NSRCT OR EXTRACTION?
05/06/2025
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
The introduction of implant dentistry, in some cases, eliminated the need for non-surgical endodontic retreatment as well as the need for apical surgery. Proverb says: «When you have a hammer, everything around seems to be nails.»
It’s well accepted that non-surgical retreatment of case of previously failed endodontic therapy provides good results.Success rates between 70% and 90% have been reported in several investigations. Conversely, retreatment procedures often are tedious and time consuming so that practitioners may prefer apical surgery or no-intervention even in case of evident failure of previous endodontic therapy.
One of the main problems in retreatment is the removal of the insufficient root canal filling. A great variety of metallic objects are left in the root canal inadvertently for example-fractured endodontic instruments, needles, pins, burs and many other objects.
Retrieval of these intracanal obstructions be extremely difficult but be essential for non-surgical treatment or retreatment.
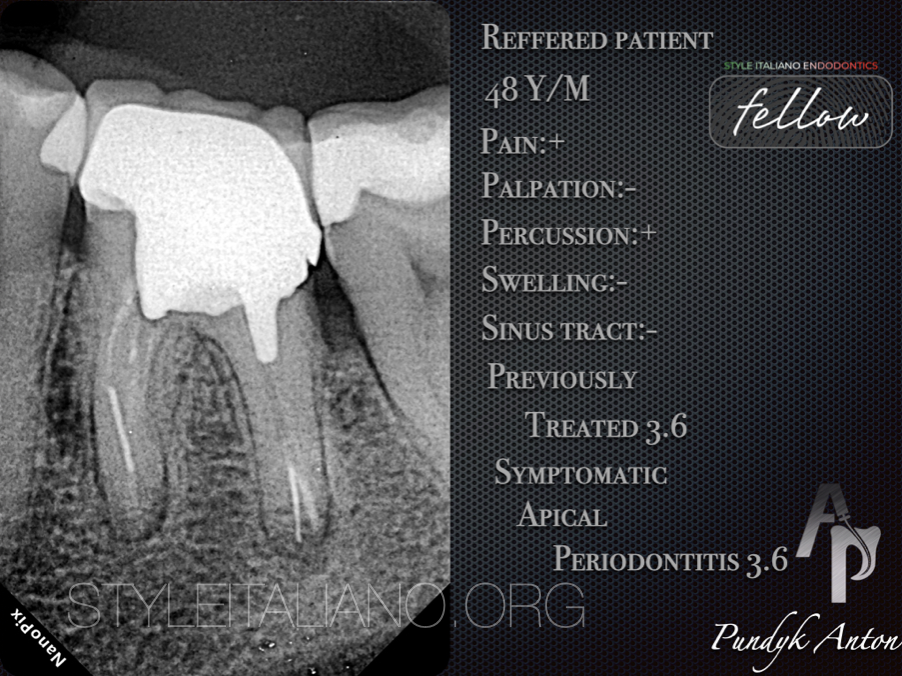
Fig. 1
The patient,48y/male,was referred for an evaluation and treatment of tooth 3.6.
Patient reported a dull pain when biting. The symptoms had started about 3 months previously but symptoms were never severe enough to seek immediate dental care.
Extraoral examination:Examination revealed no swealing,extra-oral fistula or limphadenopathy of the submandibular and neck areas.
Intraoral examination:Soft tissue appeared healthy with no sings of intraoral swelling, fluctuance or sinus tract. Patient had minor gingivitis.
Diagnostic test: - Percussion+
- Palpation-
- Mobility-WNL
Periodantal pocket depth: - Buccal side-less 4 mm
- Lingual side-less 4 mm
- Mesial proximal side-less 4 mm
- Distal proximal side-less 4 mm
Bleeding on probing: +

Fig. 2
Radiographic interpretation:Tooth 3.6 had root canal treatment.There was a full crown with pinlay restoration at the molar area. A threated post in the distal root shoowed a 3-4 mm gap apically to the broken file.
Besides apical transportation was identified in apical third of distal root. In the mesial root, 2 separated files were found. Crestal bone loss was noticed at the interproximal bone between teeth 3.6 and 3.7. The furcation was intact.
CBCT:A definite radiolucency of middle part mesial root was noticed.The coronal portion of the post and root canal filling in the distal root were located slightly off-center towards the buccal aspect.
