

Retreatment of a first mandibular molar with three independent mesial canals
04/09/2023
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Completing the main objectives of our treatment is not simple. We must be able to clean mechanically and chemically the root canal system in order to seal the internal anatomy and protect the periapical tissues.
For that reason, it is very important to understand the anatomy of the teeth and know the different anatomical variations that we can face in the clinic.
Mandibular molars are one of the most complex anatomical challenges that we can find in our daily practice.
The presence of an additional middle canal is not something strange. Although it can be found in both roots, it is more frequent in the mesial, and according to literature, the prevalence of the middle mesial canal in the mesial root is up to 53,8%, while in the distal root is up to 10%.
It can be found in the middle of the bucal and lingual canals, or closer to one of them and are usually narrower than the main canals. It is very important to be careful and understand if the canal is independent or not and do a proper shaping without risking the pericervical dentine.
A classification for the configuration of the middle mesial canal has been described by Pomeranz et al. They described three types of middle mesial canal:
Independent, confluent (Middle mesial joins bucal or lingual canals) and fin (an isthmus is present in any stage of the way from the orifice to the apex.

Fig. 1
A 40-year-old patient comes to the office with severe pain after broken his composite filling while eating.
Exploring the preoperative X-ray we can see the presence of a threaded post in the mesial root and incomplete cleaning and shaping of both roots, especially the mesial one.
Following the Recommendation 3 of the AAE and AAOMR Joint Position Statement we take a CBCT for suspecting complex anatomy with some extra canal.
The diagnosis was previously treated tooth with symptomatic apical periodontitis.
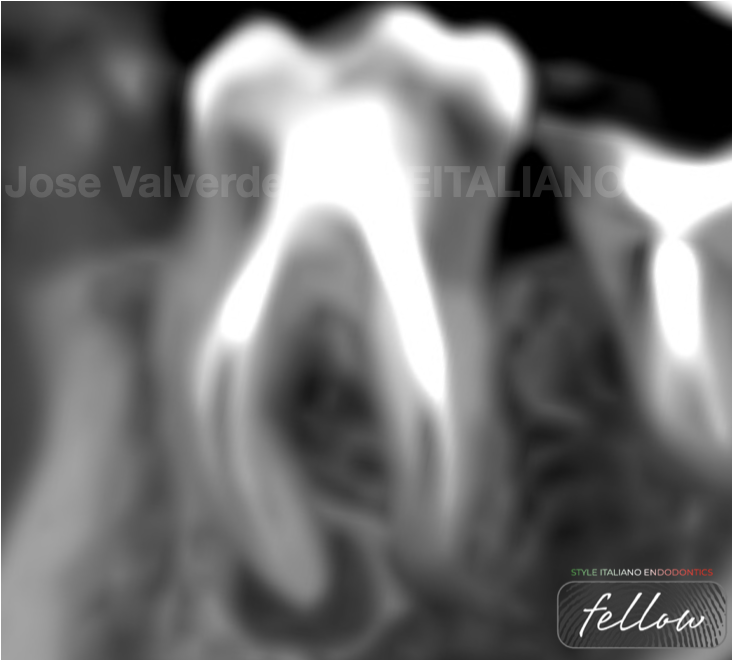
Fig. 2
Image of the sagittal plane of the CBCT where we can see the apical periodontitis because of an incomplete treatment of the two roots and additional canals in both.
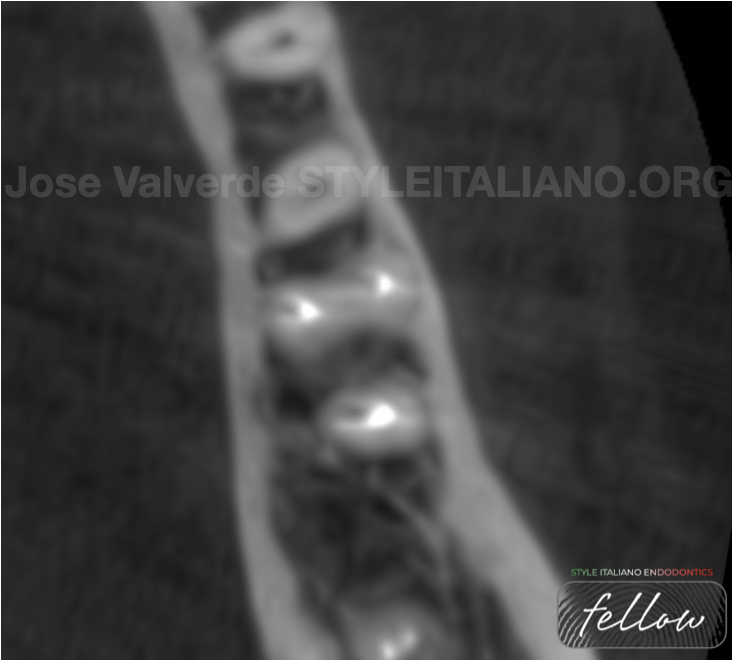
Fig. 3
Image of the axial plane of the CBCT showing the distance between mesial canals and the extra canal in the distal root.

