sore taste he has. I explained that if I left the tooth as is, as his original dentist had recommended, the sinus tract would remain right where it was, and the bump on his gums wouldn’t go away. This did the trick. He quickly changed his mind and agreed to do the retreatment.

Fig. 4
Following isolation with a rubber dam, access cavity preparation was done on tooth #22. One root canal was detected.
After the previous gutta percha was removed with Ultrasonics and rotary instruments, working length was measured using electronic apex locator.
Cleaning and shaping were performed using rotary instruments along with 5.25% sodium hypochlorite as the working solution. The canal was enlarged to size 40/0.04.
Sonic activation of the sodium hypochlorite was performed for one minute in the canal then a final rinse with 17% EDTA to remove smear layer.
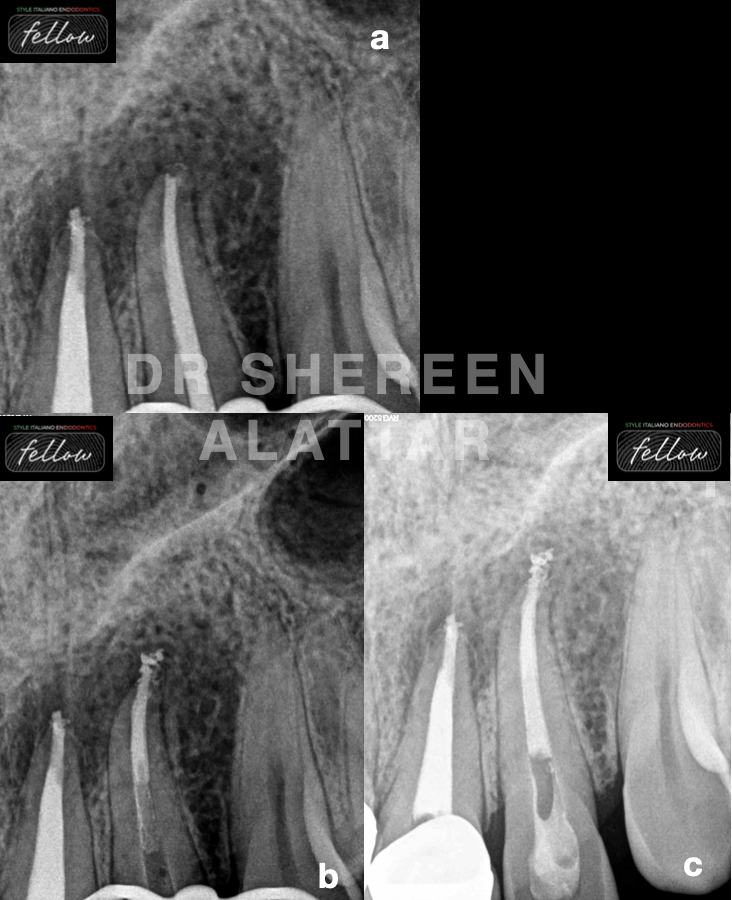
Fig. 5
Fine medium gutta percha cone was customised using the perforated ruler and a master Cone fit radiograph was taken (Fig. 5 a)
Obturation was performed using warm vertical compaction technique where System B was used with the Buchanan fine plugger and the temperature was set at 200°C. (Fig. b, c)

Fig. 6
At the 1-month recall, clinical findings showed adequate healing of the sinus region and the patient was asymptomatic.
The patient is on 3 months interval recall schedule.

Fig. 7
Dr Shereen Alattar (DDS, MSc) has graduated from Saint Joseph University in Beirut, Lebanon, where she received her Master’s Degrees in the specialisation of Endodontics. She works in a referral-based practice limited to endodontics in Amman, Jordan.
She is a fellow member in Style Italiano Endodontic Group and an active member in the Jordanian Scientific Committee of the Jordanian Dental Association and in the Jordanian endodontic society
Conclusions
Sinus tract tracing is an inexpensive and easily teachable diagnostic tool that deserves a place in any practice. It proves you don’t need to spend thousands of dollars on a CBCT machine or other advanced technology to land an accurate diagnosis. You only need to do what we must all strive to do: invest a little extra time and effort into your patient.
So, the next time you see a sinus tract, don’t make an exception, trace it! You never know when it might save the day.
Moreover, If your referred patient ends up needing a different treatment than expected, I always recommend explaining your process very clearly and relating it back to their primary concern. It’s so important for the patient to understand the long-term implications and effects of different proposed treatments, especially as they relate to the things they care about most.
Bibliography
- Torabinejad M, Trope M. Endodontic and periodontal interrelationships in Principles and Practice of Endodontics. E. Walton and M. Torabinejad, Eds., 1996.
- Chapple I, Lumley P. The periodontal-endodontic interface. Dent Update 1999;26:331-4.
- Huumonen S, Suominen AL, Vehkalahti MM. Prevalence of apical periodontitis in root filled teeth: findings from a nationwide survey in Finland. Int Endod J. 2017; 50(3): 229-36
- Estrela C, Holland R, de Araujo Estrela CR, Alencar AH, Sousa-Neto MD, Pecora JD. Characterisation of successful root canal treatment. Braz Dent J. 2014; 24(5): 3-11.