Diagnosis:Previously treated 3.6, Symptomatic Apical Periodontitis 3.6
Treatment plan:
Recommended-NSRCT 3.6
Alternative-Extraction and replacement with implant fixed partial denture or no treatment
Restorative-Post,core and crown

Fig. 3
Pre-operative view

Fig. 4
Anesthesia was performed with Wand STA(Milestone Scientific) used Ubistesin 4%-1/200000.Isolation split-dam for dismantling coronal build-up was used. Crown removed with Safe Relax.
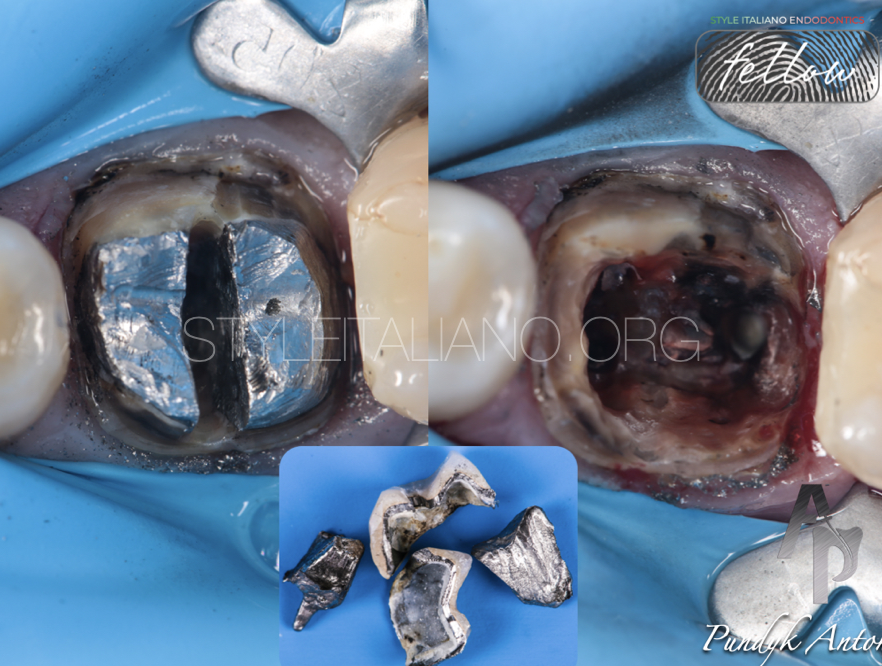
Fig. 5
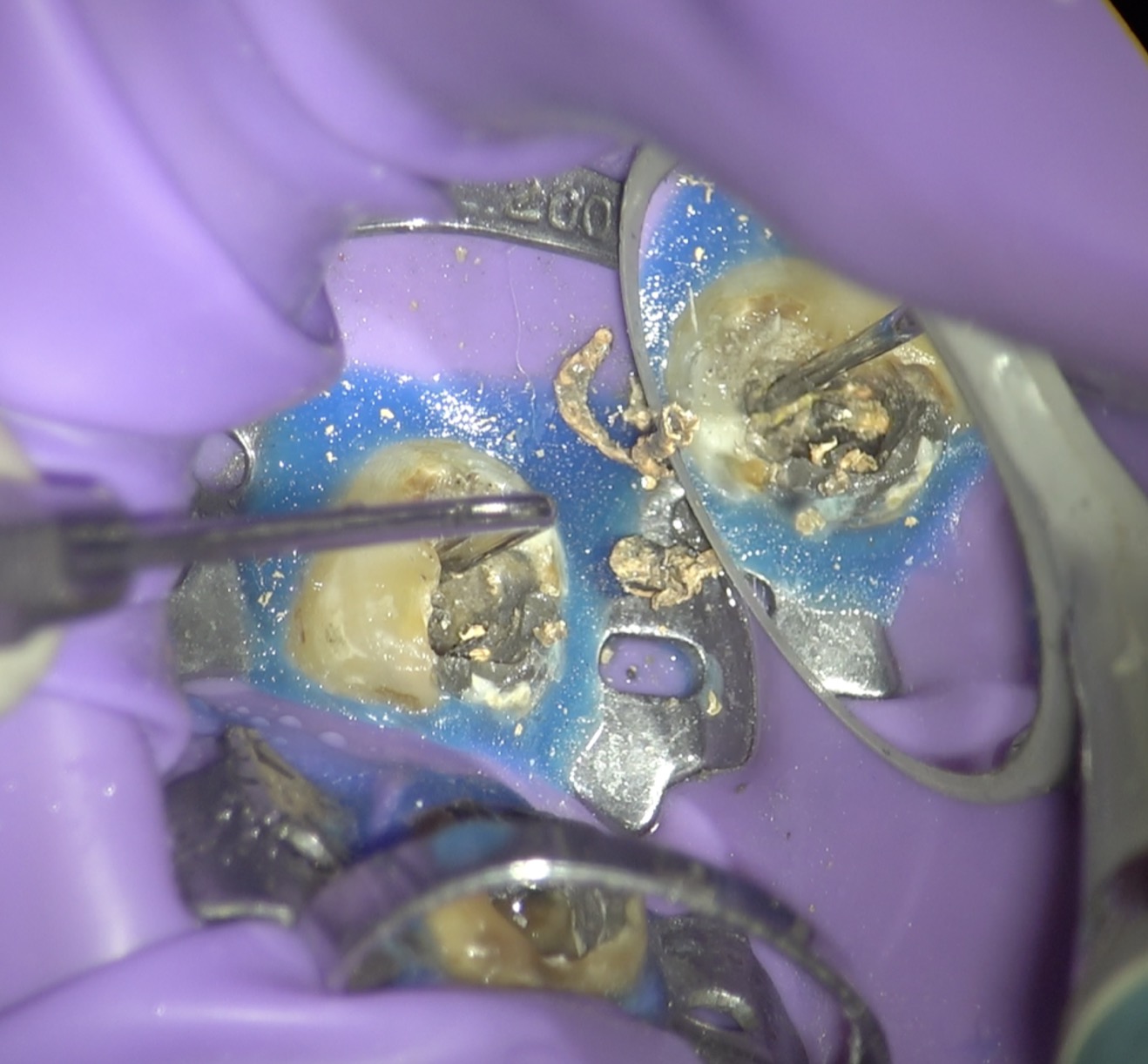
Pinlay was fragmented with bur H34L.314.012 by Komet until it reached a furcation zone under control of operating microscope.Then,two parts of post were extracted with using US tip G26(NSK)&unit Varios 970(NSK)
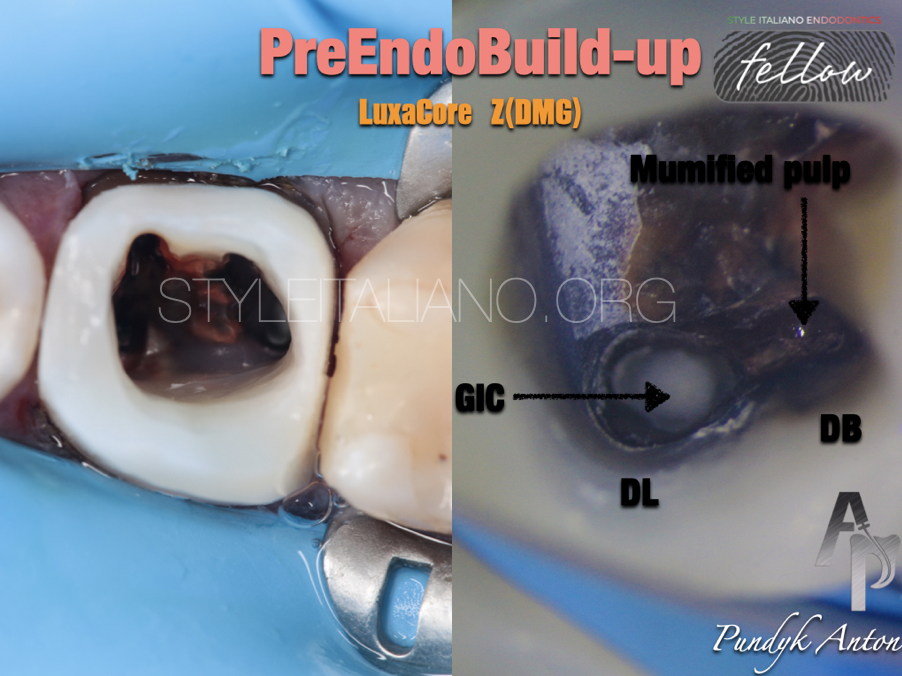
Fig. 6
Build-up phases:
