
Preservation-focused management of a hemisected maxillary molar- a case report
11/05/2026
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Historically, root-resection therapy (hemisection, root amputation) has been advocated primarily for molars with furcation involvement, root caries, root fracture or advanced periodontal disease. In appropriately selected cases, root resection offers a valid alternative to extraction. From a biomechanical standpoint, removal of a root inevitably reduces root mass and supporting bone area, leading to increased stress concentration in the remaining tooth structure under function. This underscores the importance of careful case selection, consideration of occlusion and load distribution, and optimal prosthetic restoration after resection.
In this clinical case, patient presented with a fractured coronal wall of the maxillary first molar. Clinical and radiographic evaluation revealed a previously endodontically treated tooth with chronic apical abscess and a palatal wall fracture that precluded conservative restoration. Treatment alternatives included extraction with implant placement or palatal hemisecion combined with orthograde retreatment of the mesiobuccal and distobuccal roots. A conservative approach was selected also based on the patient’s desire to retain the tooth. The buccal roots were successfully retreated, and the tooth was subsequently restored with an indirect coronal restoration.
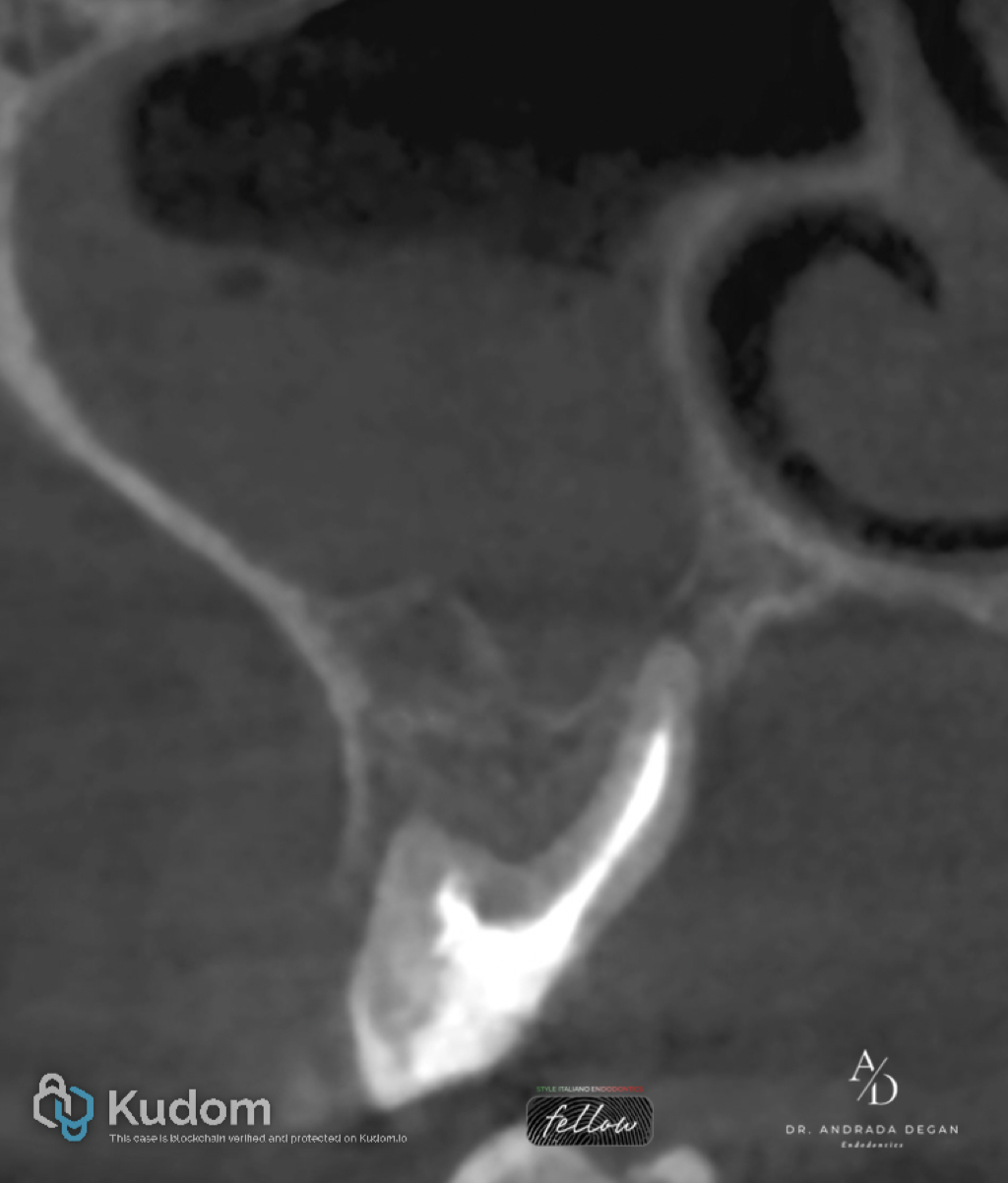
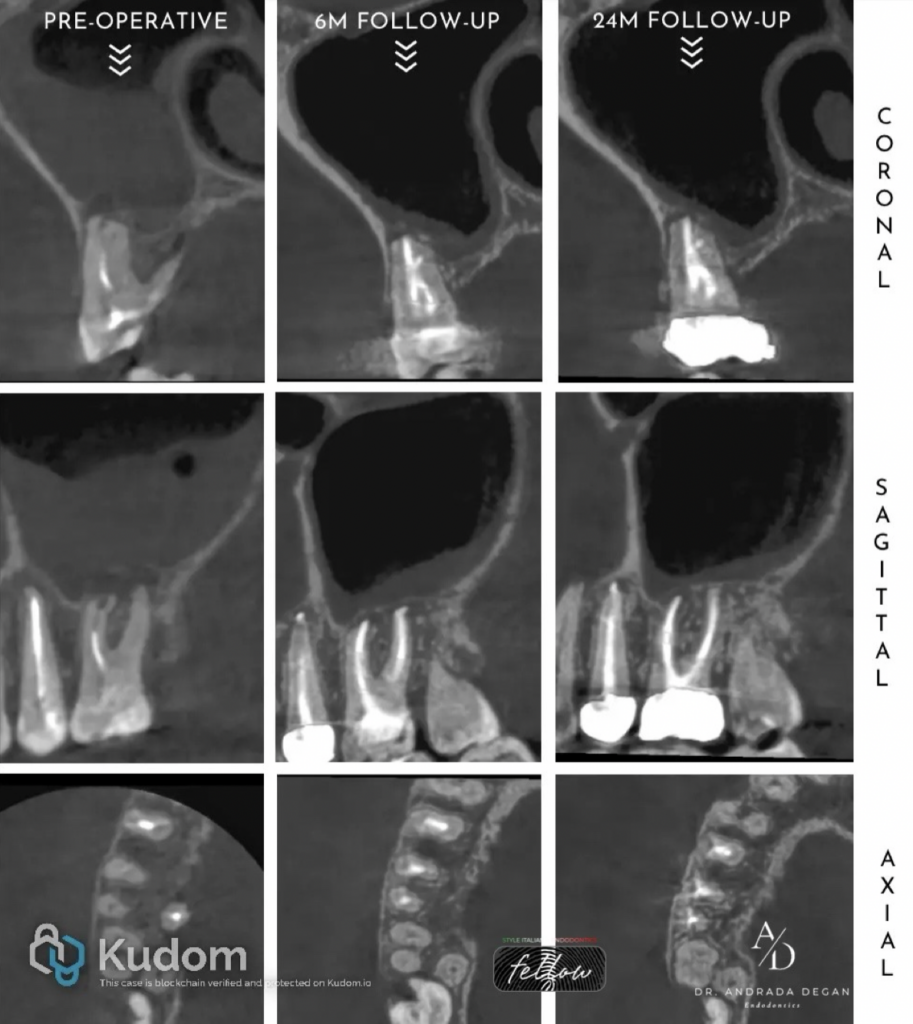
Fig. 1
Clinical and radiological findings
Following the patient interview and comprehensive clinical examination, the following findings were recorded:
Subjective findings: The patient reported no pain or discomfort.
Objective findings: On inspection, the tooth exhibited a large disto-occlusal restoration with inadequate marginal adaptation and associated secondary caries. An oblique subgingival fracture of the palatal coronal wall was evident. A sinus tract with purulent drainage was observed in the palatal gingival sulcus. Vertical percussion was negative, whereas horizontal percussion elicited a slight positive response. Palpation in the buccal vestibule at the level of the root apices was non-tender. The tooth was asymptomatic under biting pressure and exhibited no mobility. Periodontal probing depths were within normal limits on the mesiobuccal, distobuccal, and mid-buccal aspects, while on the palatal aspect a periodontal defect exceeding 15 mm was detected.
