
Rare anatomy Fusion+ Dens in dent Type ااا in upper lateral incisor.
05/03/2026
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
The management of a necrotic maxillary lateral incisor presenting with fusion and Type III dens invaginatus associated with a periapical lesion represents one of the most biologically and technically demanding scenarios in contemporary endodontics. The coexistence of fusion—resulting in enlarged crown morphology and complex, often interconnected canal systems—with Type III dens invaginatus, characterized by a deep enamel-lined invagination extending through the root and communicating with the periodontal ligament, creates a highly irregular internal anatomy. This configuration permits early microbial contamination through the invaginated tract, often leading to pulpal necrosis and extensive periapical pathology independent of the primary canal system . Effective management requires a precise diagnosis supported by three-dimensional imaging, particularly CBCT, to delineate the true canal anatomy, identify separate foramina, and assess the extent of the periapical lesion. Treatment should follow a biologically based protocol focused on maximal disinfection while preserving structural integrity. Careful access under magnification, ultrasonic refinement, and strategic negotiation of both the main canal and invaginated lumen are critical. Enhanced irrigation protocols with activation techniques are essential to address inaccessible recesses. Intracanal medicaments such as calcium hydroxide may aid in microbial control prior to definitive obturation. In cases of persistent pathology, obturation for dens in dente must be done with bioactive biocompatible material to achieve good seal in Periodontal ligament area.

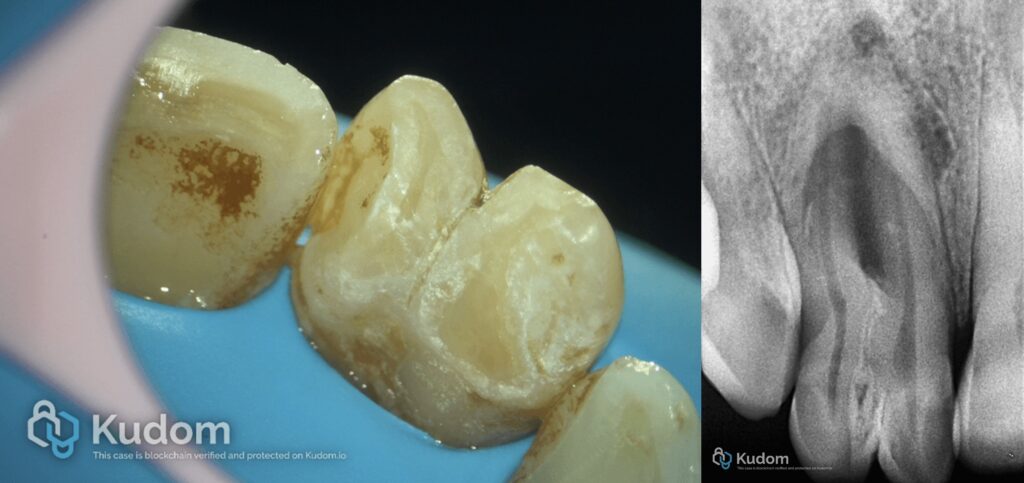
Fig. 1
Starting with isolation prevents contamination, enhances visibility, and ensures a dry, clean environment for effective root canal treatment.

