

The best implant is your natural tooth
01/07/2025
The Community
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Dental trauma is a significant public health concern, often resulting from accidents, sports injuries, or falls. Among the various types of dental injuries, avulsion and extrusion represent severe forms of trauma that require immediate and precise management to ensure optimal outcomes. Avulsion refers to the complete displacement of a tooth from its alveolar socket, while extrusion involves partial displacement of the tooth out of its socket, often accompanied by damage to the periodontal ligament and surrounding structures (1). Both conditions pose a risk to the vitality of the tooth and can lead to long-term complications such as root resorption, ankylosis, or tooth loss if not treated promptly and effectively (2). Early intervention, proper handling of the avulsed or extruded tooth, and adherence to evidence-based protocols are critical to preserving dental function and aesthetics (3). This case report highlights the clinical presentation, management, and outcomes of a patient with dental trauma involving avulsion and extrusion, emphasizing the importance of timely and appropriate care in such scenarios.

Fig. 1
A 17 years old male patient with alleged history of car accident and injuries sustained to the anterior maxillary region.
The patient had no relevant past medical history and was alert as well as responsive during the process of examination. Extra-oral examination revealed sever injury and swollen upper lip. On intraoral examination, The upper right maxillary central incisor (11) was missing and the marginal gingiva in the associated area was lacerated. The upper left maxillary central incisor (21) was extruded.
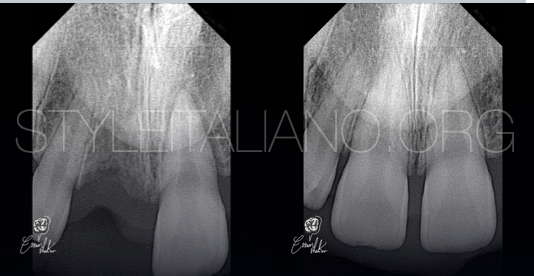
Fig. 2
After local anesthesia administration, the avulsed tooth (11) was held by the crown, taking care that the root surface was not touched, the root surface was then gently rinsed with normal saline in order to remove any debris that had adhered to it.
the alveolar socket was gently rinsed with normal saline.
Then the avulsed tooth (11) was replantation in the socket with slight digital pressure in the correct position.
The extruded tooth (21) was repositioned in the socket correctly.

Fig. 3
Flowable composite was placed at the respective spots and then the orthodontic wire was secured in place after light curing each tooth for 20 seconds.
Oral analgesics and antibiotics ( amoxicillin 500mg + clavulanic acid 125mg twice daily and metronidazole 400mg thrice daily ) was prescribed for five days.
He was advised to maintain a soft diet for two weeks along with the use of soft bristles toothbrush and 0.12% chlorhexidine mouth rinse for oral hygiene maintenance.

Fig. 4
Two weeks after replantation, the orthodontic wire and flowable composite removed, then multiple isolation was applied with rubber dam by using two small wing clamps.

Fig. 5
This photo show the pulp tissue after pulp extirpation.

Fig. 6
The access cavity was done and the pulp tissue was extirpated then arbitrary WL determination was done with apex locator and confirmed with IOPA radiography.
Since 50 size K file was freely passing through the apex, a decision for MTA plug was made.

Fig. 7
In this case the effect of the good irrigation is undeniable. As shown, was the irrigation protocol that relied on a group of irrigating materials in an orderly sequence to ensure good chemical cleaning of the root canal system, as each of this materials have a specific function.
Sodium hypochlorite 5,25% ( NaOCl ): the main irrigating solution used to dissolve organic matter and kill microbes effectively (4)
Ethylenediaminetetraacetic acid (EDTA): is needed as a final rinse to remove the smear layer.(12-15) But it has been used in this protocol more than once to ensure that the dentinal tubules are open to grantee that NaOCl well reach every point of root canal system.
saline: used between these two irrigants to avoid the chemical interaction between them(5)
It was necessary to guarantee the safety and not to pass any of these materials beyond the root apex, also a Gauge 30, double side vented irrigating needle was used to deliver the irrigating material to each canal in depth shorter than the working length by 3 mm.(6)
The activation of irrigant was done by using an ultrasonic activator, the duration of each activation last for 20 sec.(7)
The image shows the tooth after complete the irrigation protocol

Fig. 8
Incremental placement of White MTA was done at apex with pluggers and butt end of paper points, to form an apical plug.
Excess MTA along the walls was removed using moist paper points.
The extruded material (MTA) does not negatively affect the healing of the periapical tissues (8).

