Retrieve and repair
08/07/2023
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
As Endodontists our daily work is an adrenaline fuel because we face new challenges on a daily basis and each case requires a strategy to fix it.
Strategy before any retreatment consists of reading very carefully the preoperative X-Ray, in order to explain to the patient what is the problem, prognosis ,number of visits, possibility of flare ups and cost as well.
In this interesting case, a dear colleague of mine referred this patient to me due to a non stop pain in this tooth.
Psychological management is the very first step to treat patients like this because it is not an easy task and she is already in a lot of pain.
In this case we find perforation of mesial root that is obturated by GP & broken file inside distal root causing the patient tremendous consistent pain.
Aroma, Music and calm voice to explain the patient about the severity of the problem while giving her confidence that we can handle such cases and also explaining the possibility of flareups and how the session will go.
As a routine, I always prefer to prepare all of my stuff before I start the case and in this case after viewing the preoperative X-Ray I prepared my ultrasonics from the start along with all the files I'm gonna need to retreat this tooth and waste no time.
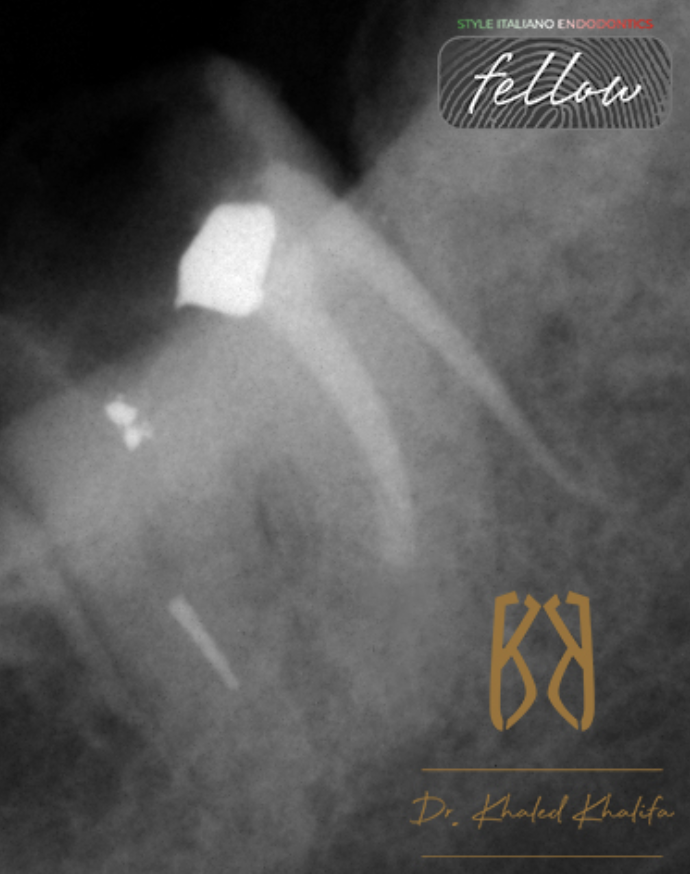
Fig. 1
Careful examination of pre-operative X-Ray to determine the degree of difficulty:
- GP perforating the mesial root of the tooth (denoting cleaning and shaping of bone and obturating it with GP).
- Short mesial filling by 3-4 mm denoting either ledge or blockage.
- Broken Rotary file at middle to apical junction of distal root.
- Metallic filling over mesial root and inside the orifice of distal root.
- Non visible canals space beyond broken file and beyond short mesial filling denoting dystrophic calcification or very tight canal space.
