
Mechanical Management of Calcified & Curved Apical Third of Upper Premolar
19/04/2021
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Calcified Canals always represent a challenge in root canal treatment, specially when the calcified canal is curved (either moderate or severe curvature).
Once the case is identified as a calcified one, either at apical third or the whole length of the canal, we should bear in mind that dealing with such cases requires lots of tools and skills. Tools include Magnification, Manual files (stainless steel or carbon steel), Nickel Titanium files with small tip sizes and taper and heavy irrigation all the time.
Magnification is important but, when it comes to calcified apical third, it has less use and mainly depends on the skills of the operator and the files used.
This case report shows how to manage apical third calcifications easily using nickel titanium files only and not using any manual files, while preserving the curvature of the canal.

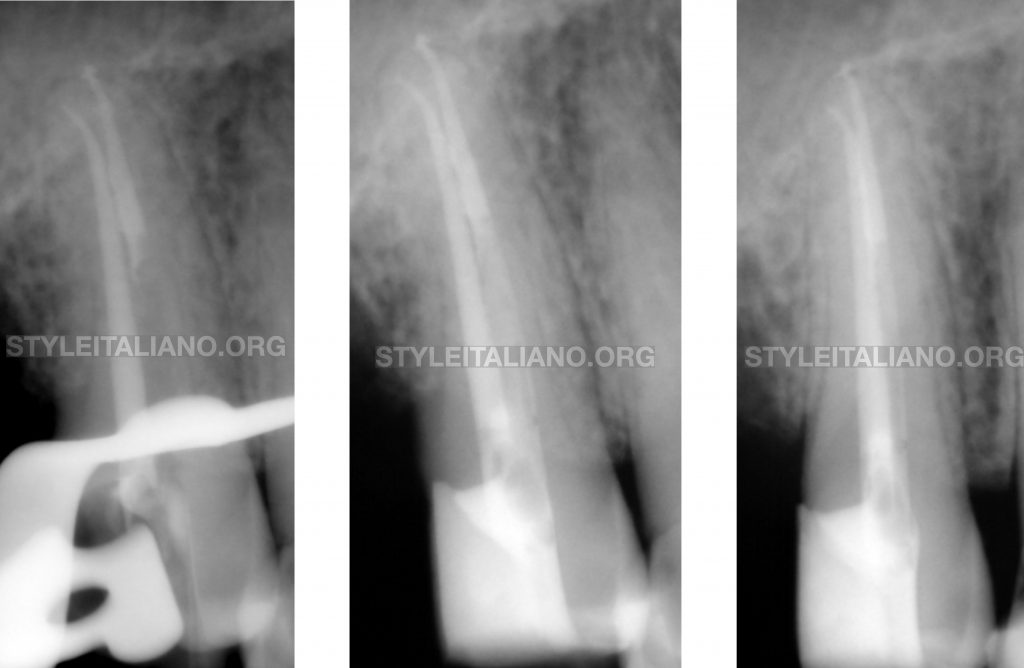
Fig. 1
A 35-years-old male came to our dental clinic complaining of pain related to the upper right second premolar.
This Premolar shows distal caries and, after thorough clinical & radiographic examination, it was diagnosed as SIP/SAP.
We decided to go for RCT immediately but we had a challenge of having a calcified apical third as shown in the Pre-operative radiograph
All the steps were done under dental operating microscope using the most advanced techniques in all the steps of RCT.
Removal of the Caries was done. Then, the Access Cavity was done and refined using Ultrasonics.
The key now was do proper coronal flaring in order to achieve better accessibility to the Apical third of the canal and gain nearly straight access to that complex anatomy.
Coronal flaring was done using the Starter file #20/10 in MG3 Kit (Shenzhen Perfect Medical Instruments Co).
