

Touching the pulp
28/02/2026
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Vital pulp therapy (VPT) is technique that aims to preserve the living pulp tissue by treating reversible pulp inflammation caused by decay or trauma, maintaining the tooth defense system and allowing root development in newly erupted teeth and promoting healing and regeneration.
Indication: vpt indicated when:
- The pulp is healthy or shows signs of reversible pulpitis, mechanical, traumatic or small carious exposure, Hemorrhage from the pulp that can be controlled, and There are no radiographic signs of periapical pathology.
CONTRAINDECATION: when the pulp is necrotic, there is uncontrolled bleeding, signs of periapical radiographic pathology, and when the tooth is unrestorable.
Types of vpt:
- Indirect pulp capping.
- Direct pulp capping.
- Partial pulpotomy.
- Full ( coronal ) pulpotomy.
Best common materials used in vpt:
- MTA
- BIODENTIN
- BIOCERAMIC PUTTY

Fig. 1
Patient came to my clinic complaining from slight sensitivity from sweets and cold drinks in the lower right second molar. After performing cold test the tooth responded for 15 second to cold then the sense disappeared.
Radiographic x-ray shows normal periapical area with no sign of pathology.

Fig. 2
After anesthesia and rubber dam isolation I began removing all carious lesion and unsupported enamel starting from the peripheral areas away from the pulp horns step by step heading to the pulp horn area that is covered with infected dentin.
As the picture shows, the pulp exposed(pin point exposure) at the area of mesio buccal pulp horn.

Fig. 3
After disinfecting the cavity with 2,5% naocl applied with a sterile cotton, the cavity washed with normal saline and dried .
Bioceramic putty applied directly on the pulp tissue closing all the the exposure site and adapted with damp cotton piece.

Fig. 4
Then the bc putty covered with resin modified GIC. And now the tooth is ready to receive the final fiiling.

Fig. 5
Coronal sealing achieved with direct composite restoration. This case is a direct pulp capping case.
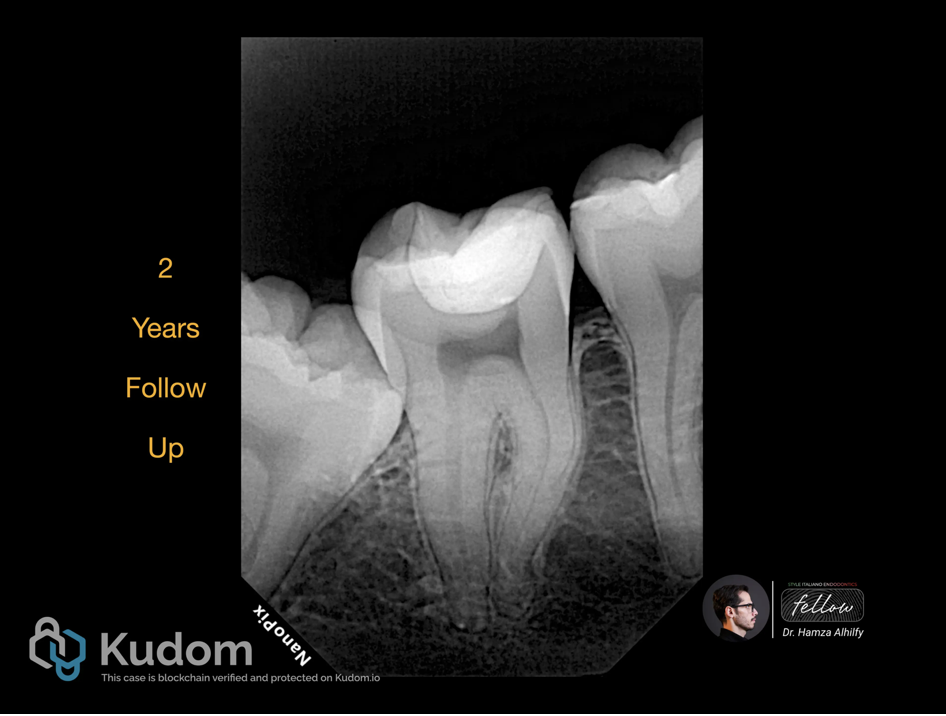
Fig. 6
Two years follow up PA x-ray shows normal periapical area with no pathology signs. And the tooth has a normal response to cold test.

Fig. 7
Here a case of partial pulpotomy. Of an upper right first premolar.
The patient came with a chief complain ( sensitivity to cold drinks and sweets ) .

Fig. 8
I removed all caries beginning with the peripheral areas away from the pulp horn region .

Fig. 9
Then I changed the bur to a new sterilized one to remove the infected pulp making a partial pulpotomy.

