MG3 Blue , Long Rooted Molar
23/12/2022
Ibrahim El Naggar
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
In this article we are introducing the MG3 Blue Files for the treatment of Long Mandibular Molar and how the system combines the function of Cutting Efficiency & Flexibility to facilitate the shaping sequence.

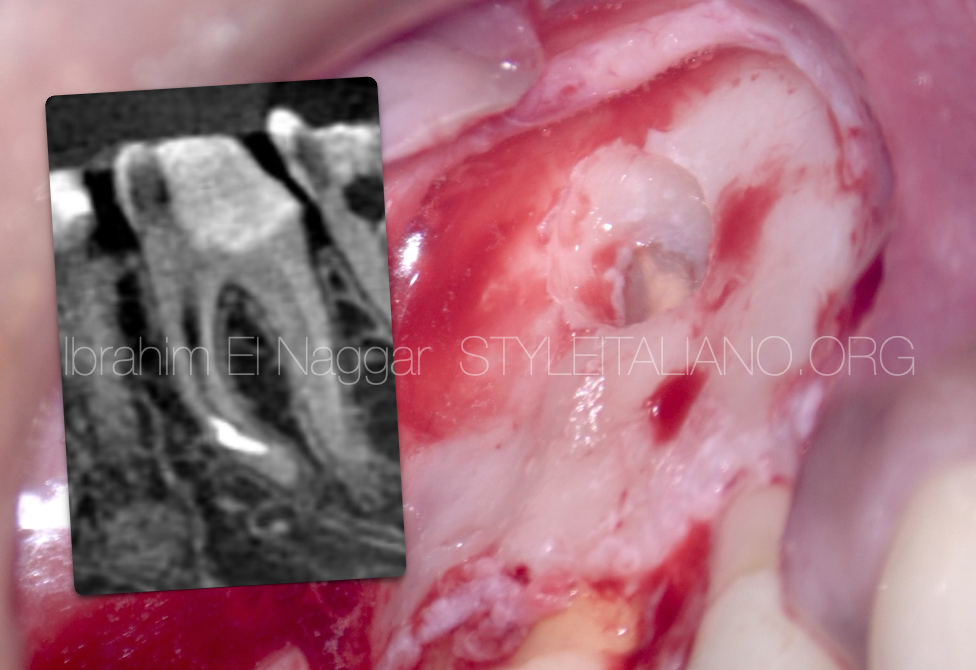
Fig. 1
Pre - Op Radiograph , Long Rooted Molar with Coronal Interference in the coronal part of the Mesial System.