Radiological findings CBCT Scan-Coronal view of the anatomical crown showing a fracture of the palatal wall with the palatal root in a floating condition.
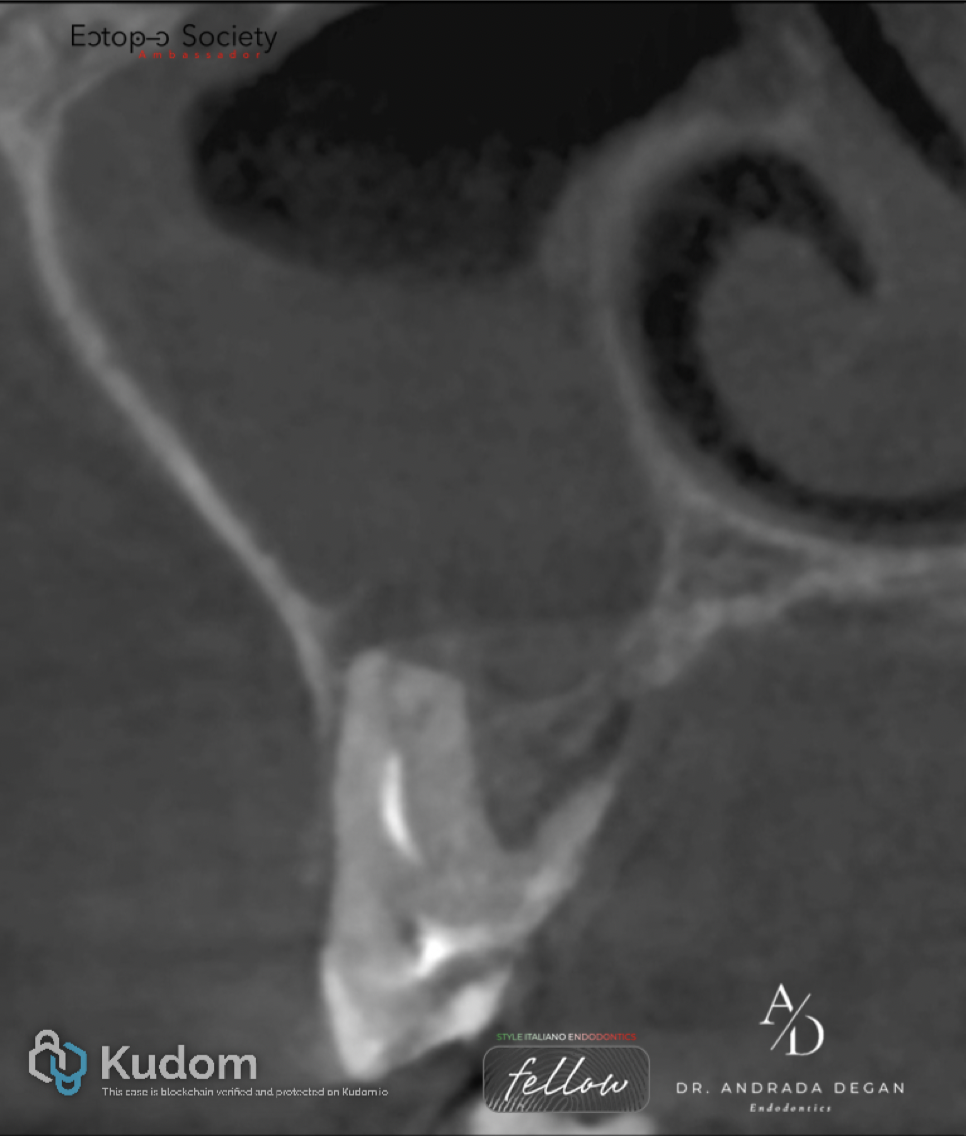
Fig. 2
Pre-Operative: Coronal view of the MB root showing un untreated Vertucci Type VI (2–1–2) canal configuration. This CBCT image is showing the apical periodontitis perforating the antral cortical floor and periosteum causing an inflammatory thickening of the sinus mucosa.