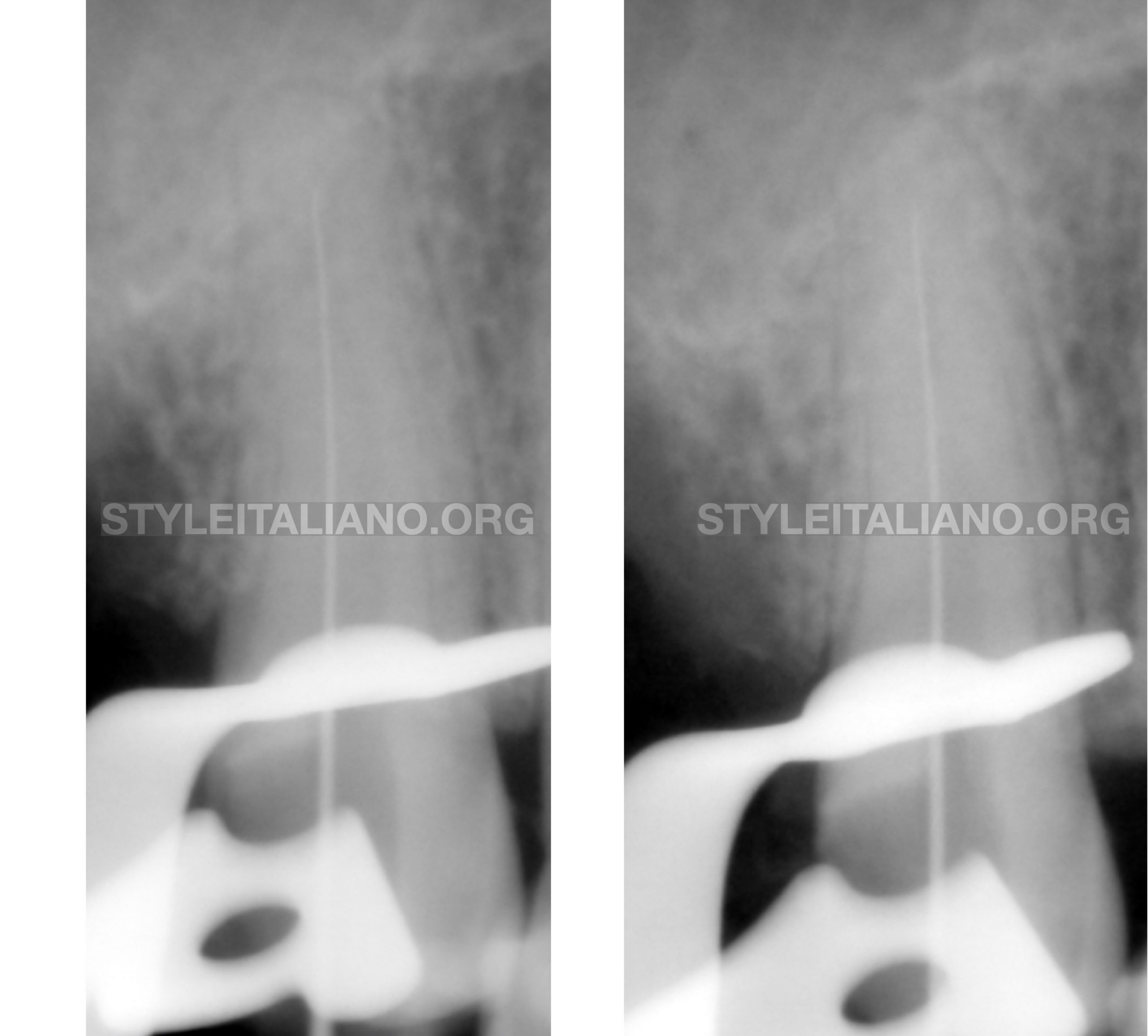
Fig. 2
After Coronal flaring, radiograph was taken with #10 K file in the B & P to ensure the Straight line access to the Apical third of both Canals, confirming also the calcified anatomy apically
After gaining the Straight Access to the apical third, I decided to use the P2 file #19/2 (MG3 Kit) directly to the apical third in order to manage this calcification.
I preferred to use this file in particular as it has a tip size #19 and standardized taper of 2%, so it will provide the required flexibility with the perfect moderate tip size.
The P2 file could manage to negotiate these canals easily while preserving the curvature of the buccal canal.
After Working Length determination using EAL, The Biomechanical Preparation was done using Controlled Memory Rotary files of the MG3 Kit up to the working length. G1 in action
G2 of size 25/06. This size would enable proper disinfection either by syringe & needle or any other irrigation activation method.
