
Retreatment of teeth with a complex root system anatomy #1
08/06/2024
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
The second maxillary premolar may have 1 to 3 roots: with one root canal in 75-96% of cases, with two root canals in 4-24% and three root canals in 0-1%.
Careful interpretation of preoperative radiographs is essential for providing insight into the number of existing root canals. In maxillary premolars with multiple roots and canals, the roots and canals may look unusual but the canals may not be evident in radiographs. Sudden narrowing or disappearance of the root canal space may indicate the presence of one or more extra canal(s). Radiographic appearance of the corresponding contralateral tooth may help in detecting additional canal(s), since bilateral teeth may present a similar morphology.
Three dimensional data obtained with cone beam computed tomography (CBCT) is extremely useful in identifying the multiple‐canal variants Given the relatively high percentages of two canals in these teeth, radiographic imaging with varied horizontal angulation is recommended to determine the presence or absence of a second or third canals (Mahajan et al. 2016). Of course, if CBCT imaging was available, it would be the most definitive means of determining the root canal anatomy. Once the access preparation is properly oriented and extended, the case becomes more predictably treatable.
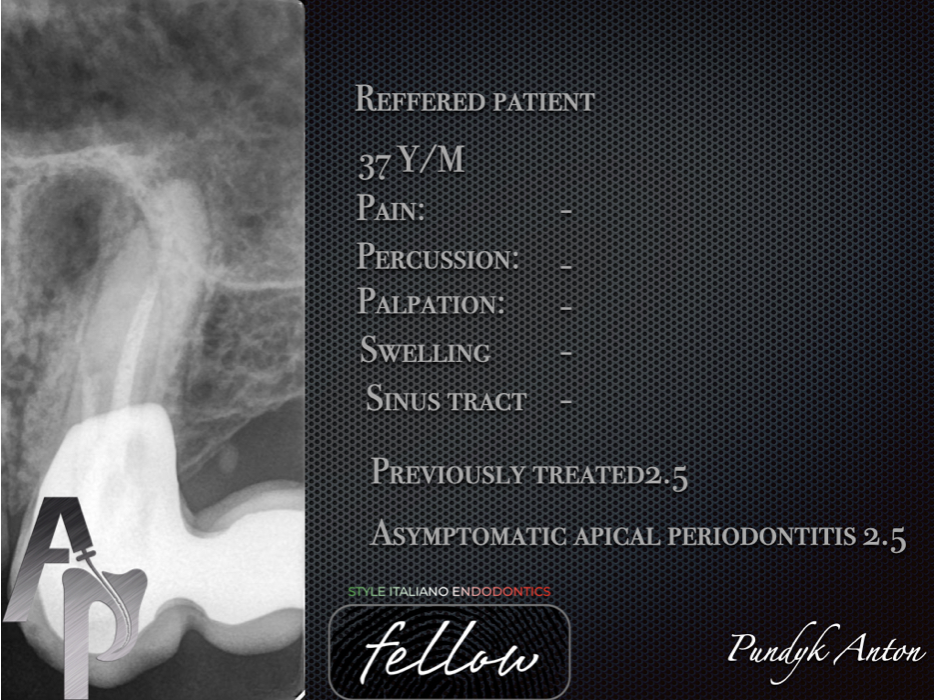
Fig. 1
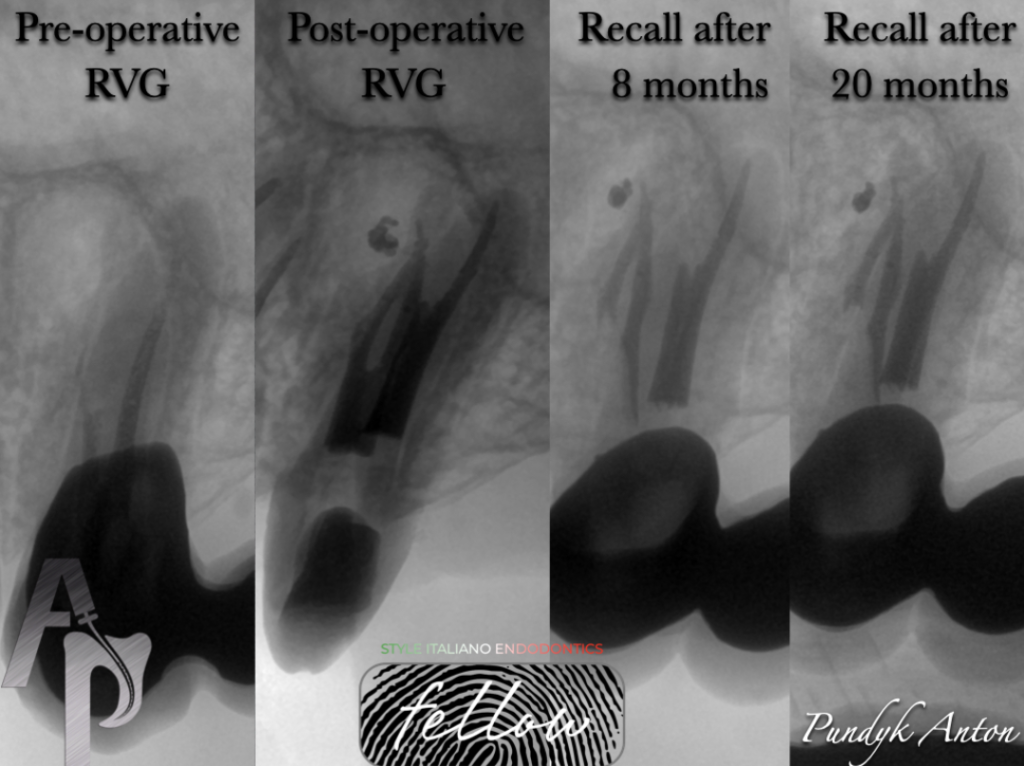
The patient 38y,male,was referred by the his doctor for NSRCT on tooth # 25.During addmision,PMF’s bridge was placed on abutment on teeth #24,#25 and #27 with pontic on tooth #26.Tooth #2.6 was extracted over 10 years ago.Patient didn’t any complaints,percussion-,swelling-,sinus tact-.One digital periapical radiograph was taken.Radiopaque area was identified on lateral side of roots #2.5,short obturations
Diagnosis:Previously treated 2.5,Asymptomatic apical periodontitis 2.5