Fig. 4
Image of the coronal plane of the CBCT showing the complexity of the mesial root and all its canals.
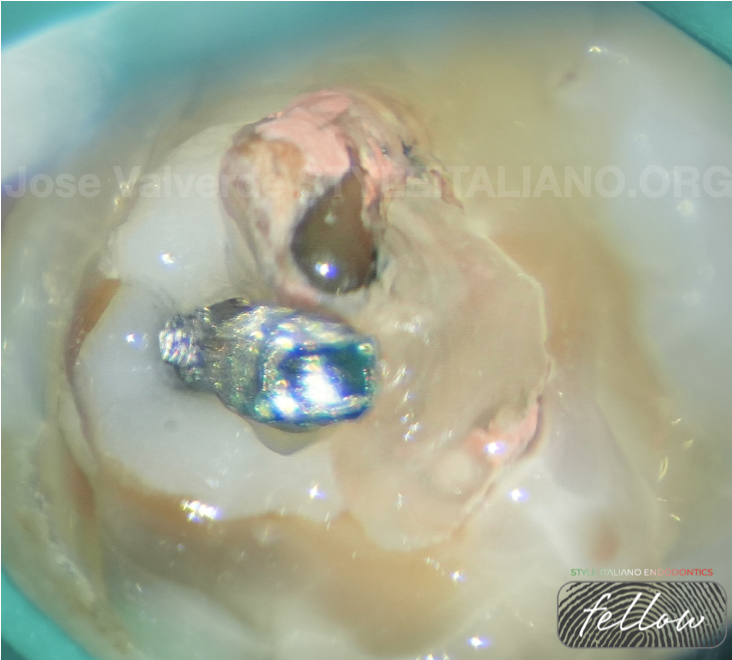
Fig. 5
First of all we have to eliminate the old composite filling and then, we can see the threaded post and remains of cement in the pulp chamber.
In this case, we cleaned the cement and removed the threaded post with a ultrasonic tip.
Once the pulp chamber was cleaned, we activated the tip for removing the post, unscrewing it in an anticlockwise direction.
It is important not to apply lateral forces with the ultrasonics in order to avoid a root fracture.
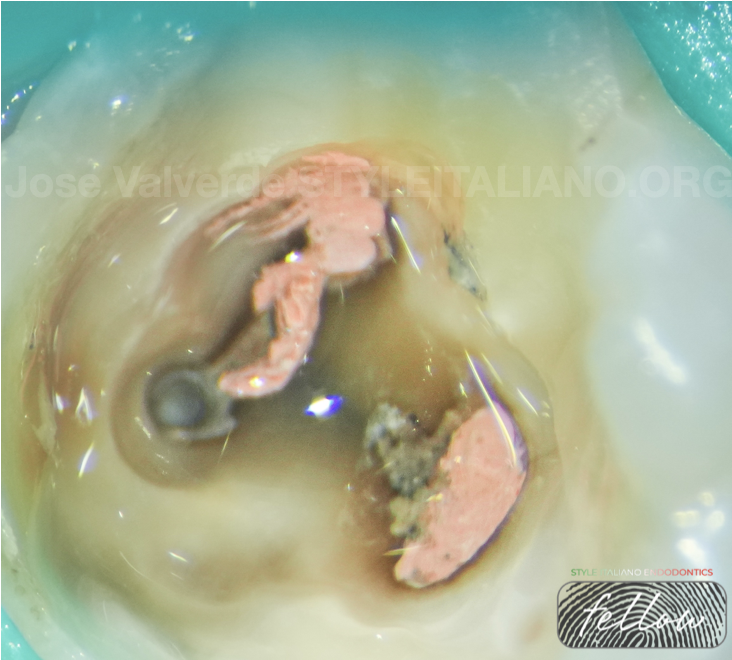
Fig. 6
After cleaning the pulp chamber and removing the threaded post, we can see there is some gutapercha inside the mesial isthmus.
We use a Micro-Opener for looking for the middle mesial in this area.
The cleaning of the isthmus was carried out with EndoTracer 004 (Komet) for eliminate any coronal interference.
Once we found the middle mesial, we filled the chamber with 4,25% NaOCL and removed the coronal gutta-percha using a Gates Glidden number II. For the middle third we used a heat treated file.
As soon as the coronal and middle third was cleaned, we measured for the first time the canals and confirmed that the mesial canals were independent. Then, proceeded to clean the apical area using Hedstroem and K-Files.
We repeated the measuring of the canals after the apical third was completely cleaned and ended up increasing the apical preparation up to 35/03 in mesials and 40/03 in distals.
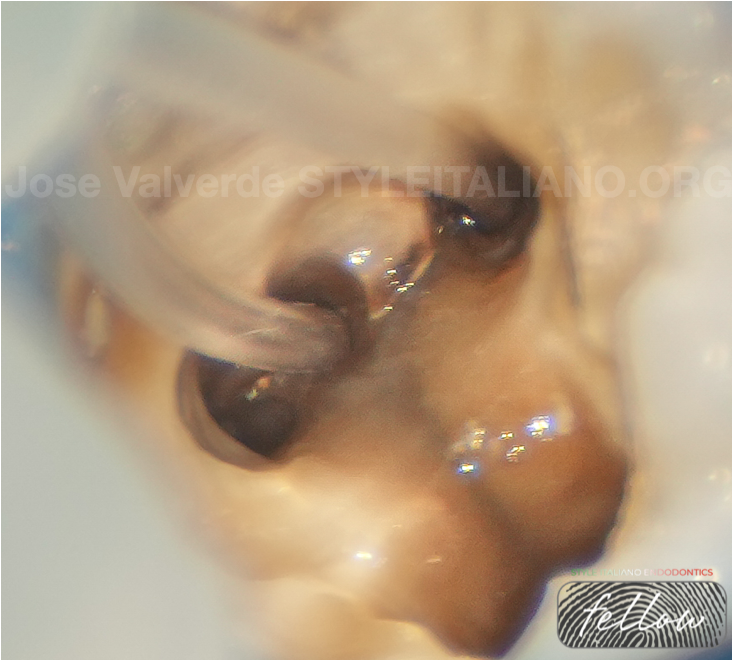
Fig. 7
During all the treatment, 4,25% NaOCl was used, filling the pulp chamber while shaping and cleaning all the canals after the entrance of each file.
Right after the mechanical disinfection was completed, we started the final irrigation protocol.
Ultrasonic activation of 4,25% NaOCl in all canals, followed by apical negative pressure, with both 4,25% NaOCl and 17% EDTA, using a tip that allow us to reach the apical third without any problem.
In this case we used Irriflex for the suction and delivery of the irrigants to the apical third.