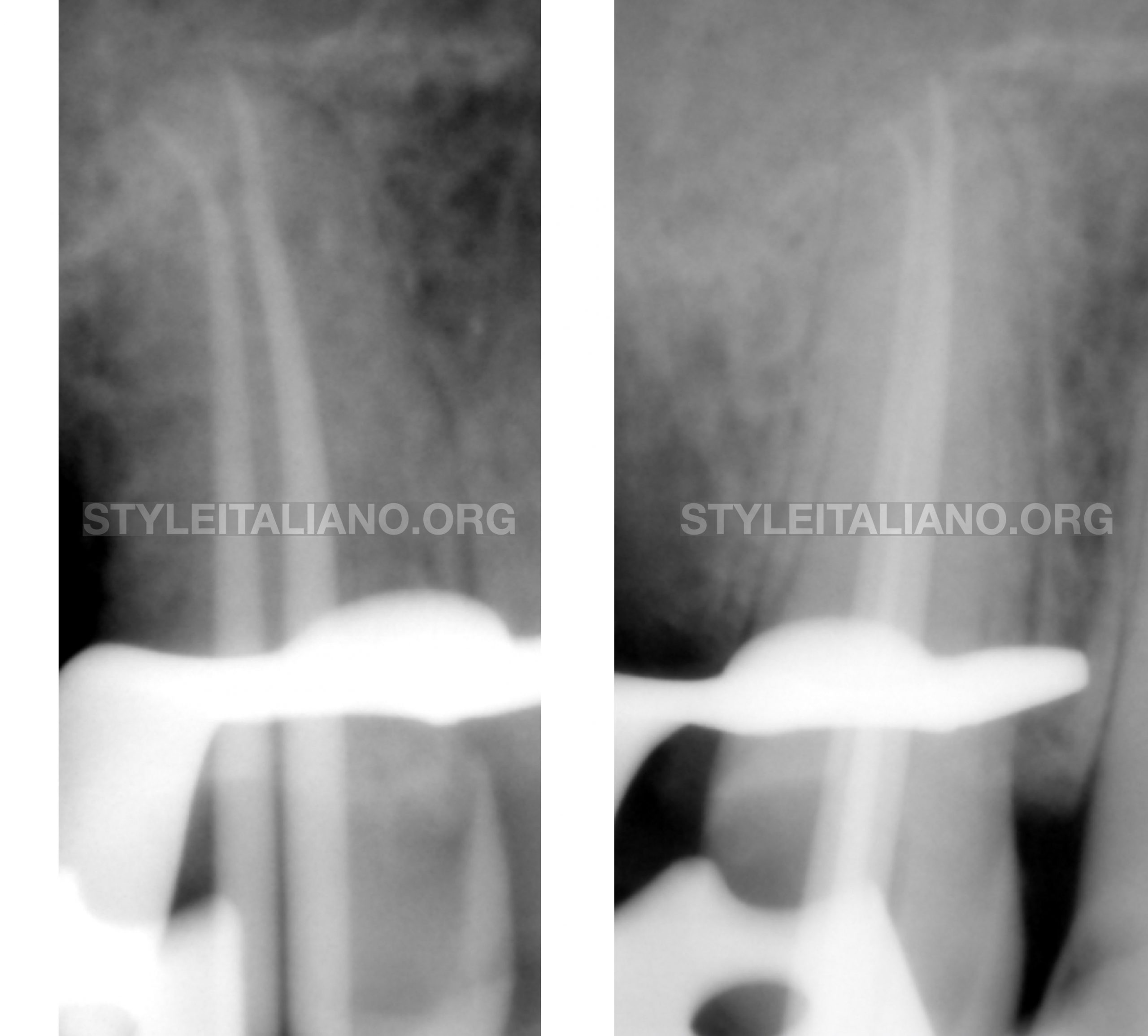
Fig. 3
The intra operative radiograph was taken with master cones of the same size as the MAF, up to the working length, as shown in figure
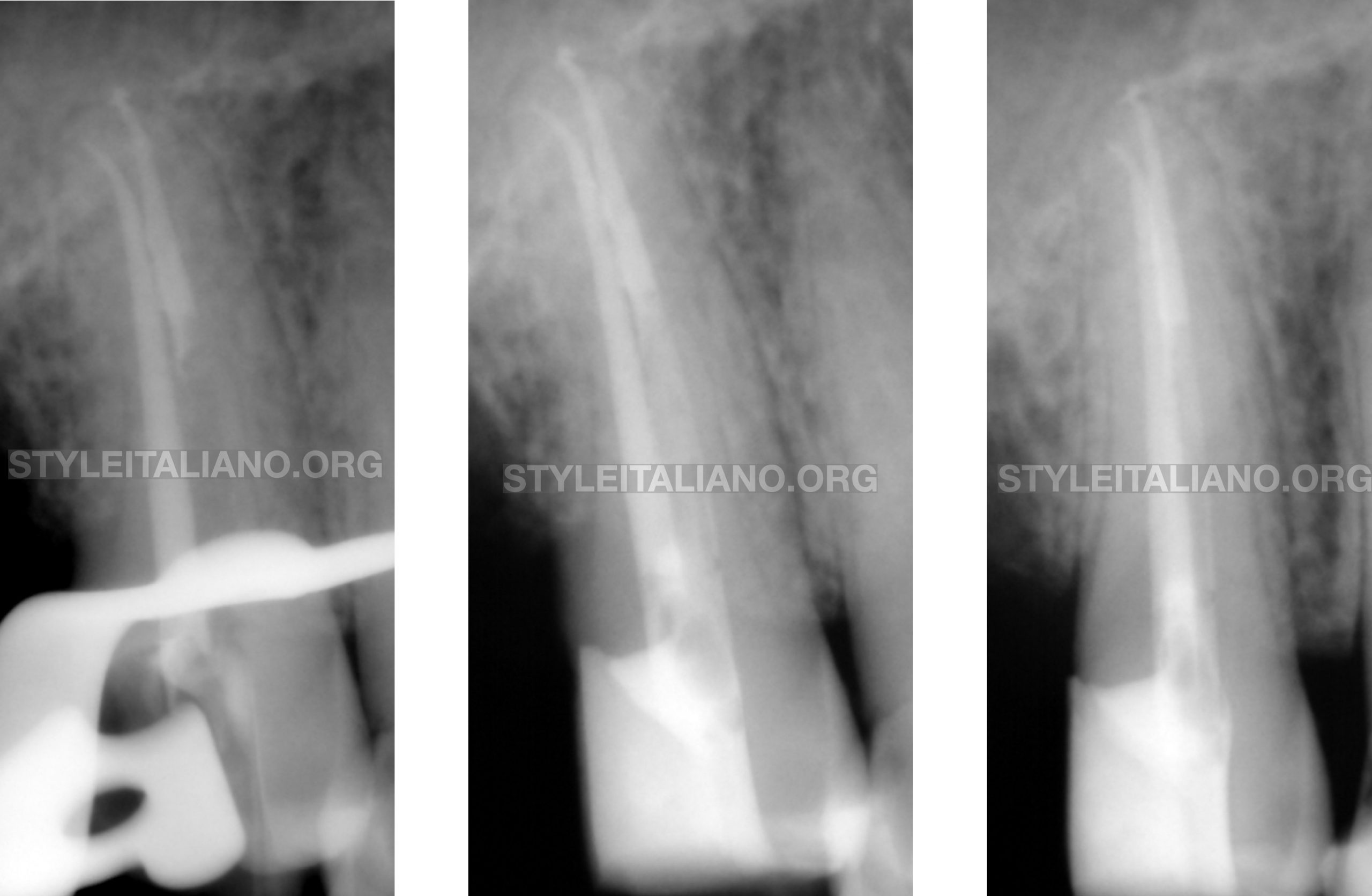
Fig. 4
Obturation was done using Synchronized Hydraulic Condensation technique using BioCeramic sealer and the master cone only in the Buccal Canal.
While, the palatal canal was obturated using CWC technique with Resin Sealer in order to Create a post space.
Post Placement with Composite Core restoration was done in the same visit to provide good coronal seal.
The Case was done as single visit RCT and referred immediately to the prosthodontist.
Conclusions
This clinical case showed us that managing of apical calcifications could be achieved mechanically if the right instruments are used. This could be done in particular cases where rotary files tend to negotiate the canals from the first time, and if not, shifting to manual files is mandatory to decrease iatrogenic errors.
MAF is chosen according to each case where the most important issue is to provide better disinfection of the root canal system.
Bibliography
- Anil Kishen et al, 2015. “Contracted endodontic cavities: the foundation for less invasive alternatives in the management of apical periodontitis”. Endodontic Topics.
- Lee et al, 2019. “Influence of apical preparation size and irrigation technique on root canal debridement: a histological analysis of round and oval root canals”. International Endodontic Journal.
- Kulild et al, 2014. “Master apical file size – smaller or larger: a systematic review of healing outcomes”. International Endodontic Journal.
- Ove A Peters, 2004. “Current challenges and concepts in the preparation of root canal systems: a review”. JOE
- Vertucci FJ, 2005. “Root canal morphology and its relationship to endodontic procedures”. Endodontic Topics.