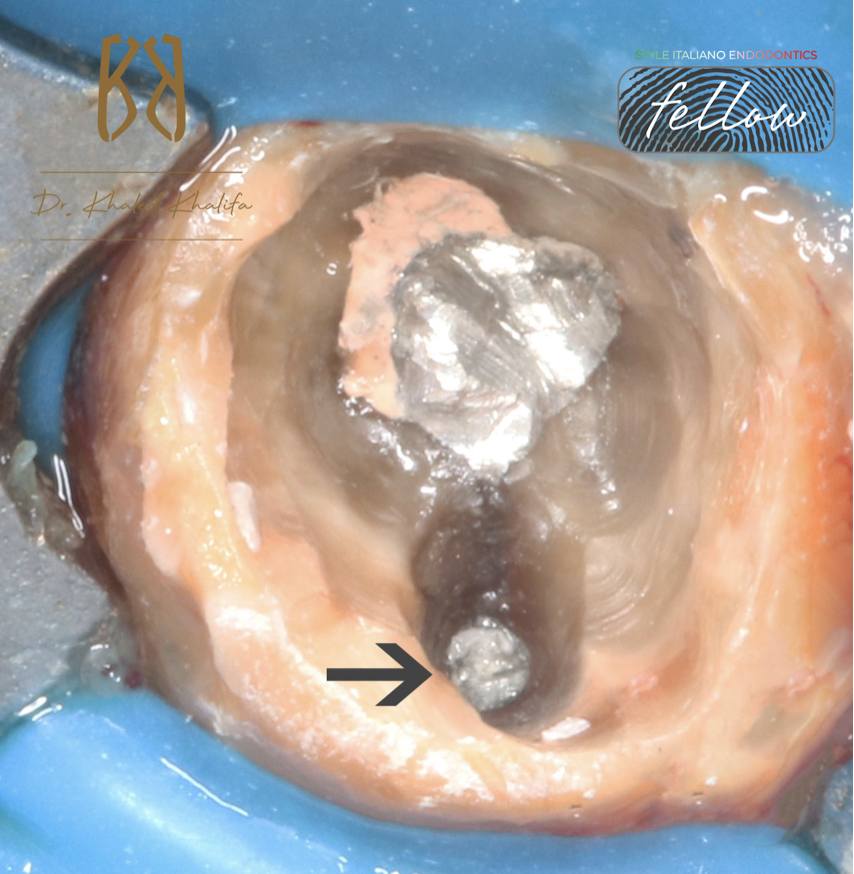
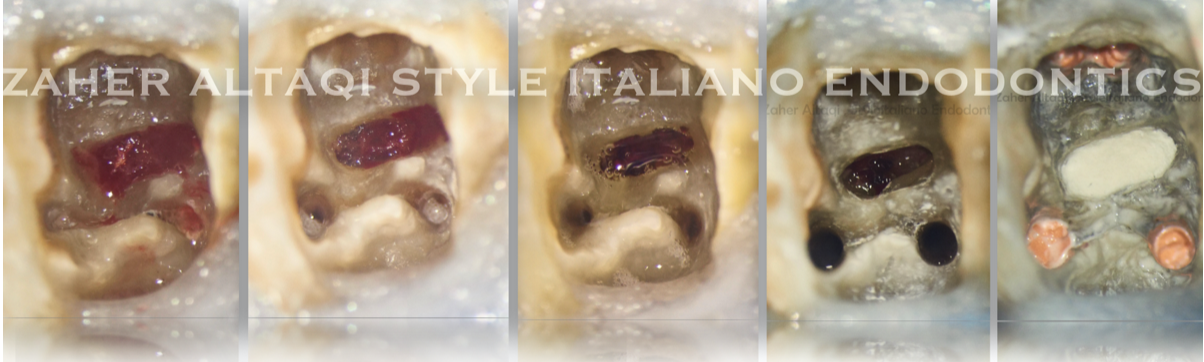
Fig. 2
Here is after removal of temporary filling, metallic filling covering mesial root and inside the orifice and canal of distal root (black arrow).
Careful inspection using ultrasonics and Endodontic probe DG16 to remove all of this and to uncover the GP inside the bone and differentiate it from the GP inside the root.
