Non-Surgical Root Canal ReTreatment of Failed Apicoectomy with the Use of MTA cement
16/03/2024
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Teeth with previous apical resection and persistent apical periodontitis are usually re-treated surgically or with a combination of non-surgical and surgical re-treatment. Alternatively, nonsurgical orthograde treatment of failed apicoectomy can be performed using the apical barrier technique used for apical closure of nonvital teeth with apical resorption or immature nonvital teeth. Mineral trioxide aggregate (MTA) has become the material of choice in such cases due to its excellent biocompatibility, sealing ability, and osteoinductive properties.

Fig. 1
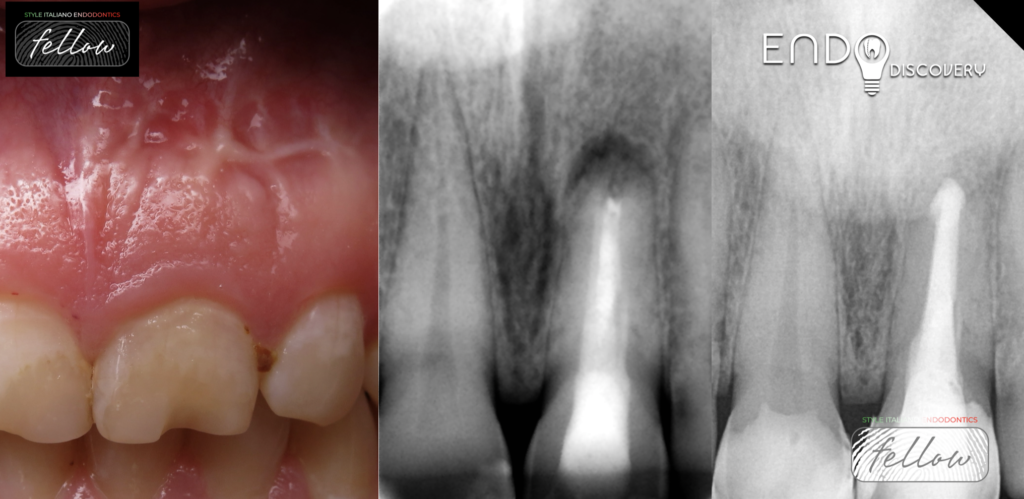
Initial Appearance
Referred
Patient S., 27 yo, 2.1 Asymptomatic Apical Periodontitis following failed Apicoectomy
A 27-year-old man came to dental office to repair a chipped left maxillary central incisor with a history of endodontic treatment and apicoectomy 4 years ago. Intraoral examination revealed tooth 2.1 with old chipped composite filling. Diagnostic radiograph showed radiolucent lesion in periapical area of 2.1. Percussion painless, periodontal probing within normal limits. Cone-beam computed tomography revealed periapical bone lesion, an oblique section of the root apex, buccal ledge in the middle third of the root canal. The treatment plan was the replace of the old composite filling and solve the endodontic problem. The patient rejected the idea of another surgery, so nonsurgical retreatment with the use of MTA apical plug was chosen.