Fig. 2
Anesthesia was performed by STA Unit.Isolation was performed at split-dam technique.Diamond bur S6856.314.016(Komet) removed ceramic surface of PFM crowns and bur H34l.314.012(Komet) was used for cutting metal part of crown.

Fig. 3
Examination of the pulp chamber with the surgical operating microscope revealed a mummified pulp tissue.The pulp tissue was removed with ultrasonic tip and endodontic explorer.The Buccal and Palatal canals were located.
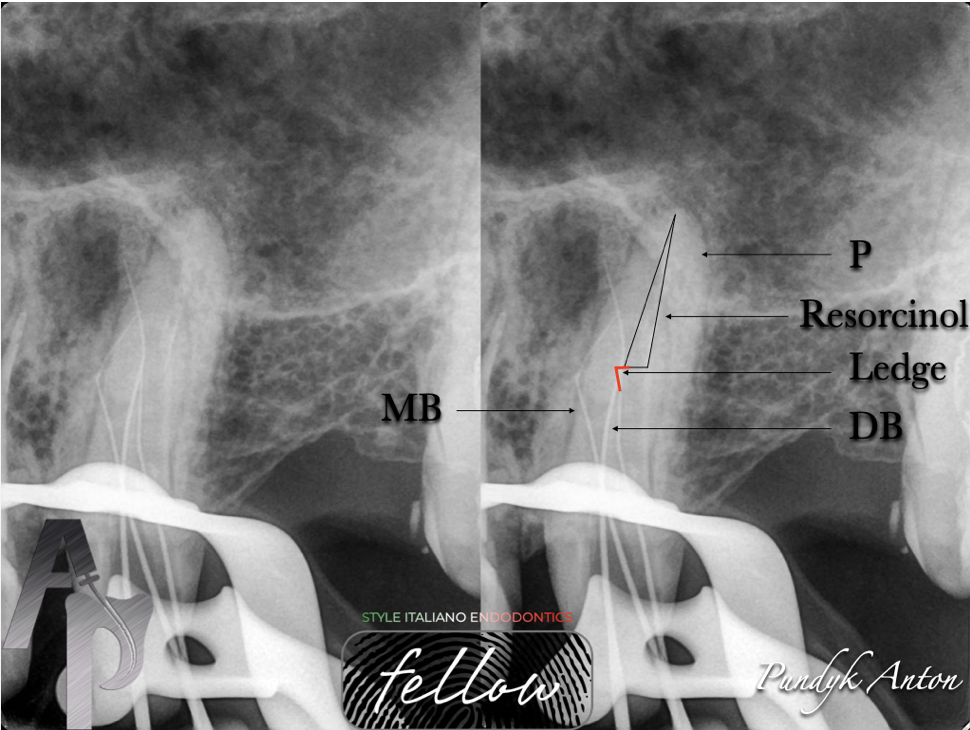
Fig. 4
Further examination showed that Buccal root had deep split-MB and DB rc.Bypass two ledges was performed by precurved C-Pilots(VDW) 06.02-10.02,K-File 15.02,20.02 with combination low speed handpiece M4(Sybron Endo).The canals were instrumened to WL to 15.02 K-File.The MB,DB and P canals were cleaned with E3 Azure(EndoStar) using crown-down technique to a size 30.04 and size 35.04,respectively.The canals were irrigated with 5,25% NaOCL,40% Citric Acid and RC-Prep was used for file lubrication.IrriFlex and EddY is the best choice for irrigation’s stage
Paper points were used to dry tha canals