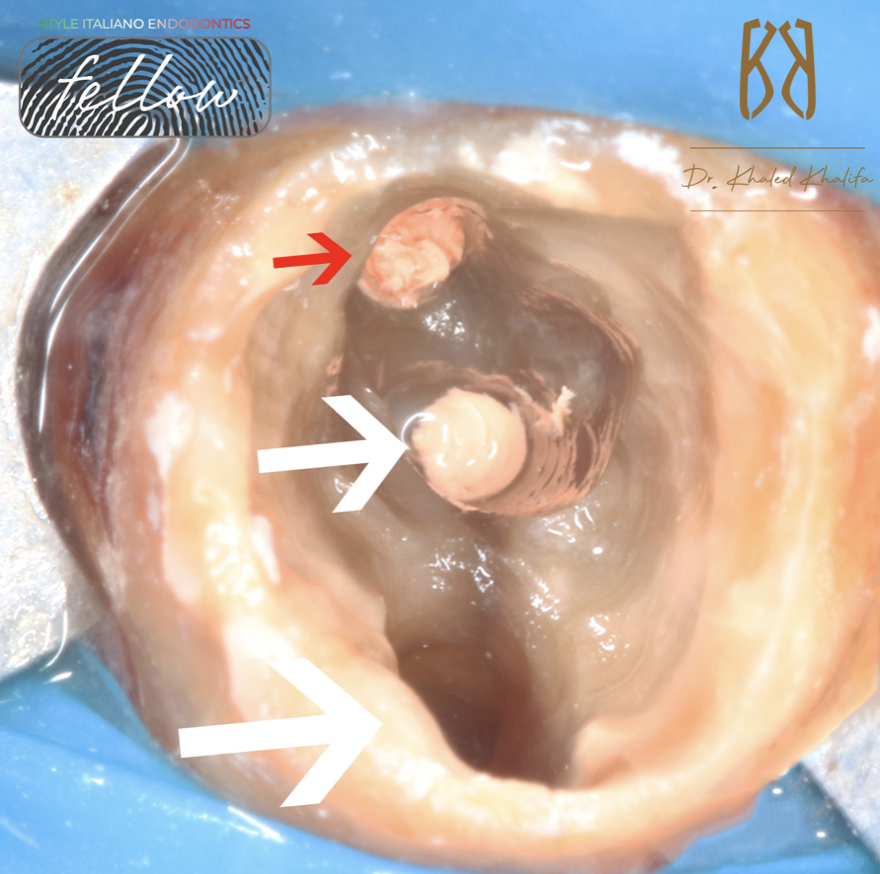
Fig. 3
Here is after careful removal of all coronal obstructions
GP inside the bone (red arrow )
GP inside the Mesial Canal (small white arrow)
Distal Root after removing all metallic filling (large white arrow)

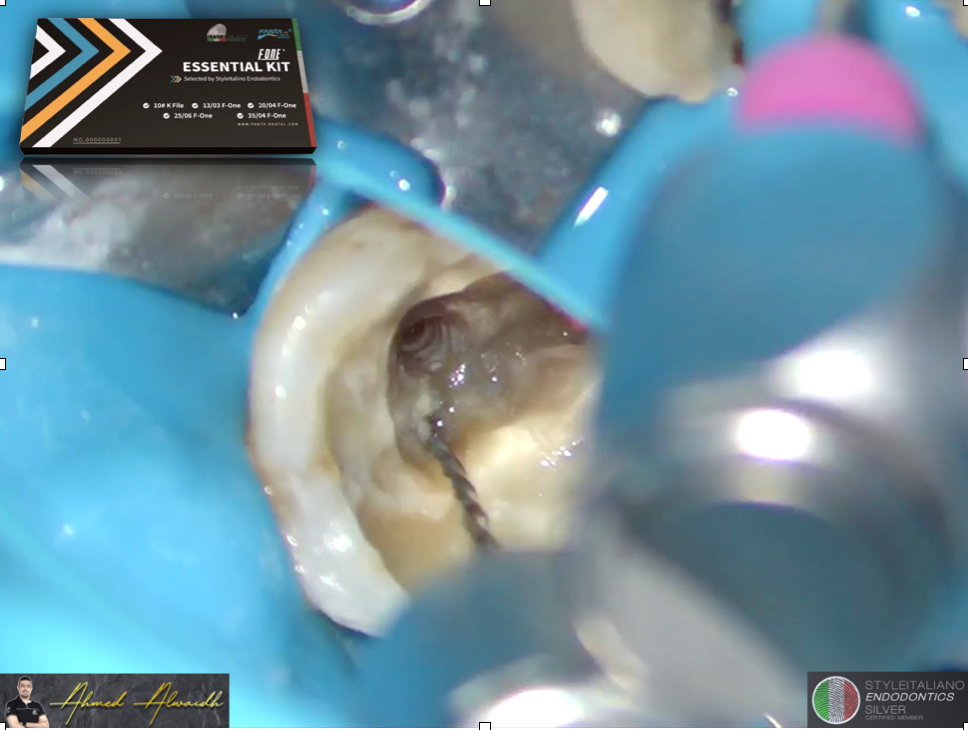
Fig. 4
Atraumatic removal of broken file from distal canal.