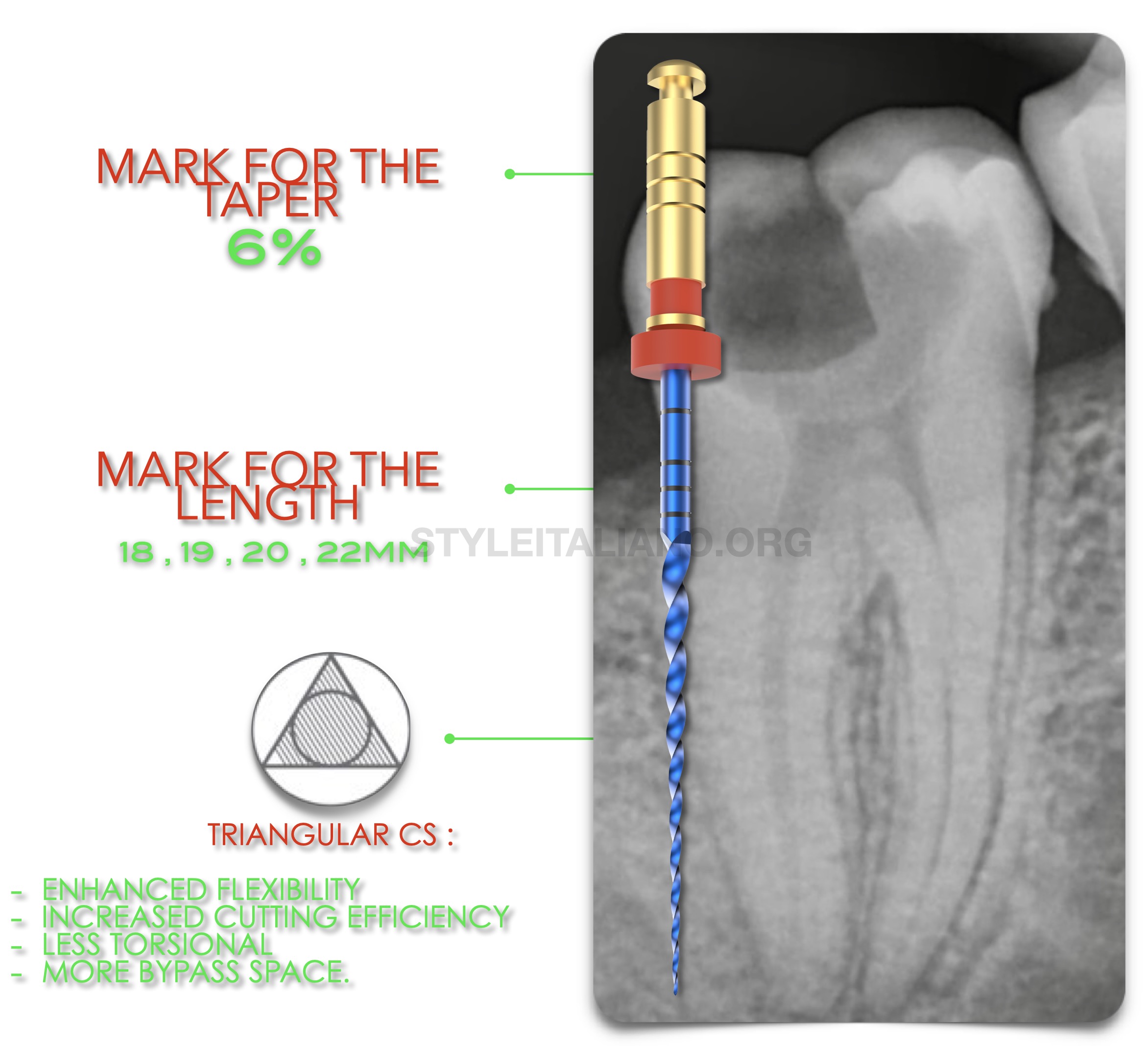
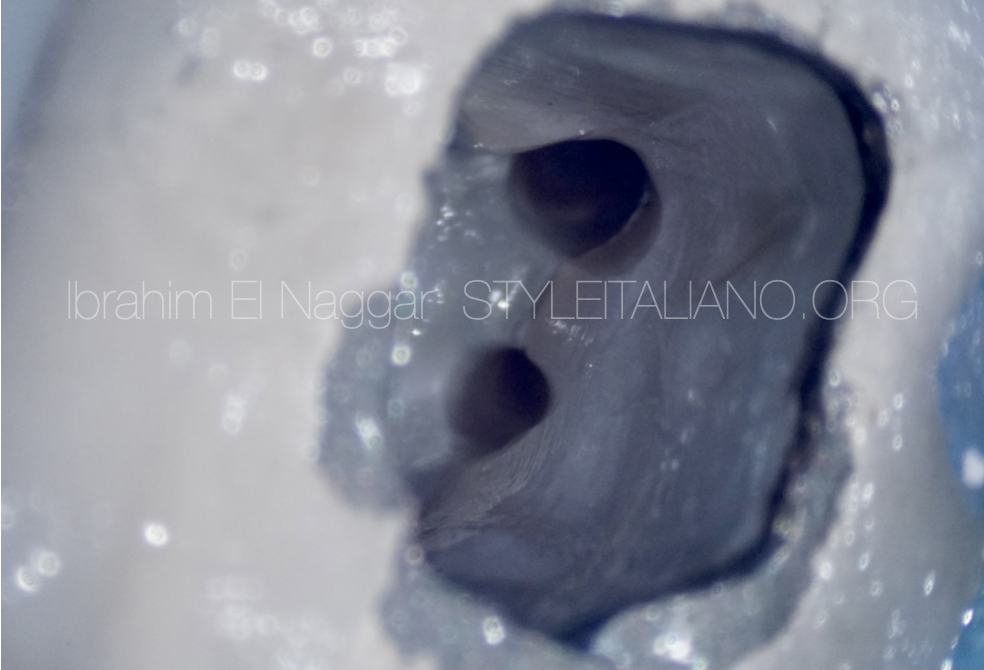
Fig. 2
In the distal Canal we can see that its a large canal , that’s why we can take the advantage of the instrument taper especially the G2 which 25 6% taper to do the flaring and shaping in the same step , also we can shape the canal manulless by using the dual function in the Motor to minimize the number of files and maximize the efficacy.