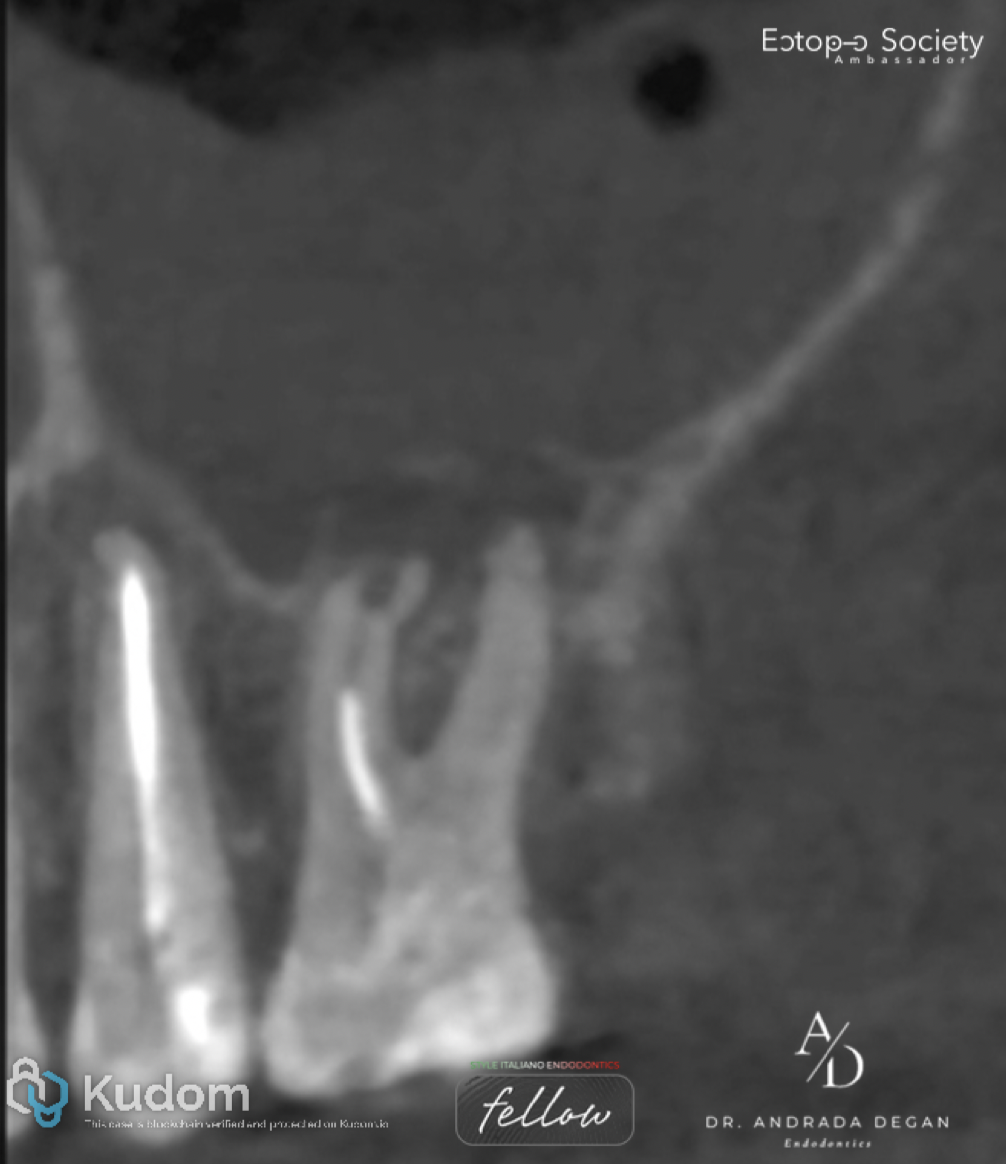
Fig. 3
Pre-Operative: Sagittal view of the MB and DB roots shows an external apical resorption on both roots and an inflammatory internal resorption in the apical third of the MB root.