Enlargement above it using modified 25 Taper 6% rotary file and ET25 Ultrasonic Tip.
P.S I removed the file before removing GP from the perforation Site and from Mesial canal in order for it not the jump from distal root to any other place.
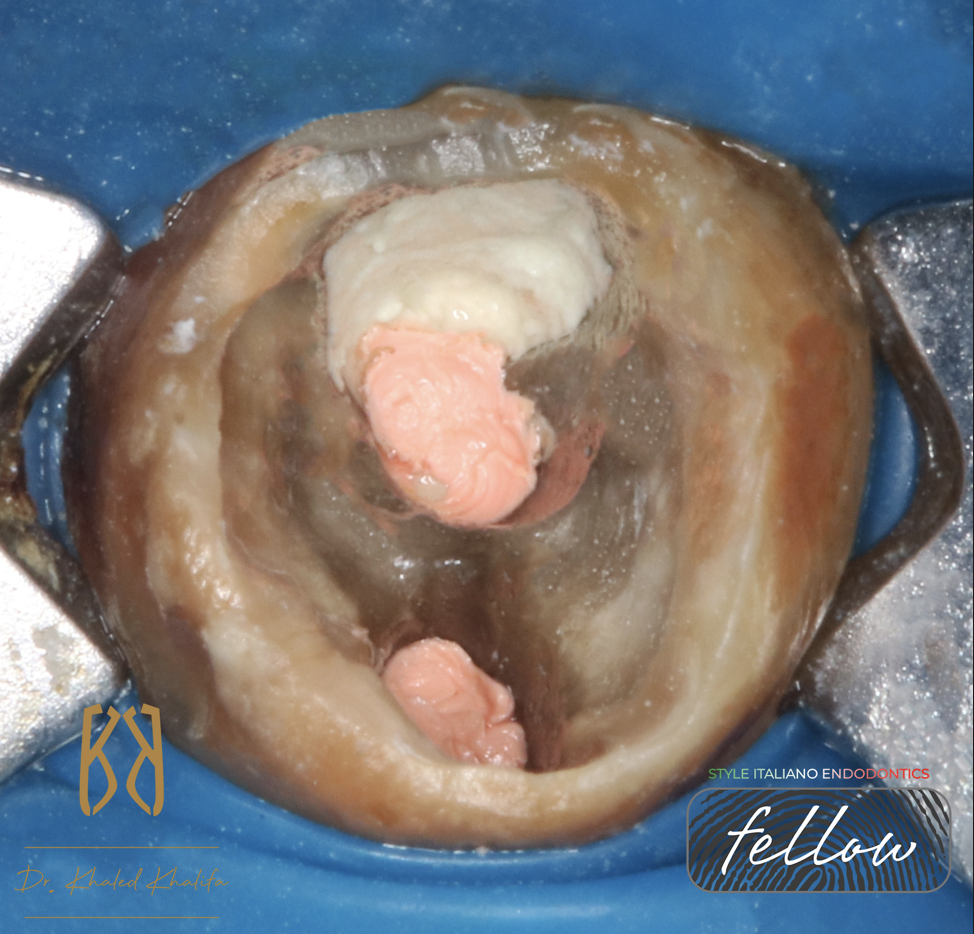
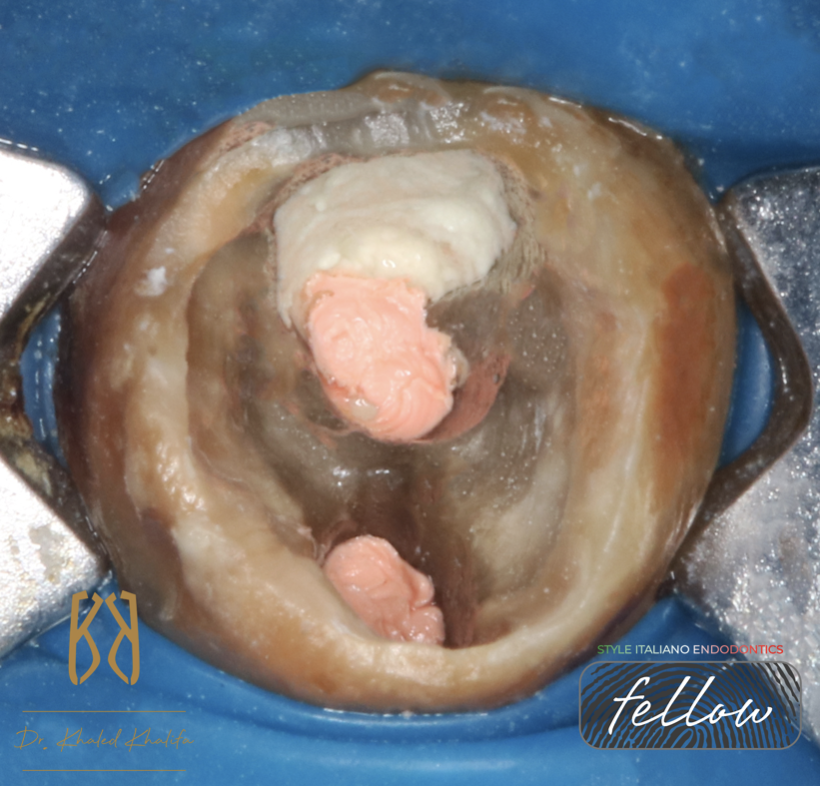
Fig. 5
After complete cleaning and shaping of mesial root and distal root, I removed GP from perforation side using H Files to grab it.
Due to severe bleeding of granulation tissues removed, I temporized the case using calcium hydroxide to neutralize the acidity of perforation site before placing MTA
Here you find the Mesial and Distal Canal obturated and Perforation site closed by MTA.

Fig. 6
Post operative X-rays show:
- Closure of perforation site with no voids and closing every discrepancy.
- GP removed from bone with no leftovers.
- No loss in dentin while removing broken file distal.
- Fixing short mesial root ledge and reaching apex.
- Coronal seal via final bonded restoration.

Fig. 7
About the Author:
Dr Khaled Khalifa
B.D.S. Misr International University
Endodontic Specialist
Course Director “The Endo Formula”
Endodontic Consultant in multiple private clinics
Member of The Royal College of Surgeons England (MJDF)
Member of The American Association Of Endodontics (AAE)
Member of British Association Of Endodontics (BES)
Practice limited to Endodontics
Conclusions
