Single session endo resto treatment of an upper second molar
25/11/2024
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
A 38 years old patient with a non-contributory medical history came to my attention due to a persistent and intense pain on the upper left hemiarch.
On clinical examination, the patient presents severe toothache, sensitivity to hot and cold stimulations and pain while biting. There was a strong positive response to the cold test and a negative response to the percussion test on tooth 2.7, which had an amalgam restoration on the occlusal surface.
In agreement with the patient, it is decided to perform root canal treatment on the tooth 2.7.

Fig. 1
On radiological examination, there is no evidence of periapical lesions.
There is a radiolucent area beneath the amalgam restoration, indicating a potential infiltration or secondary decay.

Fig. 2
Pre operative picture

Fig. 3
After the anesthesia I did a multiple isolation on teeth 2.7, 2.6 and 2.5

Fig. 4
I removed the existing restoration and the decayed tissue, then I started designing the access cavit with a diamond coated bur mounted on a turbine, until the pulp chamber floor was visible. Subsequently, I refined the access with ultrasonic tips.

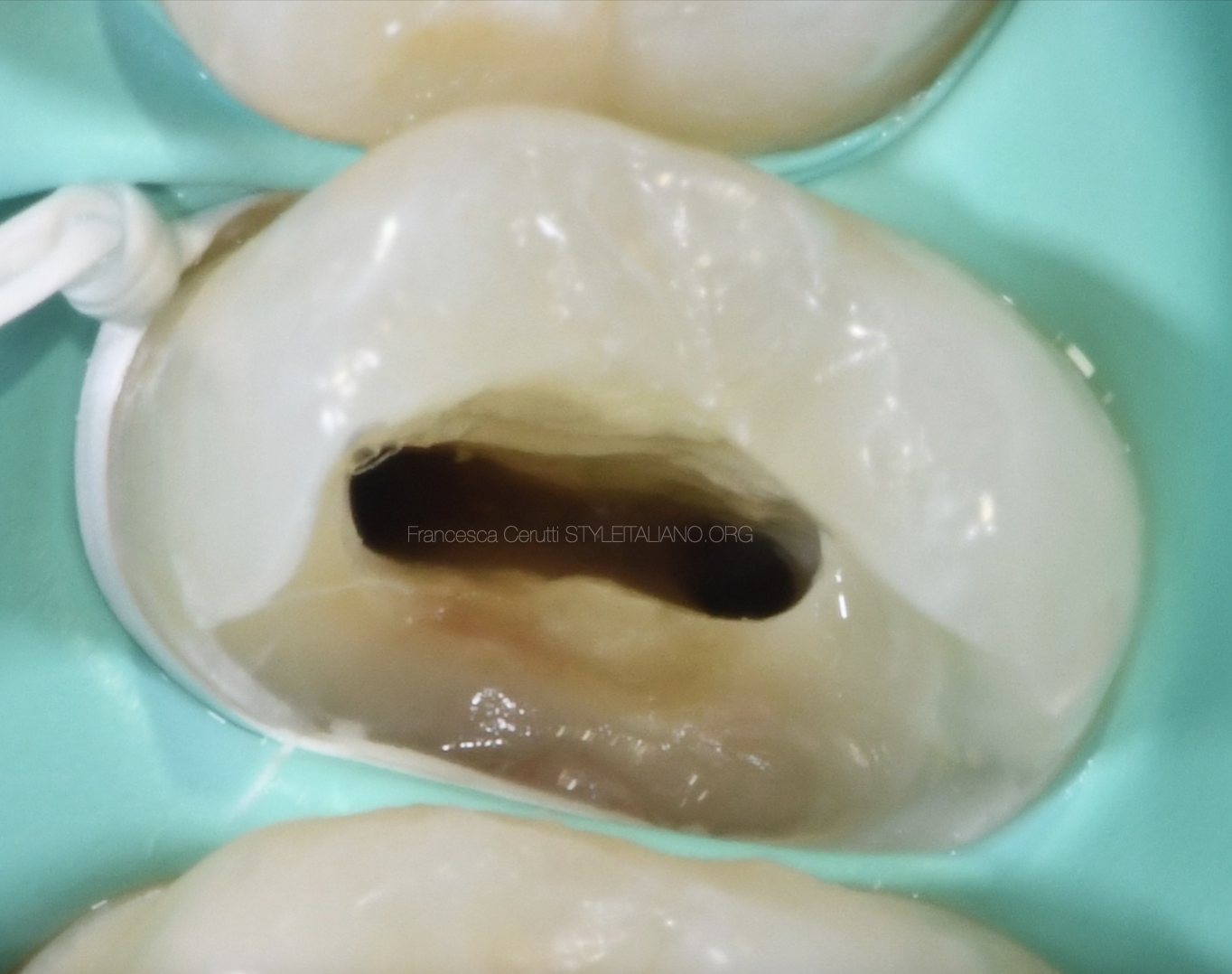
Fig. 5
From the picture in can be seen that there are 4 root canals in this tooth.
Due to the difficult scouting of MB1 with a #10 K-file, I did some coronal preflaring and refined the access cavity.
I then proceed to shape the root canals using martensitic files, following the sequence with a Crown-Down technique.
I established patency with a #.10 K-file, then I continued the shaping up to the working length.