Fig. 4
Pre-Operative: Axial view of the roots in the middle to apical third

Fig. 5
Pre-Operative: Axial view of the roots in the apical third
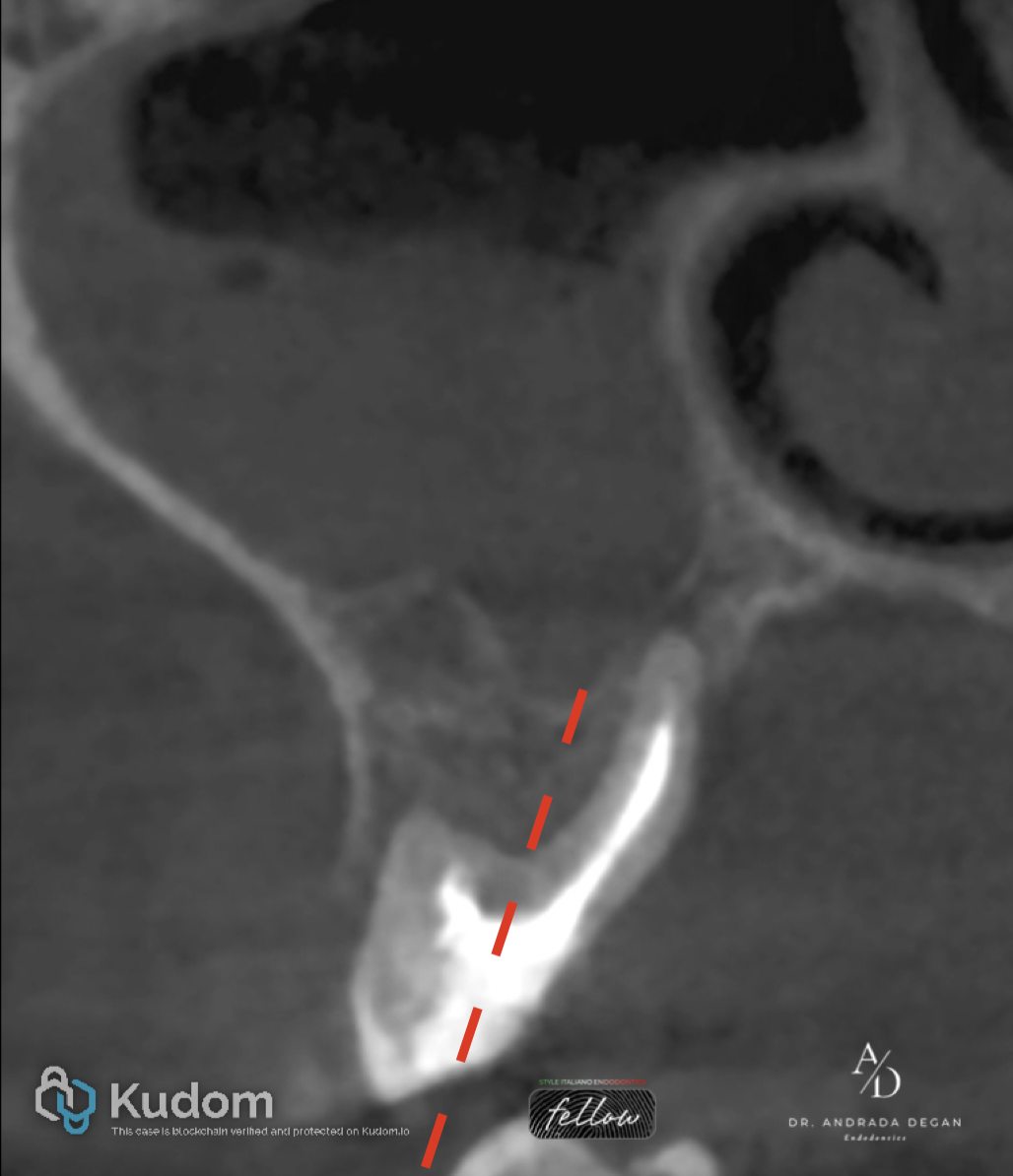
Fig. 6
Treatment plan:
Hemisection of the palatal portion of the molar through a mesiodistal section of the tooth, followed by orthograde retreatment of the remaining roots.
From a restorative standpoint, an immediate full-coverage PMMA provisional crown was selected until the first follow-up appointment. This decision aligns with current evidence highlighting the importance of timely cuspal coverage following endodontic treatment. As reported by Bhuva, Giovarruscio, Rahim, Bitter and Mannocci, posterior teeth exhibit significantly improved survival rates when restored promptly, whereas even a 4–6-month delay may negatively influence long-term outcomes
First appointment:
A mesiodistal section at the level of the pulp chamber floor of the maxillary first molar was performed, separating the buccal roots from the palatal root, followed by extraction of the palatal root. The procedure was carried out by an oral surgeon

Fig. 7
Second appointment
Isolation was achieved using a rubber dam applied to teeth 1.7–1.5. A primary W3 clamp Tor VM was placed on tooth 1.7, supplemented by an additional W8A clamp (Hygenic Fiesta, Coltene) on tooth 1.6, with Teflon tape used to enhance sealing and stability.