Retreatments are very challenging. Careful inspection of preoperative X-ray allows you to put a strategy on how to fix the tooth.
Operator must have enough knowledge, skills and tools before going through such treatments in order not to complicate the case more than this.
Our prime goal is to restore function and health of tooth structure with minimal loss of tissues.
Bibliography
Prognostic Factors and Primary Healing on Root Perforation Repaired with MTA: A 14-year Longitudinal Study
Fabio G. Gorni, DDS Andrei C. Ionescu, DDS, PhD
Federico Ambrogi, MSc, PhD Eugenio Brambilla, DDS Massimo M. Gagliani, MD, DDS
Published:June 14, 2022DOI:https://doi.org/10.1016/j.joen.2022.06.005
Contemporary Endodontic Retreatments: An Analysis based on Clinical Treatment Findings
Michael M. Hoen, DDS Frank E. Pink, DDS, MS
DOI:https://doi.org/10.1097/00004770-200212000-00010
Postoperative Pain after Endodontic Retreatment Using Rotary or Reciprocating Instruments: A Randomized Clinical Trial
Daniel Comparin, DDS, MSc Edson Jorge Lima Moreira, DDS, MSc, PhD Erick M. Souza, DDS, MSc, PhD Gustavo De-Deus, DDS, MSc, PhD Ana Arias, DDS, MSc, PhD Emmanuel João Nogueira Leal Silva, DDS, MSc, PhD
Published:May 03, 2017DOI:https://doi.org/10.1016/j.joen.2017.02.010
Flare-ups after Endodontic Treatment: A Meta-analysis of Literature
Igor Tsesis, DMD Vadim Faivishevsky, DMD Zvi Fuss, DMD Ofer Zukerman, DMD
Published:August 26, 2008DOI:https://doi.org/10.1016/j.joen.2008.07.016