Fig. 10
Here I used a piece of cotton soaked with NaOCl 2.5% to disinfect the pulp tissue and also to gain hemostasis.

Fig. 11
After washing the region with normal saline , and drying it with a dry sterilized cotton, I applied bioceramic putty and made a good adaptation with suitable sized bond brush.

Fig. 12
I covered the putty with resin modified GIC. The tooth now ready for the restoration.

Fig. 13
And here is the final restoration .

Fig. 14
Pre and post operative x-ray images .

Fig. 15
The last case is full coronal pulpotomy of upper right second molar. I followed all the steps mentioned in the other cases about caries removal, etc. but in this case I removed more infected pulp tissue reaching the orifices until I gained healthy tissue and hemostasis . Then I did the same steps of disinfection and dryness.

Fig. 16
Bioceramic putty applicated then covered with resin modified GIC .
The I made a biobase and prepared the tooth for overlay.
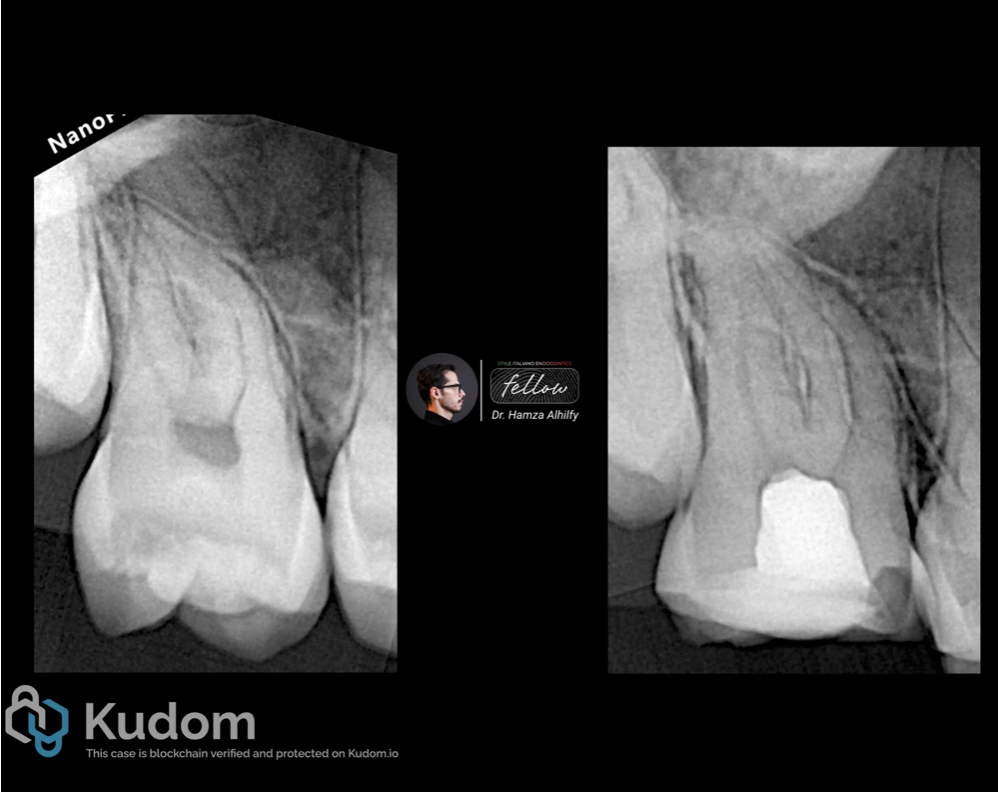
Fig. 17
X-ray images .

Fig. 18
About the author:
Dr. Hamza Alhilfy
Graduated from Al-zahrawy dental college in Iraq .
5 years experience in dentistry especially endodontic treatments .
Conclusions
Vital pulp therapy is a key component of modern minimally invasive dentistry. Advances in diagnostic methods and bioactive materials have significantly improved outcomes, making VPT a reliable alternative to RCT in appropriately selected cases. High success rates ( reaching 97% ) and preservation of natural tooth vitality make it an important option in contemporary dental practice.
Bibliography
Asgary S, Nosrat A. Vital pulp therapy: Evidence-based techniques and outcomes. Iranian Endodontic Journal. 2025;20(1):e2.
American Academy of Pediatric Dentistry (AAPD). Pulp therapy for primary and immature permanent teeth: Best practices. AAPD Clinical Affairs Council report.
Cohen S, Hargreaves KM. Pathways of the Pulp. 11th ed. St. Louis: Elsevier; 2016.
Torabinejad M, Walton RE. Endodontics: Principles and Practice. 6th ed. Elsevier; 2020.