Access cavity preparation involved complete removal of the existing restoration along with the underlying carious tissue, ensuring clean margins and proper visualization. This was followed by a pre-endodontic build-up to re-establish coronal structure and facilitate subsequent procedures.
The rubber dam isolation was then readjusted to optimize access and visibility, particularly for the mesiobuccal (MB) root, ensuring effective moisture control throughout the endodontic phase.

Fig. 8
Pre-flaring of the coronal third of the MB1 and DB root canals was performed using a 25/12 rotary instrument. Working length was established using D-Finder ISO size 10 manual files. This step was followed by glide path preparation of the canals with 15/03 rotary files. Shaping and finishing were completed using a crown-down technique.
The MB1 canal was prepared to a final size of 40/04 at a working length of 16 mm. The DB canal was prepared to 35/04 at a working length of 16.5 mm. The MB2 canal was identified and negotiated, merging with MB1 at approximately 15 mm and then they split again in the apical third. Apical gauging was performed with K-files, confirming an apical diameter of ISO #45 for MB1 and ISO #35 for DB.
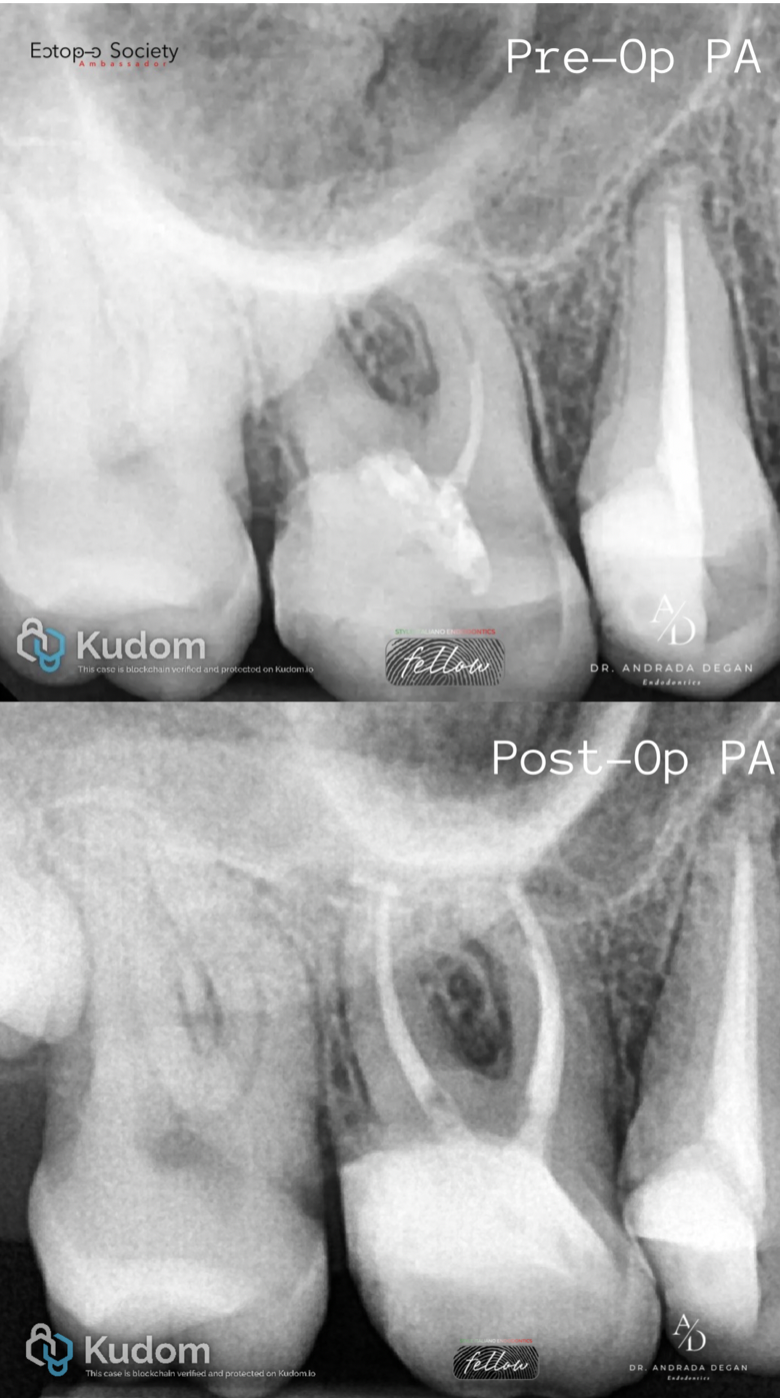
Fig. 9
Final irrigation was performed using 5.25% sodium hypochlorite solution with 5 mL delivered per canal and activated by passive ultrasonic irrigation. This was followed by irrigation with 17% EDTA solution for 1 minute per canal to remove the smear layer, and a final flush with 0.9% saline solution.