-Sandblasting was performed with RondoFlex(KaVo),abrasive powder-Allustral 50 micron
-Etching-Ultra-Etch(Ultradent)
-Opti Bond FL(Kerr/Sybron Endo)
-Core composite - Luxa Core Z(DMG)
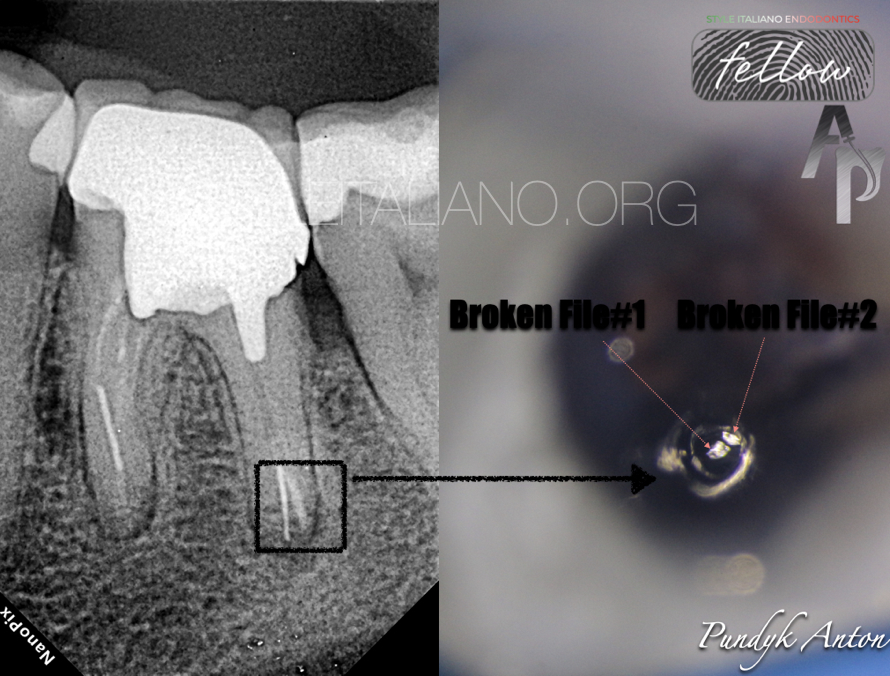
Fig. 7
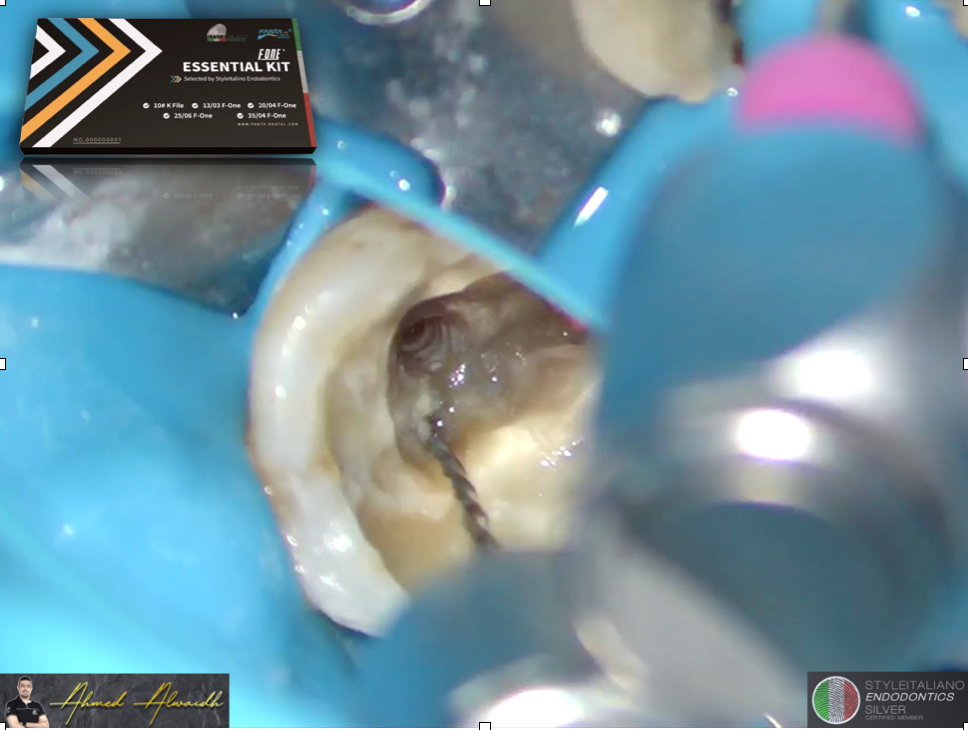
Treatment started from the distal root, the distal-lingual r/c was filled with glass ionomer cement. US tip E7(NSK) was used to remove the material and retrieve two broken files.