Fig. 5
Bypass-not easy procedure.
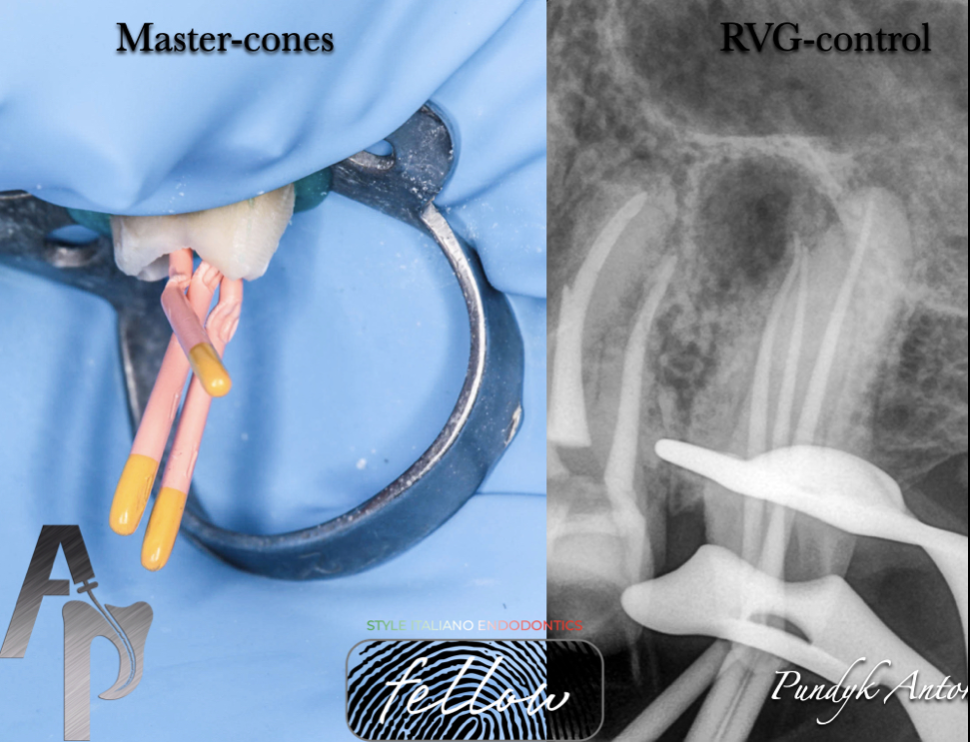
Fig. 6
Radiograph control of fitting master points. 20.04 gutta points were verified on the gauge of guttapercha points(Dentsply/Sirona)
Length Size ISO Taper
MB 17.0 30 .04
DB 17.5 30 .04
P 18.0 35 .04

Fig. 7
Obturation of the canals were completed by warm vertical compaction using AH Plus Root Canal Sealer to cat the guttapercha cones and canals walls.A heat source and pluggers were used to heat and compact the GP.The remaining canal space was backfilled with warm GP to the level of the canals orifices.Pulp chumber was cleaned with an alcohol+brush,drying,Air Flow.A dry cotton pellet was placed in the pulp chamber and the access cavity was sealed with IRM.Patient was finished treatment at his doctor

Fig. 8
I have a remarkable result 20 months later

Fig. 9
About the author:
Anton Pundyk
Born in 1984 in Tumen,Russia.
Studied National Pirogov Memorial Medical University,Vinnitsa and graduated in 2008.
Author articles regarding endodontics on Ukrainian dental magazine "DentArt" and using of the operating micropscope in everyday practice.
Since 2017 he is working in private clinic in Vinnitsa,Ukraine. The main specialization is an endodontics,cad/cam and aesthetic dentistry.
Conclusions
Clinicians should be aware of the potential anatomical endpoints of the maxillary premolars and possess the ability to apply their own knowledge in clinical and X-ray interpretation.Complex premolar anatomy can be treated with predictability after receiving proper diagnosis.
Bibliography
1) Gorni Fabio(2006) The use of Ultrasound in Endodontics.ROOTS international magazine of endodontology 1(1):58-65
2) Vertucci F.J.,Seeling A.,Gillis R.(1974)Root canal morphology of the human maxillary second premolars.Oral Surgery.38:456-464
3) Sjeraski S.M.,Taylor G.N.,Kohn R.A.(1989) Identification and endodontic management of three-canaled maxillary premolars.Journal of Endodontics.15:29-32