Root canal obturation was carried out using a single-cone technique in combination with a calcium silicate–based sealer.
The coronal third of both canals, as well as the pulp chamber, were restored using a fiber-reinforced bulk-fill composite material. This approach provided internal reinforcement of the remaining tooth structure while preserving as much dentin as possible.
Evidence-based guidelines differ regarding post placement. Atlas, Grandini and Martignoni indicate that a fiber post may be appropriate when only one coronal wall remains, improving retention of the build-up material to the residual tooth structure. In contrast, Carvalho et al. show that when an adequate ferrule is available, posts are not required for adhesive restorations and may even increase catastrophic failures.
In this particular case, MB1 and DB root canals were too narrow and delicate for post placement without unnecessary dentin removal.
Chosen approach: glass-fiber-reinforced bulk-fill composite in the coronal third of both canals + core build-up.
Rationale: maximize dentin preservation while providing internal reinforcement.
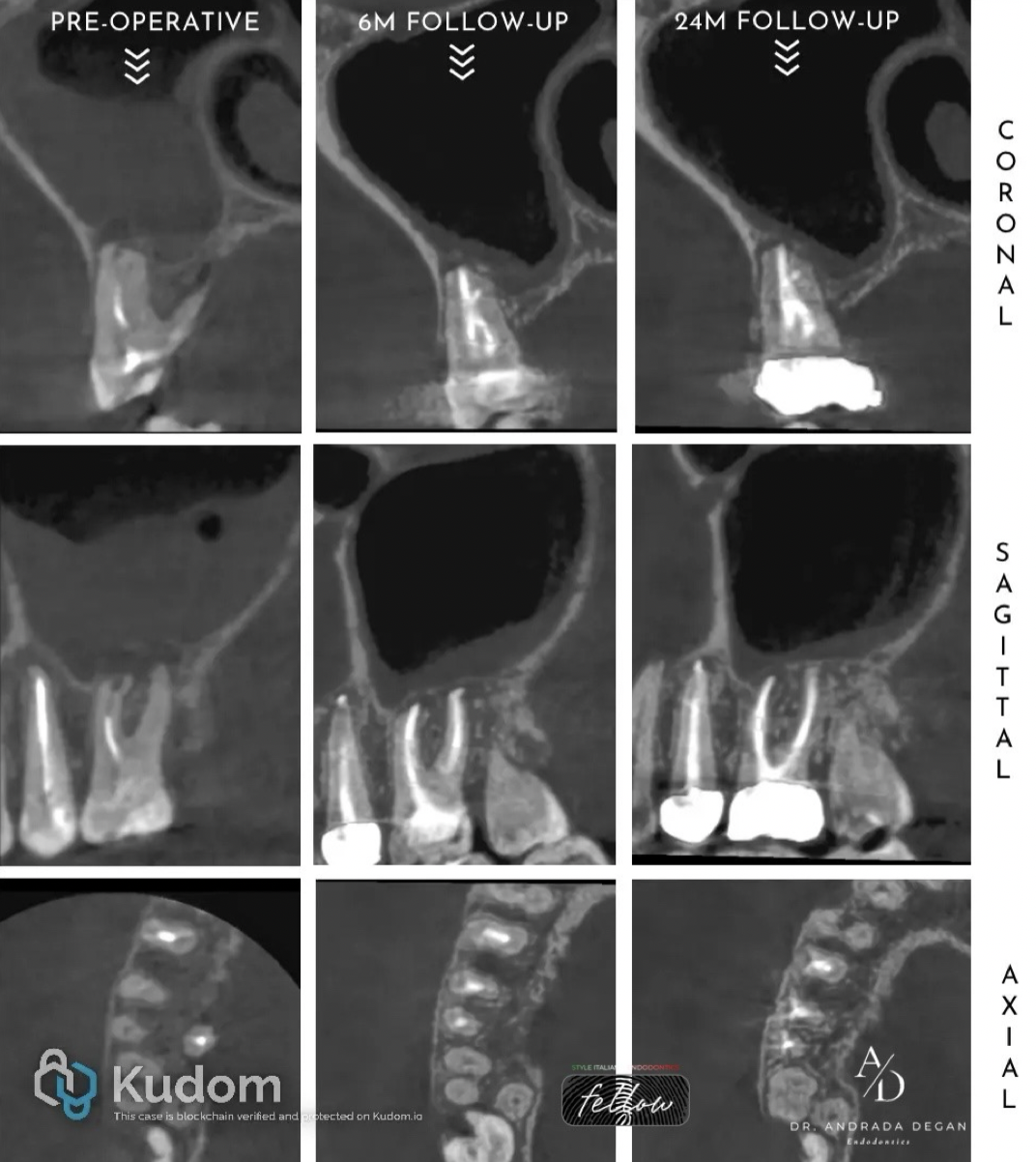
Fig. 10
Follow-Up:
Following the 6-month follow-up, significant healing of the periapical lesions associated with the buccal roots of the molar was observed, as well as a resolution of the sinus mucosa inflammation. The tooth was still asymptomatic, and the periodontal probing depths on the buccal aspect were within normal limits (WNL), while on the palatal aspect they measured 5,5 mm. Based on this assessment, the patient was subsequently referred to the prosthodontist for a long-term restoration- a zirconia crown.
Following the 24-month review, the radiological condition of the tooth had slightly improved compared with the previous follow-up. The tooth remained asymptomatic and maintained its function within the arch.

Fig. 11
Follow-Up:
Clinical aspect of the final restoration of the tooth at the 24-month follow-up.

Fig. 12
About the author:
Andrada Degan
Conclusions