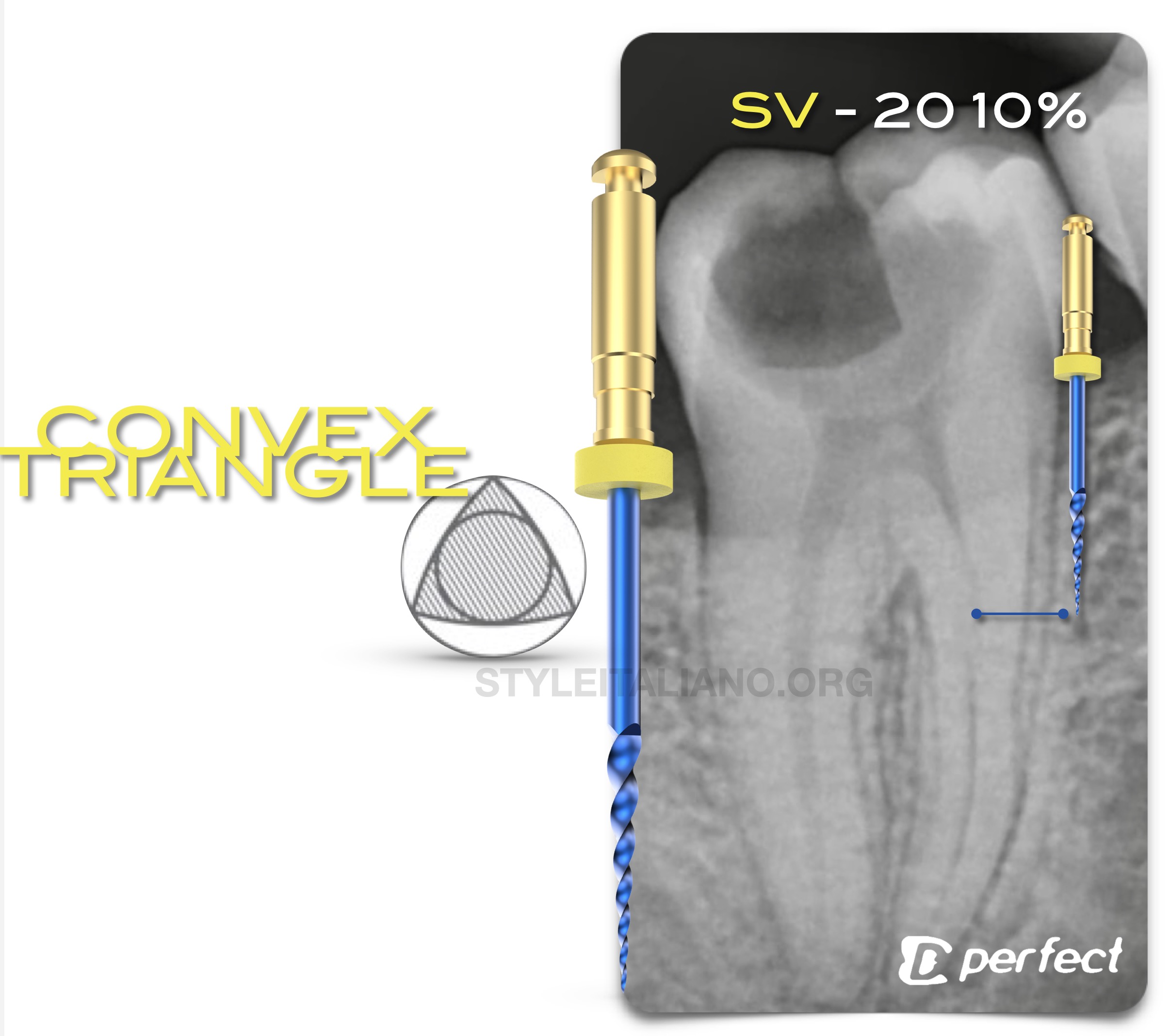
Fig. 3
In the mesial system to unlock the coronal interference we will start mechanical preflaring using the opener which is 20 10% taper and comes in a convex triangle Design which gives the file the needed flexibility beside the cutting efficiency.
The file will be used in the coronal segment with a brushing movement on the outer wall.