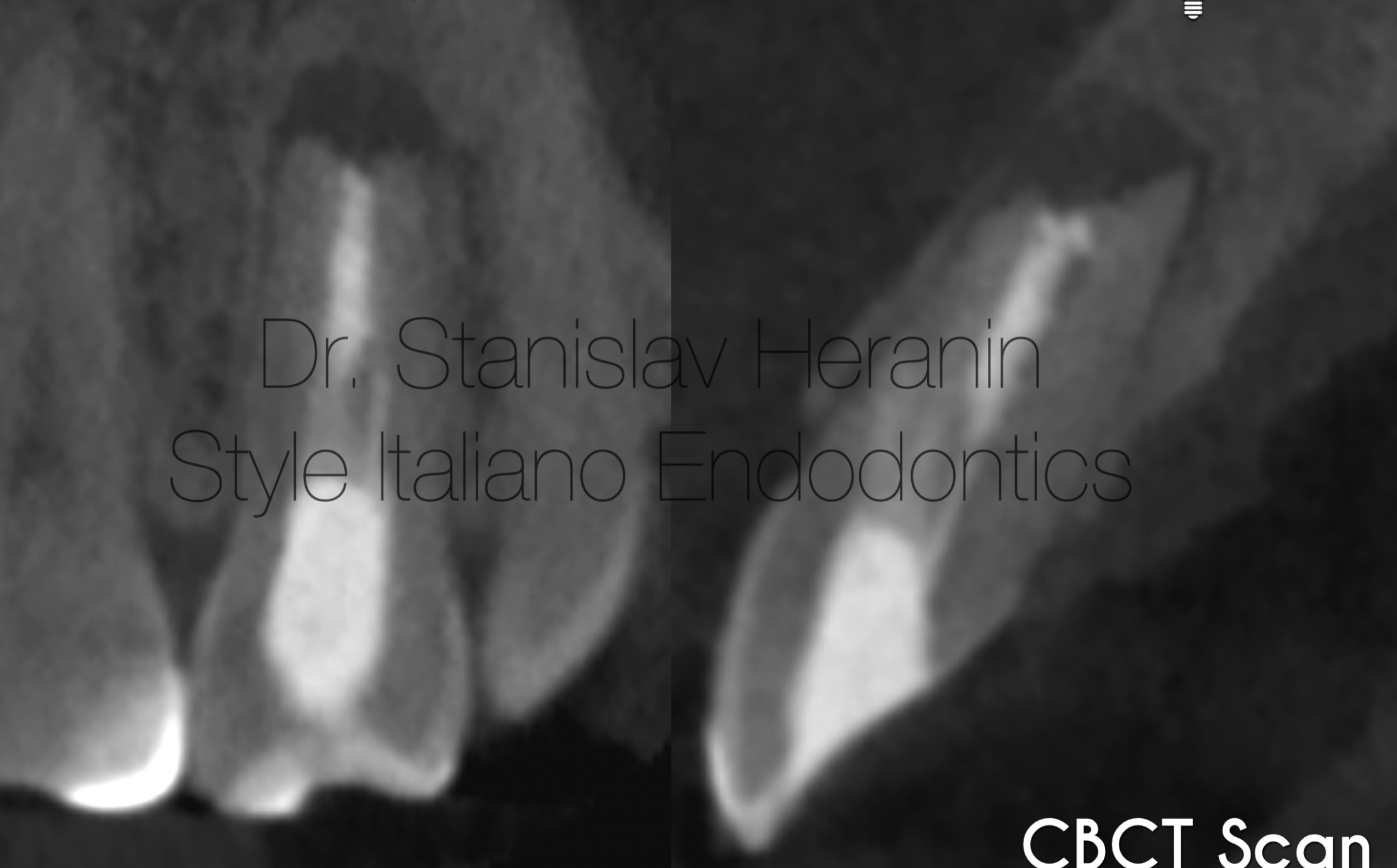
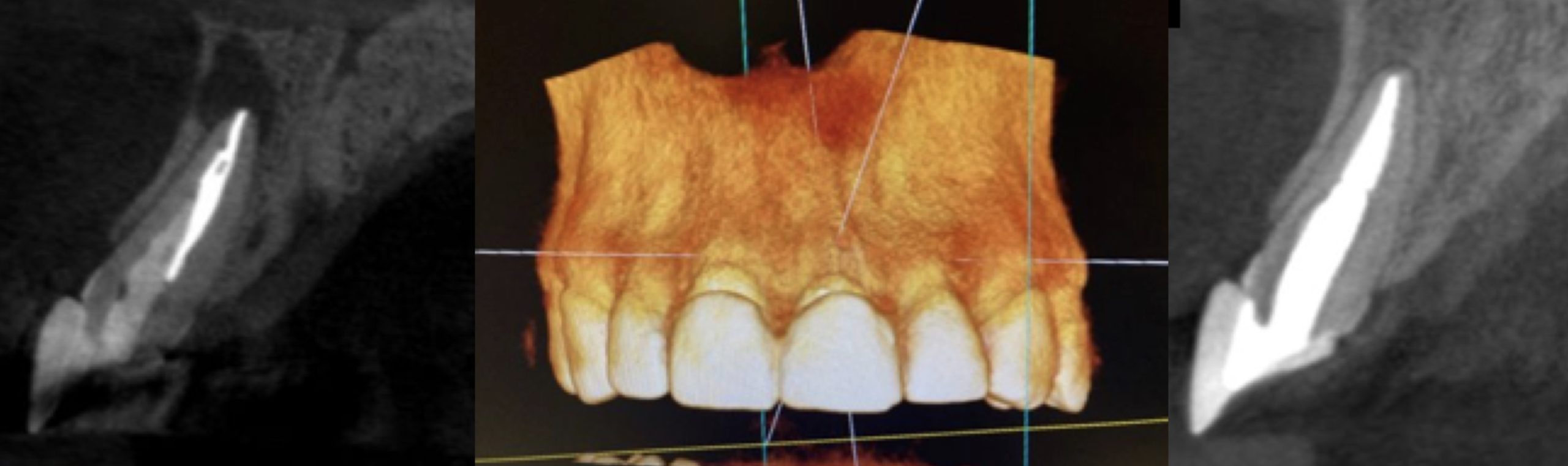
Fig. 2
Pre-operative CT scans show presence of
persistent periapical lesion and risk of root perforation

Fig. 3
Pre-operative CT scans show presence of
persistent periapical lesion and risk of root perforation

Fig. 4
1st app.
Initial access revealed a non-hermetic white cement-like material in the root canal, which was easily removed by ultrasonic tip. Buccal ledge complicated with perforation was found on the root surface. Multiple irrigation with 5.25% sodium hypochlorite solution with ultrasonic agitation, finished with calcium hydroxide dressing for 2 weeks.
