MG3, Perfect Endo The BEST Sequence.
23/06/2022
Ibrahim El Naggar
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Shaping the root canal System is a stressful step in the Endodontic treatment , but with development of protocols , devices & files it’s no longer a headache to shape a canal , in this article we will go deep through Shaping Technique and the file metallurgy.
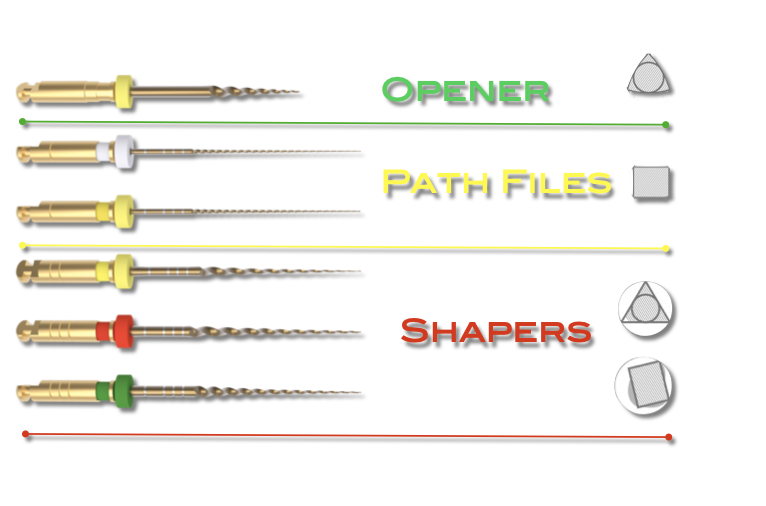
Fig. 1
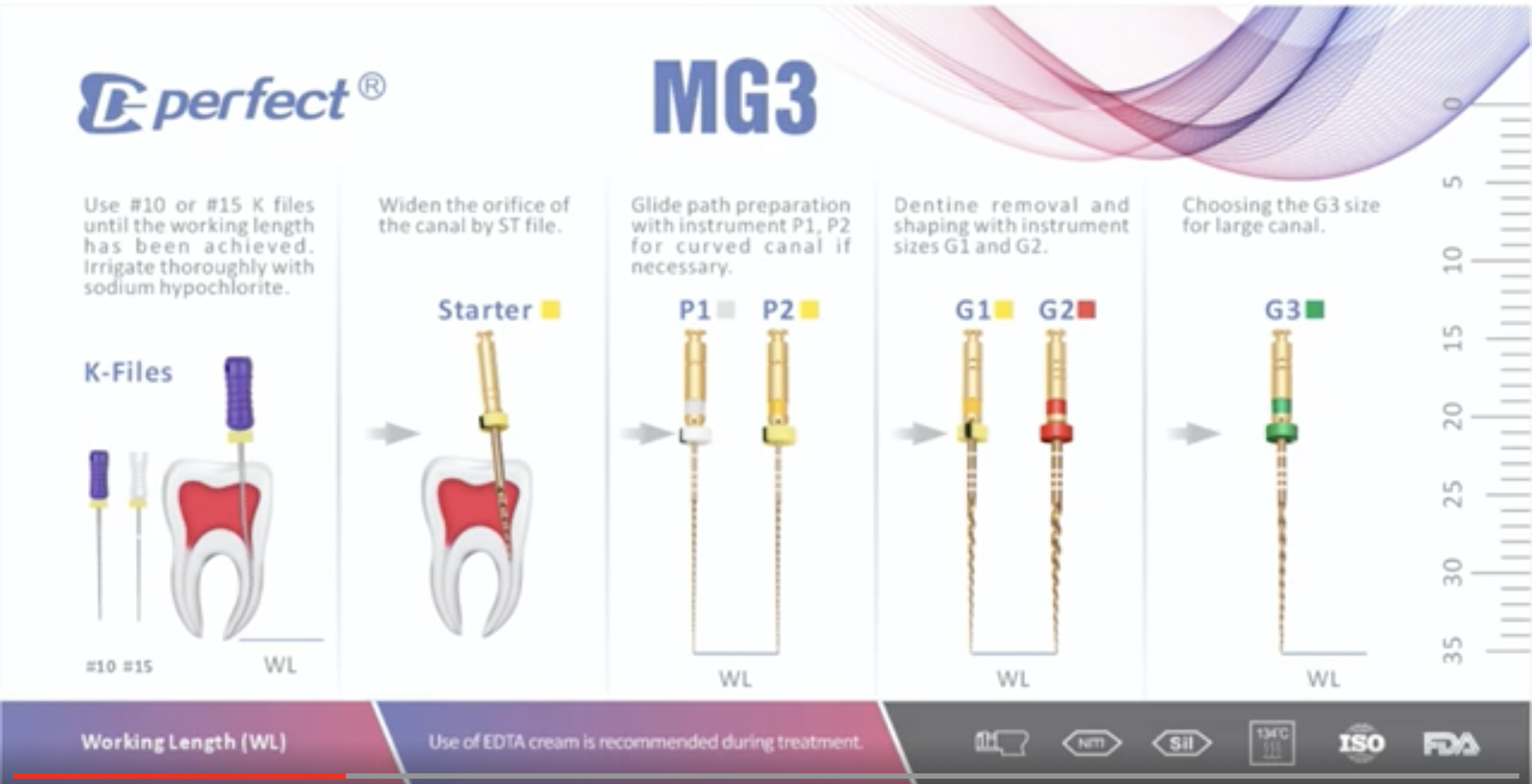
MG3 System comes in 6 files :
- Starter : Orifice Opener.
- P1 & P2 : Glide Path Files.
- G1 , G2 & G3 : Shapers.