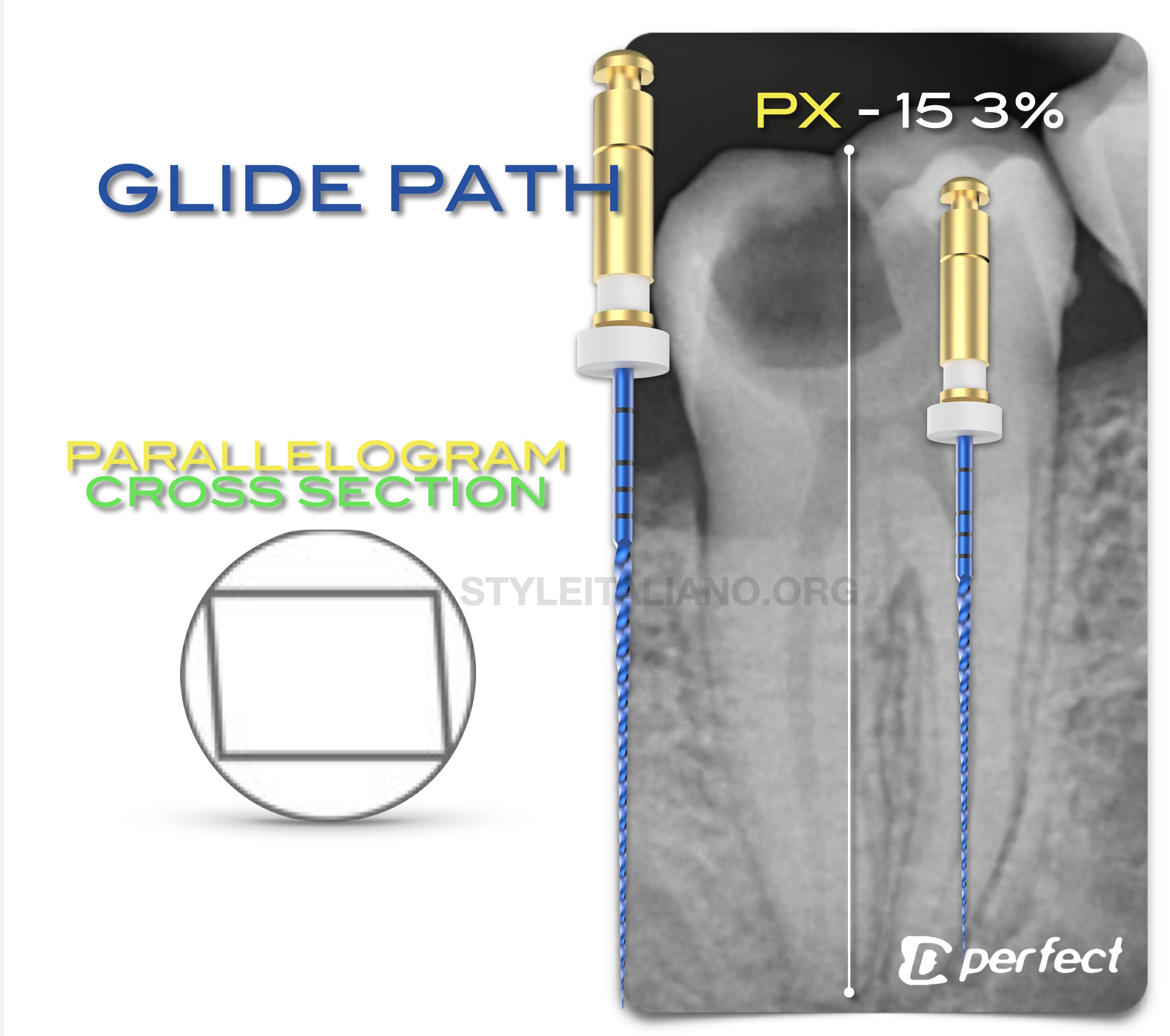
Fig. 4
After the mechanical flaring the we are proceeding to the Glide Path Management.
The file of choice will be the navigator which have the features of the martensitic alloy , that makes the file have a high cyclic fatigue resistance and the small mass and taper doesn't allow any unfavorable action of the file like zipping or transportation , lastly the cross section which is PARALLELOGRAM makes the contact between the file and the canal less with move space for Debris evacuation coronally.