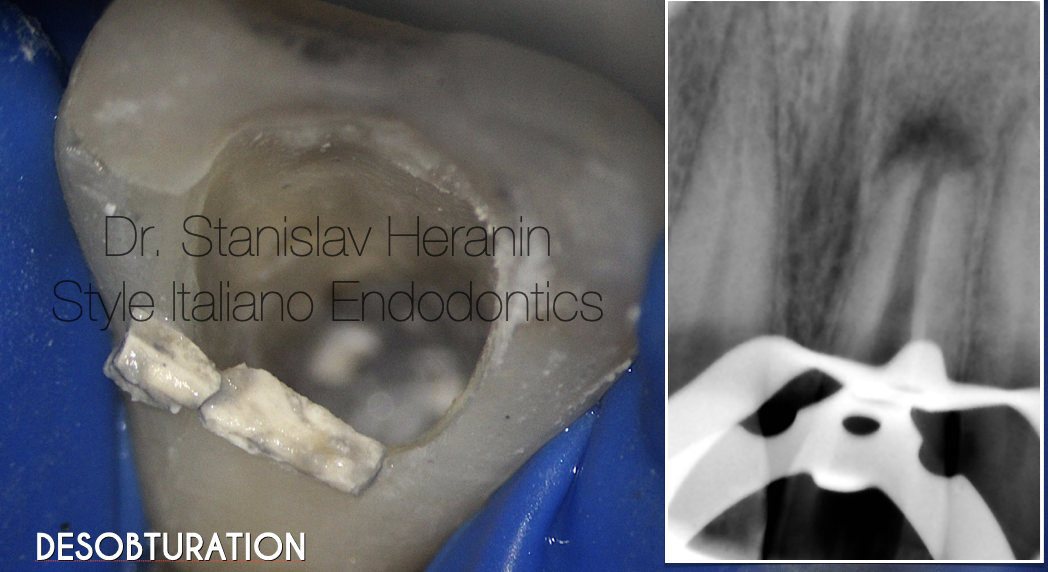
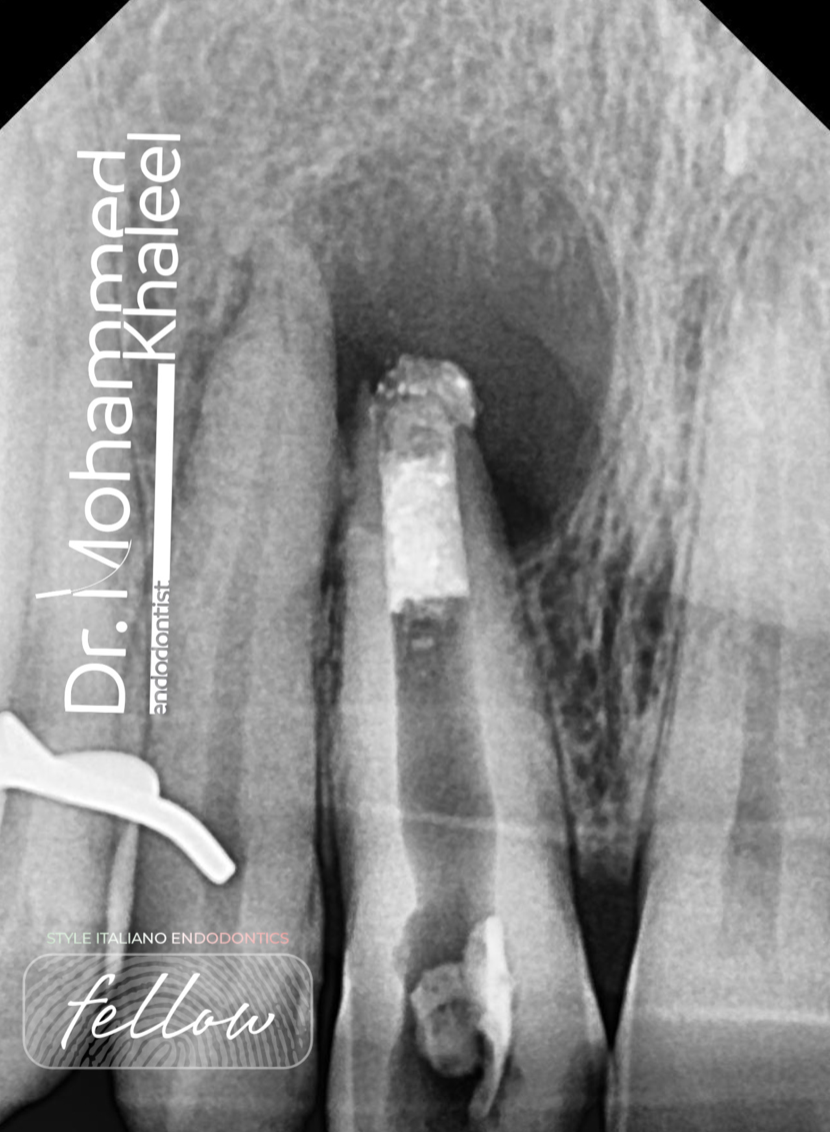
Fig. 5
Non-hermetic white cement-like material in the root canal
Desobturation radiographic control

Fig. 6
Initial access revealed a non-hermetic white cement-like material in the root canal, which was easily removed by ultrasonic tip. Buccal ledge complicated with perforation was found on the root surface. Multiple irrigation with 5.25% sodium hypochlorite solution with ultrasonic agitation, finished with calcium hydroxide dressing for 2 weeks.
Presence of Root canal perforation (buccal surface / middle third)
Undercutrs
Irregular apical area

Fig. 7
2.1 Asymptomatic.
Calcium hydroxide paste removed with US agitated 5.25% sodium hypochlorite. The final irrigation protocol consisted of alternate irrigation with 17% EDTA solution (exposure for 2 min.) and multiple irrigation with a 5.25% sodium hypochlorite solution with ultrasonic agitation. MTA plug was placed in the canal using a special syringe, including the perforation area followed by radiographic control.