The preservation of natural tooth structure is a decisive factor for succesfull restoration of ETT, post space preparation should be kept at minimum in all cases. Instead using a fiber post, the coronal third of both canals and the core were restored using a glass-fiber-reinforced bulk-fill composite, providing internal support while maximizing dentin preservation.
In addition to the general complexity of the case, a particular challenge was the anatomy of the mesiobuccal root. In situations involving resorptive defects at the root level, most studies support the use of calcium hydroxide as an intracanal medicament due to its antimicrobial properties and its ability to inhibit resorptive processes. In the present case, however, calcium hydroxide was not used. Disinfection was achieved relying on the efficacy of ultrasonic activation of sodium hypochlorite, which also allowed thorough debridement of the isthmus and the bifurcation in the apical third of the root.
Bibliography
Atlas, A., Grandini, S., & Martignoni, M. (2019). Evidence-based treatment planning for the restoration of endodontically treated single teeth: Importance of coronal seal, post vs no post, and indirect vs direct restoration. Quintessence International, 50(10), 772–781.
Carvalho, M. A., Lazari, P. C., Gresnigt, M., Del Bel Cury, A. A., & Magne, P. (2018). Current options concerning the endodontically treated teeth restoration with the adhesive approach. Brazilian Oral Research, 32(suppl 1), e74.
Mannocci, F., & Cowie, J. (2014). Restoration of endodontically treated teeth. British Dental Journal, 216(6), 341–346
Bhuva, B., Giovarruscio, M., Rahim, N., Bitter, K., & Mannocci, F. (2021). The restoration of root filled teeth: a review of the clinical literature. International Endodontic Journal, 54(4), 509–535
FALABELLA, M. E. V., de Souza, R. J. S., Dornelas, A. H. C., Vieira, A. D. D., & Soares, L. G. (2021). Root resection in molars – clinical evaluation for 10 years. International Journal of Odontostomatology, 15(2), 492–498
Camargo Dos Santos, B., Pedano, M. S., Giraldi, C. K., Oliveira, J. C. M., Barbosa Lima, I., & Lambrechts, P. (2020). Mesiobuccal root canal morphology of maxillary first molars in a Brazilian sub-population: A micro-CT study. European Endodontic Journal, 5(2), 105–111.