Extracted fragments were removed E11(NSK)+U-File#25(Mani).
Each step was executed with copious irrigation of hypochlorite
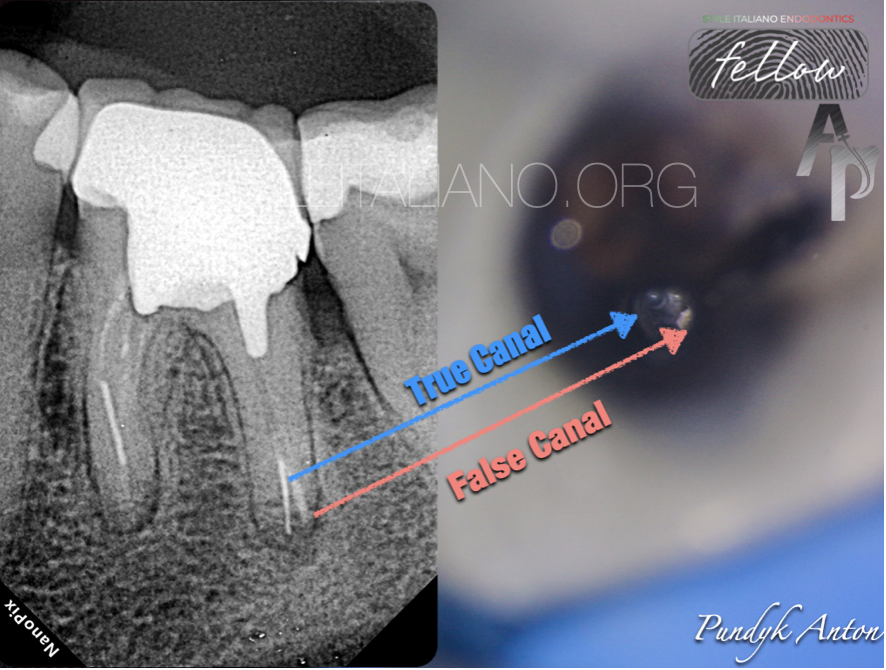
Fig. 8
View after removing both broken files.
In addition, the distal-buccal r/c had not been touched by the previous operator, and still some pulp was present.
The shaping evidenced the merging of disto buccal and disto lingual in the middle third of the root.
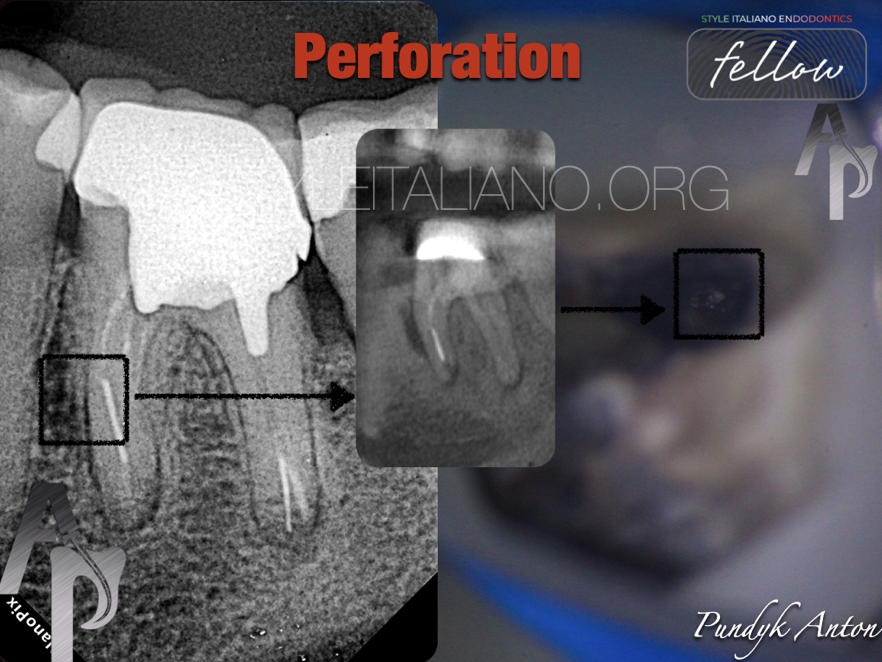
Fig. 9
Mesio-lingual r/c was passed without any problems, finishing of preparation - Vortex Blue(Perfect)45.04.