Fig. 8
MTA plug

Fig. 9
Direct Restoration (Dr. Ksenia Lazareva)
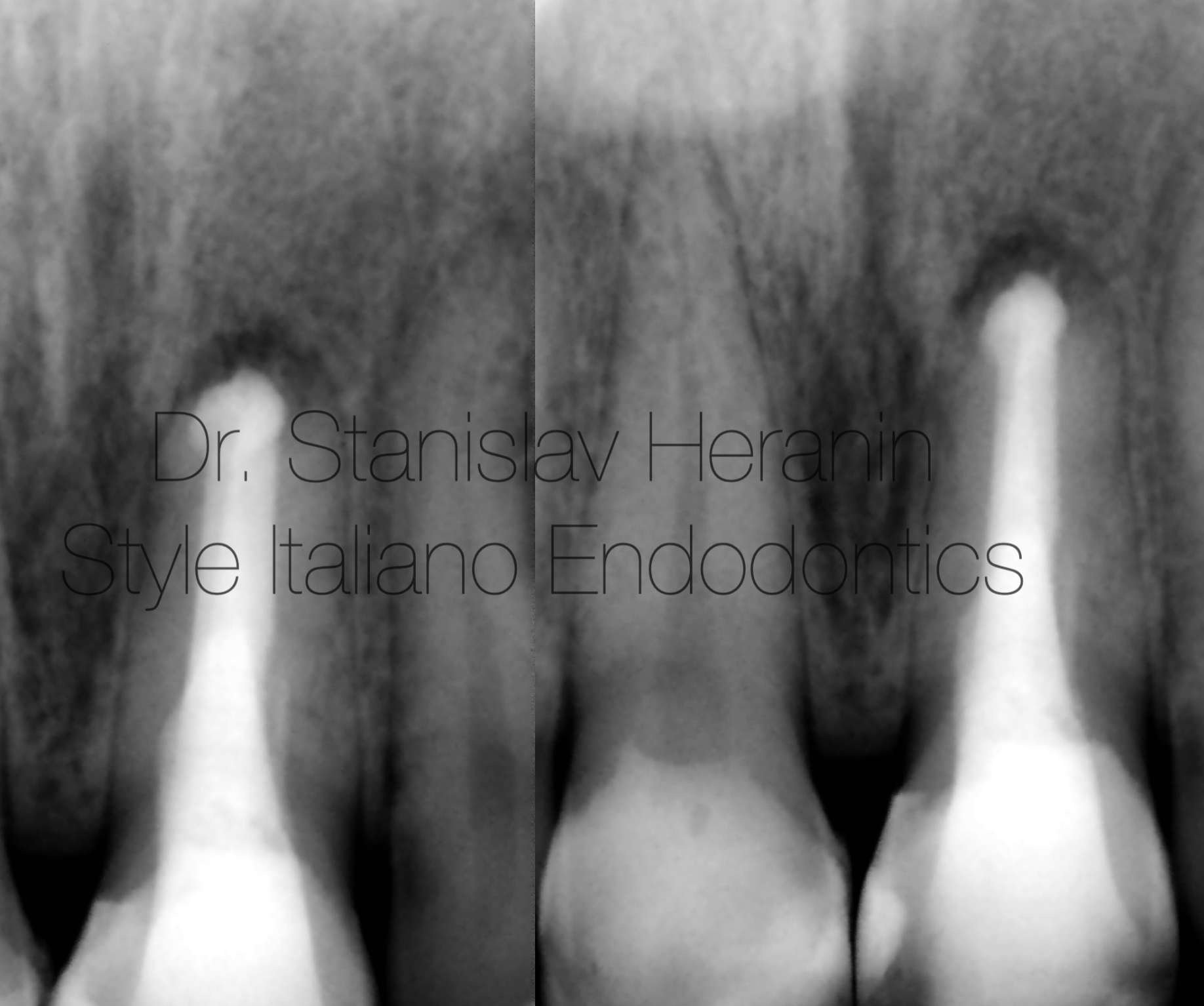
Fig. 10
4,5 m follow-up
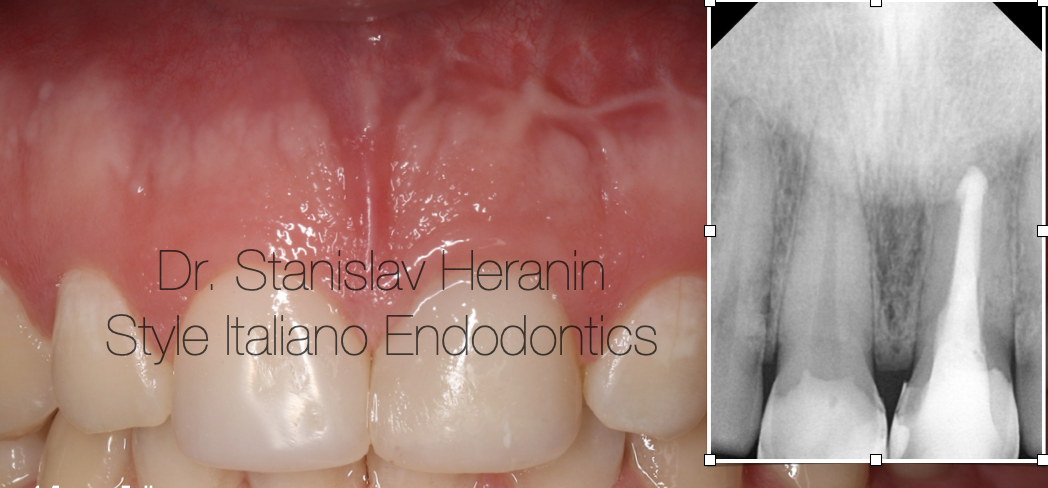
Fig. 11
1,5 year Follow-up
Direct Restoration appearance
Radiographic and CBCT follow-up revealed complete healing of the periapical lesion

Fig. 12
CBCT follow-up revealed complete healing of the periapical lesion
Fig. 13
CBCT follow-up revealed complete healing of the periapical lesion

Fig. 1
Conclusions
Hydraulic Calcium Silicate Cements (MTA / Bioceramics) used as an apical barrier can be a reliable and effective method for the non-surgical restoration of teeth with failed apicoectomy.
Bibliography
- Gorni FG, Gagliani MM. The outcome of endodontic retreatment: a 2-yr follow-up. J Endod. 2004 Jan;30(1):1-4. doi: 10.1097/00004770-200401000-00001. PMID: 14760899.
- Torabinejad M, Corr R, Handysides R, Shabahang S. Outcomes of nonsurgical retreatment and endodontic surgery: a systematic review. J Endod 2009;35:930–7