Fig. 2
Preoperative Xray
Video of the procedure
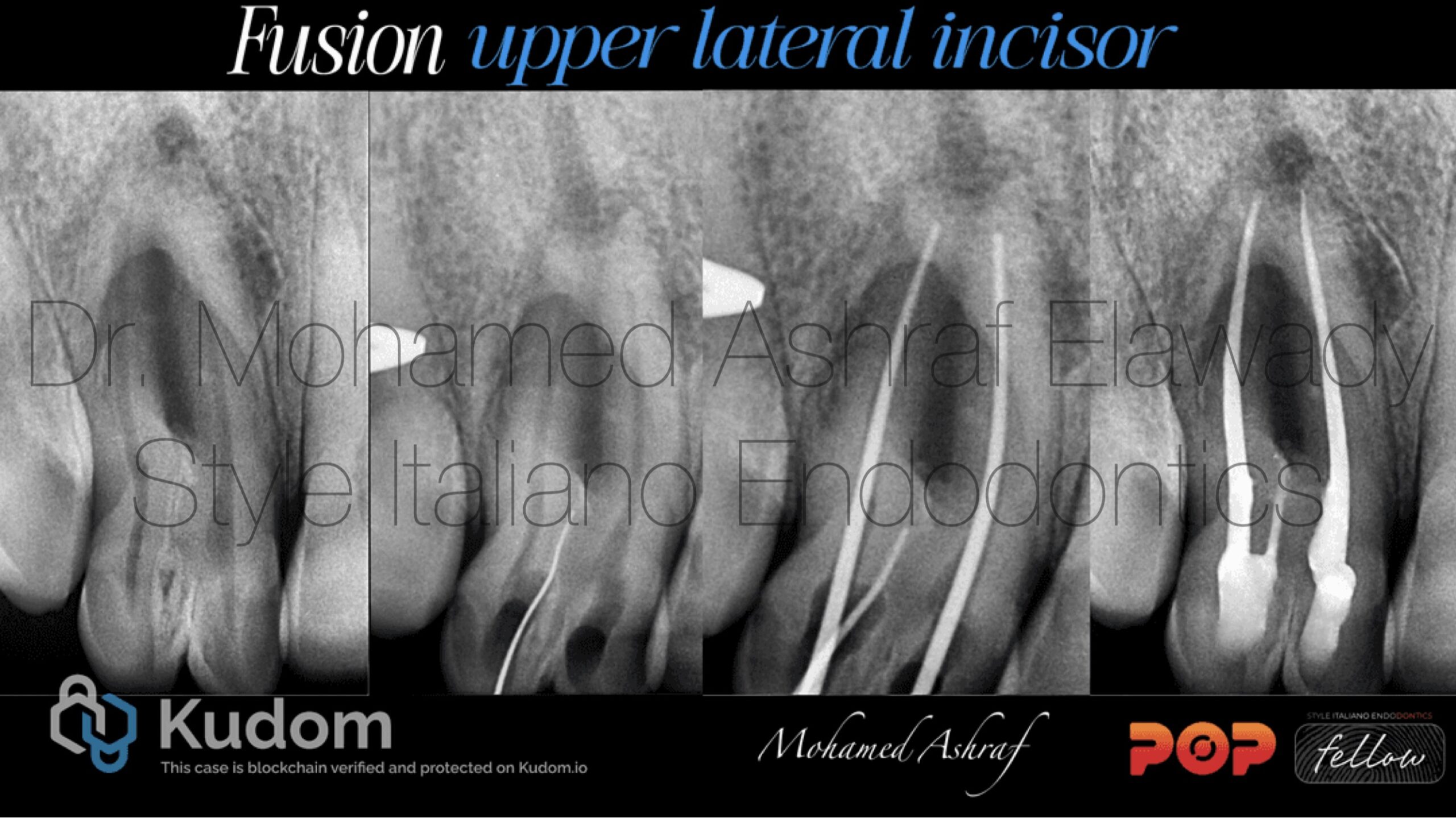
Fig. 3
Full case

Fig. 4
Obturation with ah plus resin sealer and gutta-percha for the 2 main canals and mta for dens in dent as bioactive biocompatible material for Sealing this area, play a vital role in obturation by providing excellent sealing properties, biocompatibility, and resistance to shrinkage. Their hydraulic properties allow them to adapt well to canal irregularities, offering superior resistance to bacterial penetration, promote tissue healing, enhancing long-term outcomes.

Fig. 5
MOHAMED ASHRAF ELAWADY Speaker of endodontics. Cofounder of care dental clinic, Egypt. Endodontic consultant in multiple private clinics. microscopic endodontist 2019. Style italiano endodontics fellow member.
Conclusions
In conclusion, nonsurgical endodontic management of a necrotic maxillary lateral incisor with fusion and Type III dens invaginatus can achieve predictable outcomes when guided by thorough diagnosis and a biologically driven protocol. Careful CBCT assessment, magnification-assisted access, meticulous chemo mechanical preparation, and activated irrigation are essential to disinfect the complex anatomy. The use of intracanal medication and three-dimensional obturation further enhances healing potential. With precise execution, nonsurgical treatment alone can promote resolution of periapical pathology and long-term tooth preservation.
Bibliography
1. Hülsmann M. Dens invaginatus: Aetiology, classification, prevalence, diagnosis, and treatment considerations. Int Endod J. 1997;30:79–90 2. Akers HF, Henderson CM, Foley MA. Diagnosis and management of a maxillary lateral incisor exhibiting dens invaginatus and dens evaginatus. Aust Endod J. 2014;40:32–8
3. Kirzioǧlu Z, Ceyhan D. The prevalence of anterior teeth with dens invaginatus in the western Mediterranean region of Turkey. Int Endod J. 2009;42:727–34. 4.OEHLERS FA (1957a) Dens invaginatus. I. Variations of the invagina- tion process and associated anterior crown forms. Oral Surgery, Oral Medicine and Oral Pathology 10, 1204–18
5.OEHLERS FA (1957b) Dens invaginatus. II. Associated posterior crown forms and pathogenesis. Oral Surgery, Oral Medicine and Oral Pathology 10, 1302–16. 6.Ali A, Arslan H, Jethani B. Conservative management of Type II dens invaginatus with guided endodontic approach: A case series. J Conserv Dent. 2019 Sep-Oct;22(5):503-508.
