Non-Surgical Retreatment of Tooth 46 with Stripping Perforation: A Case Report
03/07/2025
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
This case details the non-surgical retreatment of tooth 46 in a 40-year-old female presenting with symptomatic apical periodontitis. Clinical and radiographic evaluation revealed a poorly adapted crown, metallic posts, secondary caries, and tenderness. During retreatment, four canals were located, and a stripping perforation was identified in the mesiolingual canal—an area predisposed due to root concavity and thin dentinal walls. The perforation was disinfected and sealed with MTA under magnification. Warm vertical compaction was used for obturation, followed by structural reinforcement and crown placement. One-year CBCT follow-up demonstrated periapical healing. Despite the guarded prognosis typically associated with such perforations, careful case management, timely intervention, and patient compliance contributed to a favourable outcome. This case highlights the importance of early detection, conservative handling of iatrogenic complications, and the critical role of coronal seal in long-term success.
A non-surgical endodontic retreatment was planned. The prosthetic crown and core were carefully removed to gain access. The two metal posts were removed using ultrasonic vibration under magnification. All coronal filling material and infected dentine were eliminated, allowing clear access to the root canal system.
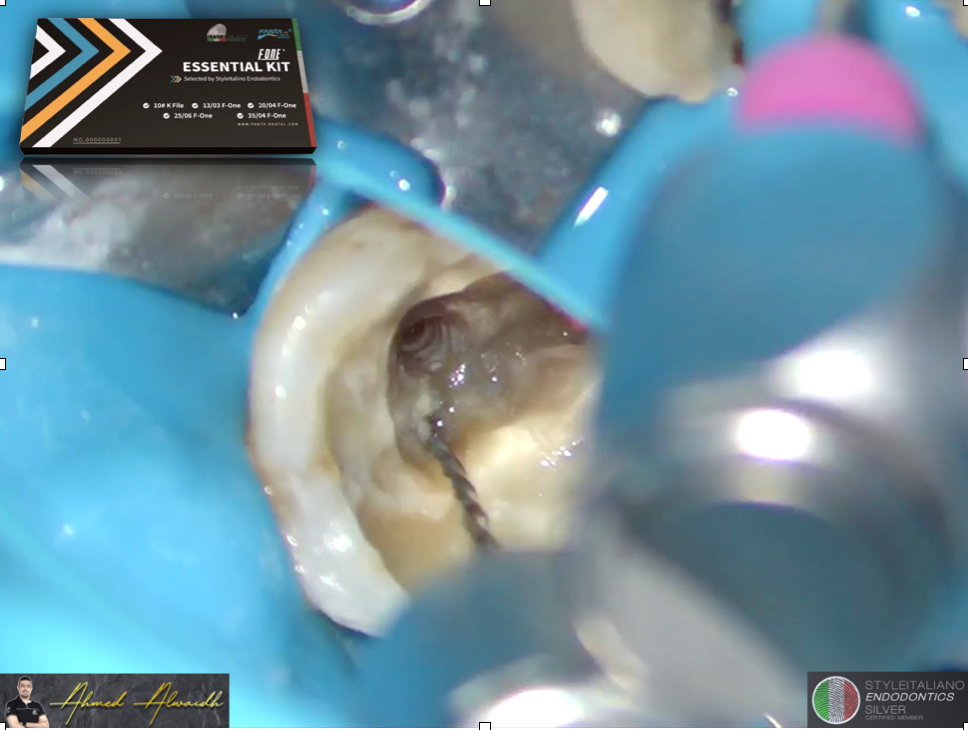
Four canals were identified. During exploration, a stripping perforation was noted in the mesiobuccal (MB) canal, a high-risk area due to the concavity of the root and the thinness of the dentinal wall. The perforation was managed conservatively with careful disinfection and obturation, avoiding extrusion of material beyond the canal.
Following cleaning and shaping, the canals were obturated to ideal working length using a warm vertical compaction technique with MTA for the perforation side. Secondary caries and structural compromise were addressed by complete removal of decay and reinforcement of the cavity with composite resin. The tooth was temporised out of occlusion.