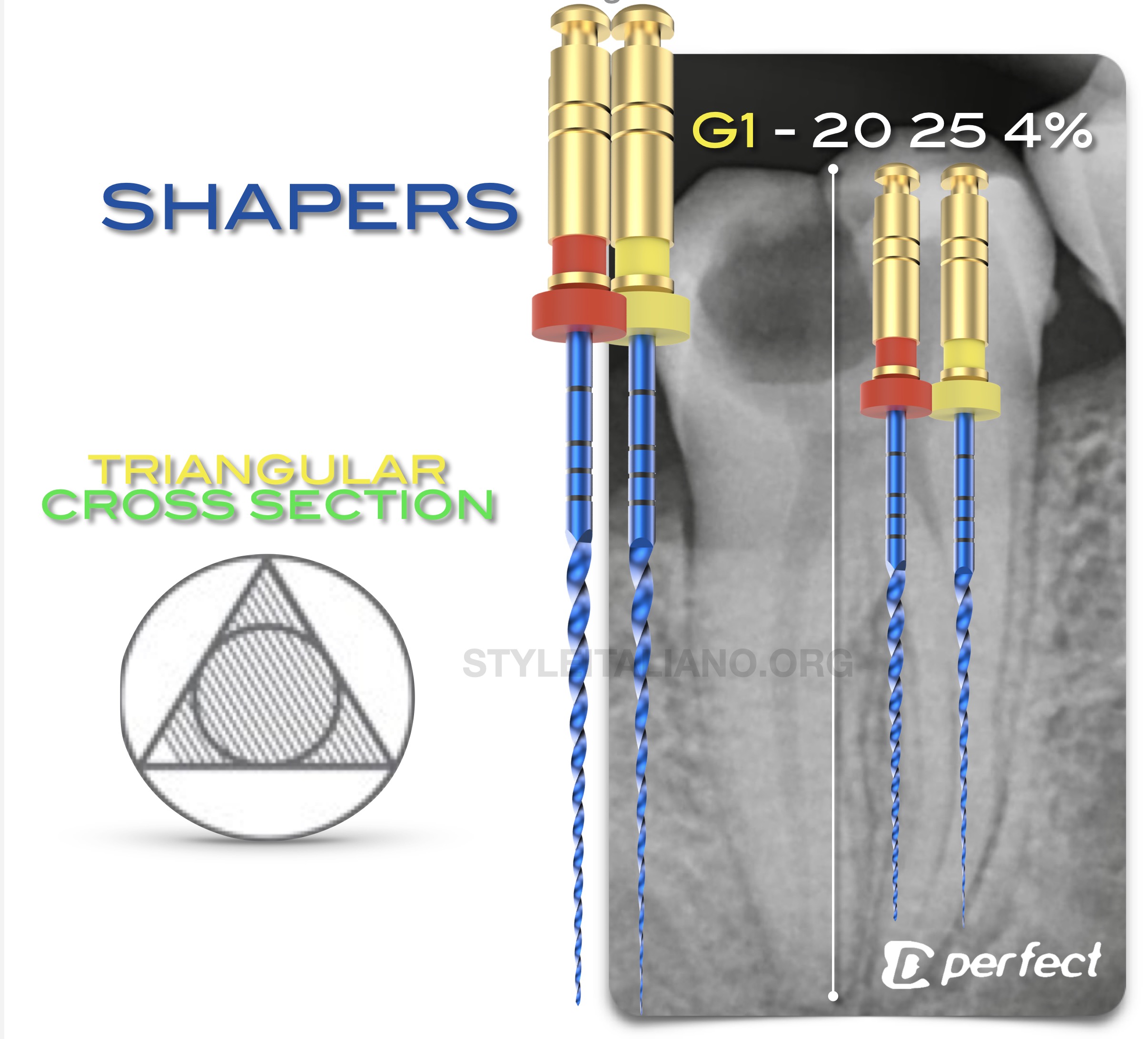
Fig. 5
After the Glide path , the space is now ready for the Shaper G1 ,G2 which is 20 25 4% , the grater benefit of this file is the cross section when it is been combined with the small mass and taper which will aid in shaping of the difficult anatomies , tight canals and also the splits the cross section gives enhanced features for the flexibility and and cutting efficiency.

Fig. 6
Master Cone X Ray

Fig. 7
POST OP
Clinical Video
Conclusions
The Clinician must have a knowledge about files , kinematics & metallurgy and to choose the best set for every situation , MG3 files and MG3 Blue offers a files for a wide range of Cases and different situation.
Bibliography
1. Endodontic Facts, American Association of Endodontists. Available at: http://www. aae.org/about-aae/news-room/endodontic-facts.aspx. Accessed June 1, 2015.
2. Borges AH, Bandeca MC, Tonetto MR, et al. Portland cement use in dental root perforations: a long term followup. Case Rep Dent 2014;2014:637693.
3. TsesisI,FussZV.Diagnosisandtreatmentofaccidentalrootperforations.Endodontic Topics 2006;13:95–107.
4. Tsesis I, Rosenberg E, Faivishevsky V, et al. Prevalence and associated periodontal status of teeth with root perforation: a retrospective study of 2,002 patients’ medical records. J Endod 2010;36:797–800.
5. Gorni FG, Gagliani MM. The outcome of endodontic retreatment: a 2-yr follow-up. J Endod 2004;30:1–4.
6. Clauder T, Shin S-J. Repair of perforations with MTA: clinical applications and mechanisms of action. Endodontic Topics 2006;15:32–55.
7. Kvinnsland I, Oswald RJ, Halse A, Gronningsaeter AG. A clinical and roentgenological study of 55 cases of root perforation. Int Endod J 1989;22:75–84.