Fig. 8
Final rinse with 4,25% NaOCl without any kind of activation and after that, physiological serum to clean the remains of the irrigants before obturation.
All the canals were dried with paper points, leaving them with moisture, since in this case, we used an hydraulic cement for the obturation.

Fig. 9
For the obturation, we gauged the 4% gutta-percha cones up to 40 in mesial canals and 45 in distals.
We delivered a heat compatible BC sealer to the middle third and brought the gutta-percha cones to the working length using soft pressure, without pumping the cones.
After that, warm vertical compaction was performed for the final obturation of all the canals.

Fig. 10
Orthoradial projection, showing the untreated anatomy of both roots and the correct filling of all the canals.

Fig. 11
Mesioradial projection shows the three canals in the mesial root and gives us a better projection of the Vertucci Type II configuration of the distal root.

Fig. 12
Distalizing the X-Ray focus we can see the three independent mesial canals more clearly, showing a Vertucci type VIII configuration.

Fig. 13
About the author: José Valverde
- 2009-2014: Graduated in dentistry from the Alfonso X El Sabio University
- 2016-2019: European Master in Microscopic Endodontics and Apical Surgery from the Rey Juan Carlos University
- In 2023 he has started the PhD program in Universidade Grande Rio
- Professor of the Master in Microscopic Endodontics and Apical Surgery at Rey Juan Carlos University
- Professor of the Expert in Endodontics and Apical Surgery at Universidad La Salle
- Titular Member of the Spanish Association of Endodontics (AEDE)
- Member of the American Association of Endodontics (AAE)
- Member of the International Association of Dental Traumatology (IADT)
- Fellow Member of Style Italiano Endodontics
- Opinion Leader for Zarc4Endo
- He has been an active participant in national and international endodontic congresses, such as AAE, ESE, AEDE or IFEA.
- He works as exclusive endodontist in Gran Canaria, Spain, and is dedicated to research and education
Conclusions
The middle mesial canal is an anatomical variation of the mesial root that we have to know and control if we want to succeed in the disinfection of the root canal system.
When we are facing complex cases in which we suspect that there is extra canals or additional anatomy the use of CBCT can help us to create an strategy for our treatment.
Combining the knowledge of the anatomy with magnification and the adequate instruments is a key factor for obtaining success in the treatments performed in our practice.
Bibliography
MARTÍNEZ-BERNÁ, Arturo; BADANELLI, Pedro. Mandibular first molars with six root canals. Journal of endodontics, 1985, vol. 11, no 8, p. 348-352.
VERSIANI, Marco Aurélio, et al. Middle mesial canals in mandibular first molars: A micro-CT study in different populations. Archives of oral biology, 2016, vol. 61, p. 130-137.
POMERANZ, Howard H.; EIDELMAN, David L.; GOLDBERG, Mitchell G. Treatment considerations of the middle mesial canal of mandibular first and second molars. Journal of endodontics, 1981, vol. 7, no 12, p. 565-568.
SIQUEIRA JR, José F., et al. Correlative bacteriologic and micro–computed tomographic analysis of mandibular molar mesial canals prepared by Self-Adjusting File, Reciproc, and Twisted File systems. Journal of endodontics, 2013, vol. 39, no 8, p. 1044-1050.
NOSRAT, Ali, et al. Middle mesial canals in mandibular molars: incidence and related factors. Journal of endodontics, 2015, vol. 41, no 1, p. 28-32.