Fig. 9
In the same session after the positioning of 4-5 mm of MTA into the apical area the canal was fill with guttaperca.
And this radiography show the final result.
The patent was informed about possibility of root resorption or ankylosis.

Fig. 10
Clinical image after three months

Fig. 11
Three months recall

Fig. 12
About the author:
Dr. ISAM SHAKIR ALWAN
.Graduated with BDS from University of Alkafeel in 2021.
.My passion in Endodontics started during my training at university.
Have certificate many courses in basic, advanced Endodontics and Endodontics microsurgery.
Key Opinion Leader for MARUCHI.
My work is committed to microscopic Endodontics and aesthetic dentistry.
Conclusions
Dental trauma involving extrusion and avulsion presents significant challenges in clinical management, requiring prompt and evidence-based intervention to optimize outcomes. This case highlights the importance of timely diagnosis, appropriate emergency care, and adherence to established guidelines, such as those provided by the International Association of Dental Traumatology (IADT). Effective management strategies, including proper repositioning, splinting, and endodontic treatment, are critical to preserving tooth vitality and preventing complications such as root resorption, ankylosis, or tooth loss. Long-term follow-up is essential to monitor healing and address any sequelae. This case underscores the need for increased awareness among healthcare providers and the public regarding the management of dental trauma, as well as the value of a multidisciplinary approach in achieving favorable patient outcomes.
Bibliography
1. Andersson, L., Andreasen, J. O., Day, P., Heithersay, G., Trope, M., DiAngelis, A. J., ... & Tsukiboshi, M. (2012). International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 2. Avulsion of permanent teeth. *Dental Traumatology*, 28(2), 88-96. https://doi.org/10.1111/j.1600-9657.2012.01125.x
2. Petti, S., Glendor, U., & Andersson, L. (2018). World traumatic dental injury prevalence and incidence, a meta-analysis—One billion living people have had traumatic dental injuries. *Dental Traumatology*, 34(2), 71-86. https://doi.org/10.1111/edt.12389
3. Fouad, A. F., Abbott, P. V., Tsilingaridis, G., Cohenca, N., Lauridsen, E., Bourguignon, C., ... & Levin, L. (2020). International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 1. Fractures and luxations. *Dental Traumatology*, 36(4), 314-330. https://doi.org/10.1111/edt.12578
4. Haapasalo M, Shen Y, Wang Z, Gao Y. Irrigation in endodontics. Br Dent J. 2014 Mar;216(6):299-303. doi: 10.1038/sj.bdj.2014.204. PMID: 24651335.
5. Prado M, Santos Júnior HM, Rezende CM, Pinto AC, Faria RB, Simão RA, Gomes BP. Interactions between irrigants commonly used in endodontic practice: a chemical analysis. J Endod. 2013 Apr;39(4):505-10. doi: 10.1016/j.joen.2012.11.050. Epub 2013 Jan 30. PMID: 23522546.
6. Uzunoglu-Özyürek E, Karaaslan H, Türker SA, Özçelik B. Influence of size and insertion depth of irrigation needle on debris extrusion and sealer penetration. Restor Dent Endod. 2017 Dec 22;43(1):e2. doi: 10.5395/rde.2018.43.e2. PMID: 29487833; PMCID: PMC5816991.
7. Nagendrababu V, Jayaraman J, Suresh A, Kalyanasundaram S, Neelakantan P. Effectiveness of ultrasonically activated irrigation on root canal disinfection: a systematic review of in vitro studies. Clin Oral Investig. 2018 Mar;22(2):655-670. doi: 10.1007/s00784-018-2345-x. Epub 2018 Jan 25. PMID: 29372445.
8. Long-term observation of the mineral trioxide aggregate extrusion into the periapical lesion: a case series.2013 Apr; 5(1): 54–57. Published online 2013 Apr 5. doi: 10.1038/ijos.2013.16.