Fig. 6
I shaped the root canal system with martensitic files and always did a visual gauging to determine the final size of the apical foramen, which was refined with dedicated rotary files..
To summarize: MB1 is prepared to size #30, MB2 to #20, DV to #25, and the palatal canal to #50.
It’s important to note that MB2 is confluent with MB1 at 16 mm.

Fig. 7
After shaping I did the final irrigation protocol using NaOCl, EDTA, and distilled water delivered by a polypropylene cannula and activating by ultrasonic tips according to the correct timing.
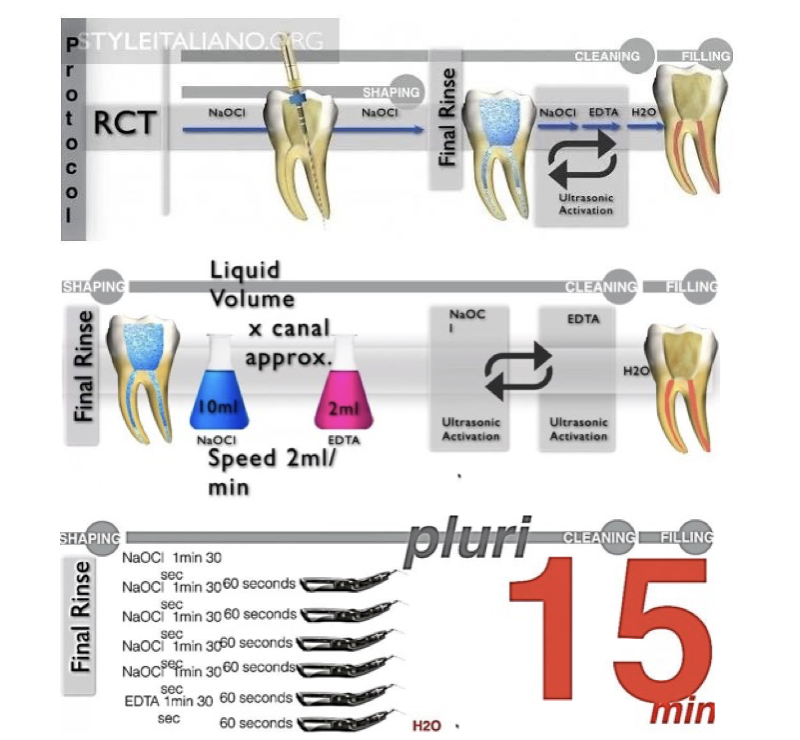
Fig. 8
The protocol I followed

Fig. 9
After that, I checked the fit of the gutta percha points

Fig. 10
Intra operative X-ray with gutta percha points. The confluence between MB1 and MB2 canal can be noted.

Fig. 11
I filled the root canal system with a hydraulic sealer and single cone technique

Fig. 12
Since the conditions were favorable, I cleaned the cavity and immediately proceeded with the post endodontic restoration that consisted in a direct composite restoration.

Fig. 13
The tooth after the restoration

Fig. 14
Post operative X-ray

Fig. 15
About the author:
Gioele Bianchetti
2013: Diploma (100/100) – Istituto tecnico Industriale “Benedetto Castelli” in Brescia
2016: Graduated (110/110) in Nursing Sciences form the UCSC of Rome
2018: Master in CardioVascular Echography Techniques
2019: Advance course in Implant of medium and long-term venous system PICC and MIDLNIE
2020 - current: Student in Dentistry in UNIBS
2023: Member of the CTS of Adakta society srl
2024: Fellow of Style Italiano Endodontics
Member of the Italian Society of EchoCardiography and CardioVascular Imaging from 2018.
Conclusions
The patient express complete satisfaction with the root canal treatment and has no post operative pain, also thanks to the fact that there was a good control of the obturation extension.
A strict protocol can help achieving good results in endo-restorative cases.
Bibliography
Fransson H, Dawson V. Tooth survival after endodontic treatment. Int Endod J. 2023 Mar;56 Suppl 2:140-153. doi: 10.1111/iej.13835. Epub 2022 Oct 2. PMID: 36149887.
Castellucci A. Endodontics: Martina; 2004.
Tonini R, Cerutti F. Disinfezione e protocolli clinici nei ritrattamenti. 1. 1 ed. Ritrattamenti. Soluzioni per patologie apicali di origine endodontica: EDRA; 2019. p. 215-44.