Fig. 1
Initial situation after removing the crown

Fig. 2
Endodontic sequence and the immediate post-operative radiograph
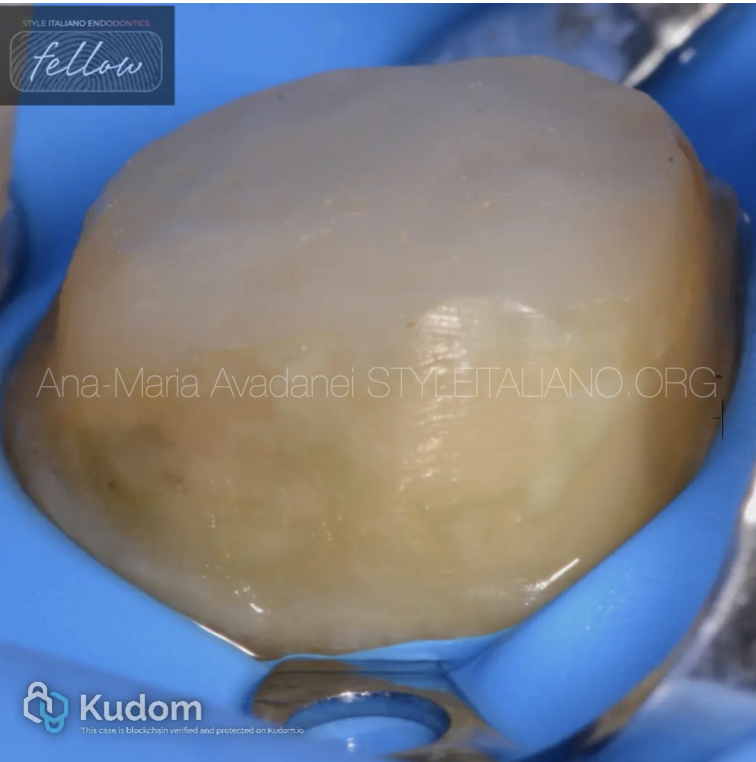
Fig. 3
Crown prepation
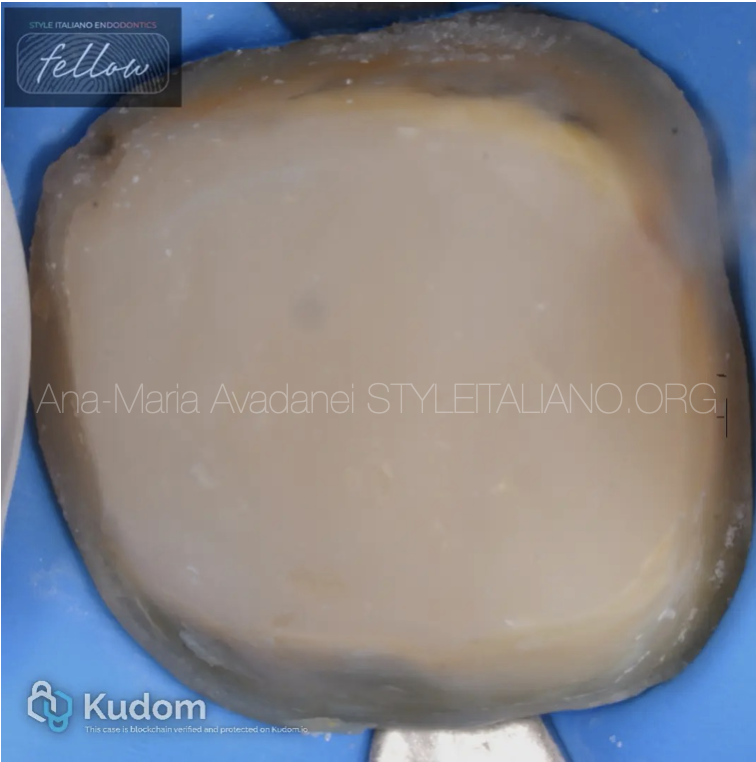
Fig. 4
Crown preparation

Fig. 5
Final crown

Fig. 6
Comparation of the initial CBCT and the CBCT at 1 year

Fig. 7
DDS, MSc Endodontics
-Graduated from the University of Medicine and Pharmacy "Grigore T. Popa," Romania.
- Worked in a practice limited to endodontics in Athens, Greece.
- Began her 3 years European Master’s Degree in Endodontics at UIC, Barcelona, while working as an endodontist in private clinics.
- Completed advanced training in Tepic, Mexico, specializing in complex surgical root canal re-treatments
-Currently working in various private clinics in London and Portsmouth, UK
Conclusions
The prognosis of non-surgical endodontic retreatment in the presence of a stripping perforation is generally considered guarded to favourable, depending on several clinical factors, including the size and location of the perforation, the time elapsed before repair, and the materials and techniques employed.
In this case, the perforation was detected and sealed during the retreatment procedure, the canal system was thoroughly disinfected and obturated to the correct working length, and a definitive coronal seal was established. The absence of periodontal communication, the patient’s commitment to follow-up and definitive restoration, and the overall restorable status of the tooth contribute to a favourable long-term outlook. The patient has also been appropriately informed of the potential for future complications and the need for surgical intervention or extraction if symptoms recur
Bibliography
Ng Y-L, Mann V, Gulabivala K. (2008). Outcome of secondary root canal treatment: a systematic review of the literature. Int Endod J, 41(12):1026–46.
Torabinejad M, Corr R, Handysides R, Shabahang S. (2009). Outcomes of non-surgical retreatment and endodontic surgery: a systematic review. J Endod, 5(7):930–7.
Tsesis I, Fuss Z, et al. (2010). Outcome of surgical endodontic treatment performed by a modern technique: A meta-analysis of literature. J Endod, 36(6), 982–987.
Pontius O, Hutter JW. (2002). Survival rate of perforated teeth treated with MTA: A retrospective cohort study. J Endod, 28(11), 683–685