Fig. 2
In the following slides we are going through the design of each file separately and also the Step Down shaping Technique.

Fig. 3
The design of the OPENER which resembles the orifice opener in the kit comes in triangular cross section for the optimization of the cutting efficiency and always with a brushing motion on the outer wall.

Fig. 4
The second 2 files are the gliders that come with the cross section of Square , they can be used sequentially in difficult cases or not in medium difficulty cases or we can skip them in simple cases , they are used in “Brushing ahead of Pecking” to avoid the tip separation or torsional stress due to small size.
Theses two files are designed to reach fully the working length.

Fig. 5
The 2 shaper files out of 3 with the size of 20/4 and 25/6 have a cross section of triangle for optimized cutting efficiency.
The 20/4 can be enough for small and tight canals and also curved canals thanks to the size and cross section for the added flexibility.
In case of large canal the 25/6 can be the final file of use and it can be also used for the flaring of the coronal 2/3 in the step down preparation.

Fig. 6
The largest file in the kit comes with the size of 35/4 and it”s used for large canals like palatal and central , that’s why it came with the offset cross section to optimize the contact with the canal wall “swaggering”

Fig. 7
Diagram for showing the possible filling sequence for simple cases.

Fig. 8
Diagram for showing the possible filling sequence for hard cases.
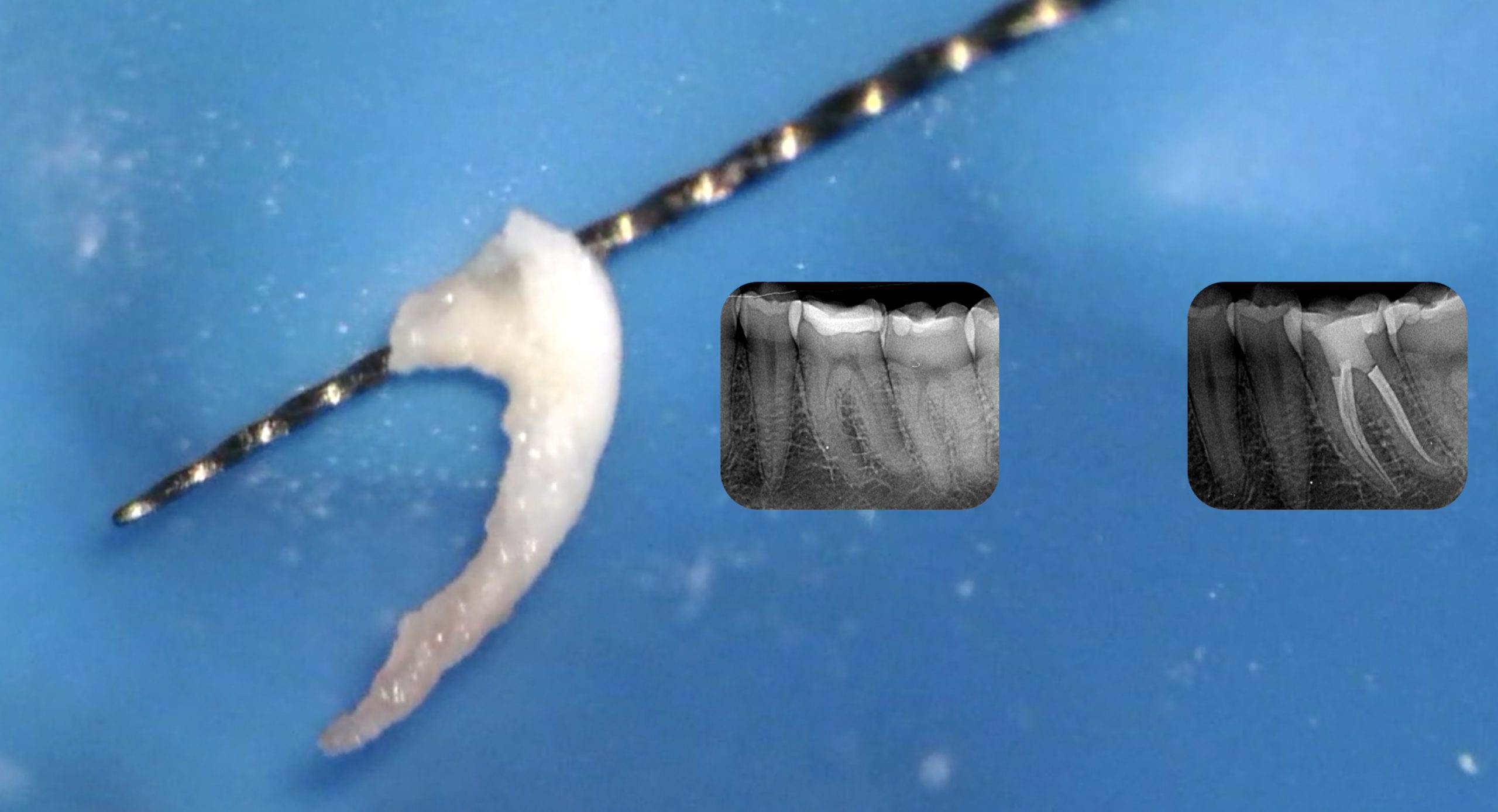
clinical video
Conclusions
The clinician must know the prosperities , advantages & disadvantages of every rotary system to be able to apply his knowledge in different clinical scenarios.
Bibliography
1. Endodontic Facts, American Association of Endodontists. Available at: http://www. aae.org/about-aae/news-room/endodontic-facts.aspx. Accessed June 1, 2015.
2. Borges AH, Bandeca MC, Tonetto MR, et al. Portland cement use in dental root perforations: a long term followup. Case Rep Dent 2014;2014:637693.
3. TsesisI,FussZV.Diagnosisandtreatmentofaccidentalrootperforations.Endodontic Topics 2006;13:95–107.
4. Tsesis I, Rosenberg E, Faivishevsky V, et al. Prevalence and associated periodontal status of teeth with root perforation: a retrospective study of 2,002 patients’ medical records. J Endod 2010;36:797–800.
5. Gorni FG, Gagliani MM. The outcome of endodontic retreatment: a 2-yr follow-up. J Endod 2004;30:1–4.
6. Clauder T, Shin S-J. Repair of perforations with MTA: clinical applications and mechanisms of action. Endodontic Topics 2006;15:32–55.
7. Kvinnsland I, Oswald RJ, Halse A, Gronningsaeter AG. A clinical and roentgenological study of 55 cases of root perforation. Int Endod J 1989;22:75–84.