- Torabinejad M, Parirokh M, Dummer PMH. Mineral trioxide aggregate and other bioactive endodontic cements: an updated overview - part II: other clinical applications and complications. Int Endod J. 2018 Mar;51(3):284-317. doi: 10.1111/iej.12843. Epub 2017 Oct 11. PMID: 28846134.
- Castellucci A. The use of mineral trioxide aggregate in clinical and surgical endodontics. Dent Today. 2003 Mar;22(3):74-81. PMID: 12705015.
- Bogen G, Kuttler S. Mineral trioxide aggregate obturation: a review and case series. J Endod. 2009 Jun;35(6):777-90. doi: 10.1016/j.joen.2009.03.006. Epub 2009 Apr 22. PMID: 19482173.
- Brito-Junior M, Faria-e-Silva AL, Quintino AC, Moreira-Junior G, Geber M, Camilo CC, Soares JA. Orthograde retreatment failure with extruded MTA apical plug in a large periradicular lesion followed by surgical intervention: case report. Gen Dent. 2012 Mar-Apr;60(2):e96-100. PMID: 22414524.
- Stefopoulos S, Tzanetakis GN, Kontakiotis EG. Non-surgical retreatment of a failed apicoectomy without retrofilling using white mineral trioxide aggregate as an apical barrier. Braz Dent J. 2012;23(2):167-71. doi: 10.1590/s0103-64402012000200013. PMID: 22666776.