In the mesio-buccal root, the fractured instrument was retrieved by US with the same approach used in the distal root.
It was also possible to determine the location of the perforation.

Fig. 10
After dressing of calcium hydroxide, the perforation was cleaned-up by US tip & heated Sodium Hypochlorite, after that carefully dried with paper points. Surgispone-hemostatic sponge was used like matrix for protect from protrusion of material into the periodontal tissues.
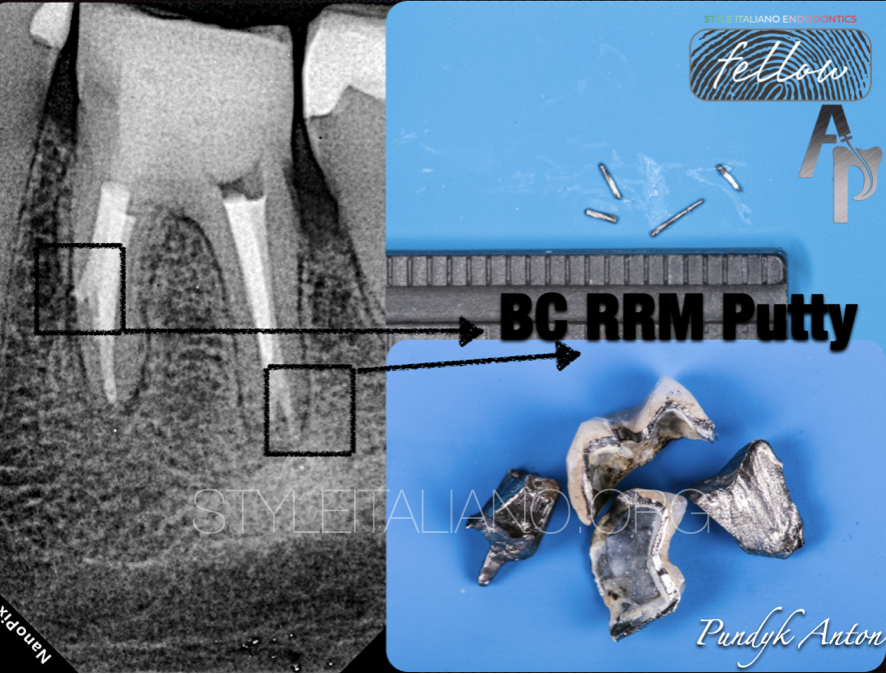
Fig. 11
Post-op

Fig. 12
Reinforcement was performed by Prosthetic Over Post size #1 (Over Fibers) and fixed by Luxa Core Z(DMG).PMMA’s crown was fixed by Ketac Cem Plus(Solventum)

Fig. 13
E.Max Press was fixed by VarioLink LC warm
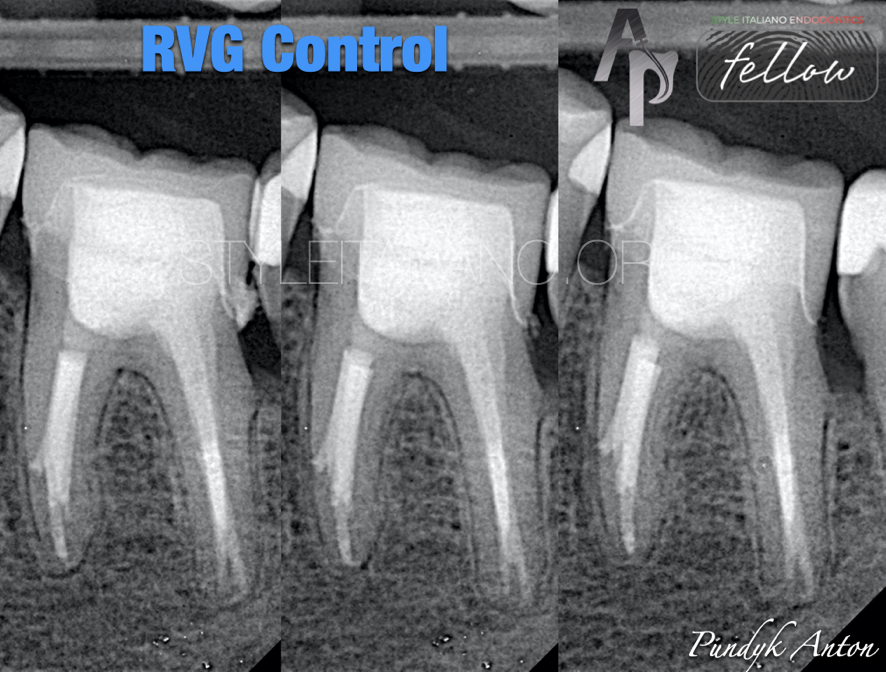
Fig. 14
Chronology of cement residues removal
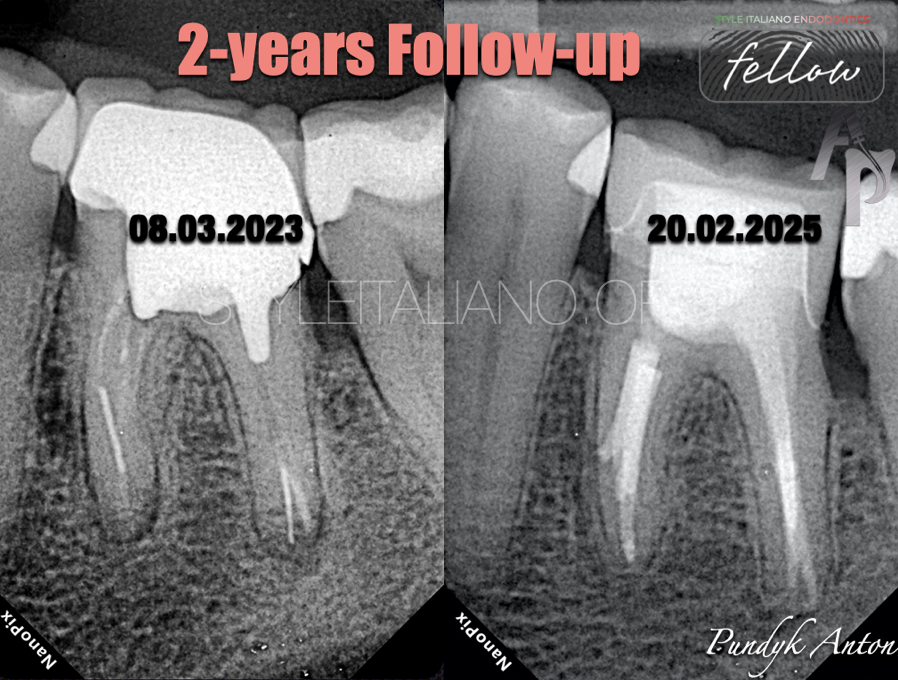
Fig. 15
Two years follow-up.

Fig. 16
About the author:
Dr. Anton Pundyk
I was born in 1984 in Tumen,Russia.I studied National Pirogov Memorial Medical University,Vinnitsa and graduated in 2008.I am an author articles regarding endodontics on Ukrainian dental magazine "DentArt" and using of the operating micropscope in everyday practice.Since 2017 I am working in private clinic in Vinnitsa,Ukraine.The main specialization is an endodontics,cad/cam and aesthetic dentistry.
In private life,I am enjoying my life with my family and my hobby is my work!
Conclusions
Magnification&illumination, ultrasound, knowledge of topographic anatomy of teeth, consistency in work, experience-this is an essential set of endodontist, necessary in the culture of modern endodontic treatment, the purpose of which is to preserve the wholeness and function of the tooth even in the most difficult clinical situations
Bibliography
1) Michael Hulsmann(1993) Endodontics&Dental Traumatology:Methods for removing metal obstructions from the root canal
2) FriedmanS.,Abitol S.,Lawrence H.P.(2003).Treatment outcome in endodontics:the Toronoto Study:initial treatment.Journal of Endodontics.29(12),787-793
3) Gorni Fabio(2006) The use of Ultrasound in Endodontics.ROOTS international magazine of endodontology 1(1):58-65