

Management of separated instrument: retrieve, bypass or leave it
10/05/2025
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
The management of a broken file refers to handling situations where an instrument, typically a file, breaks or separates during the process of cleaning and shaping the root canal. This can occur due to excessive force, inadequate instrumentation technique, or the presence of challenging anatomical features within the root canal. Broken files can present a significant challenge, as they may impede the ability to properly clean and disinfect the canal, potentially leading to complications like infection, treatment failure, or the need for retreatment.
The management of broken files in endodontic procedures typically involves several key steps:
1. Detection and Assessment: Identifying the broken file is the first step, often through radiographs or clinical examination. Assessing the position, size, and location of the broken piece within the canal is essential for planning the appropriate course of action.
2. Decision Making: Depending on the situation, the dentist may decide whether to attempt removal of the broken file or leave it in place. Factors such as the file’s location, the ability to clean and seal the canal around the fragment, and the risk of further complications are considered.
3. Removal Techniques: In cases where removal is necessary, specialized techniques and instruments like ultrasonic devices, hand or rotary files, or retrieval systems are used to remove the broken fragment. This process requires great care to avoid damaging the canal walls or further complicating the treatment.
4. Alternative Approaches: If removal of the file is not feasible or poses a significant risk to the tooth, the dentist may opt for alternative methods, such as bypassing the fragment (using smaller files around the broken piece) or leaving it in place and proceeding with treatment around it.
5. Prevention: To avoid the occurrence of broken files, it’s important to use proper instrumentation techniques, select the right size and type of file, and ensure the canal is adequately irrigated during treatment. Regular training and experience play an important role in preventing such complications.
In summary, managing a broken file in endodontic treatment requires careful planning, skillful technique, and the use of specialized tools to either retrieve or bypass the fragment, ensuring that the root canal system can be properly cleaned, shaped, and sealed for long-term success.

Fig. 1
A systemically healthy 30-year-old female patient was referred to an endodontist complaining of pain in her mandibel right first molar while chewing. Clinical examination revealed that the tooth was sensitive to percussion and palpation, and had no mobility. The probing depth was within the normal range.
X-ray examination was done and on radiographic examination broken file occurs at distal canal apically and middle third of mesiolingual canal of tooth No.46 .

Fig. 2
Access preparation was done with high speed round bur and modified
using EX24 bur. The broken file at MB canal removed with ultrasonic tip E-62 …File. No. 10-Dfinder file was inserted in D canal and bypassed the broken file .

Fig. 3
Final obturation with 3D and BC sealer after full instrumentation with 25.04 rotary files for all canals

Fig. 4
One-year follow-up
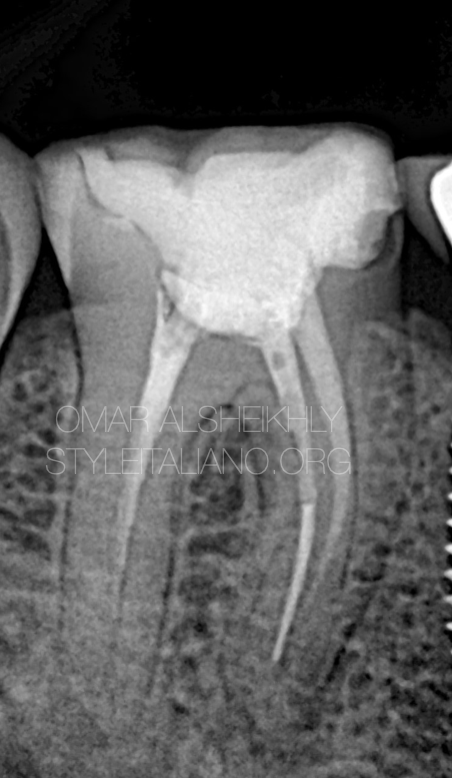
Fig. 5
A 60-year-old female patient with a noncontributory medical history reported to the endodontic with a chief complaint of pain in the lower left mandibular first molar (tooth #46) following a separated rotary file. The pain was mild in intensity, intermittent in nature, aggravated on chewing food, and was relieved on taking medication. The patient gave a past dental history of attempted root canal treatment at a private dental clinic 6 months back and has had pain since then.
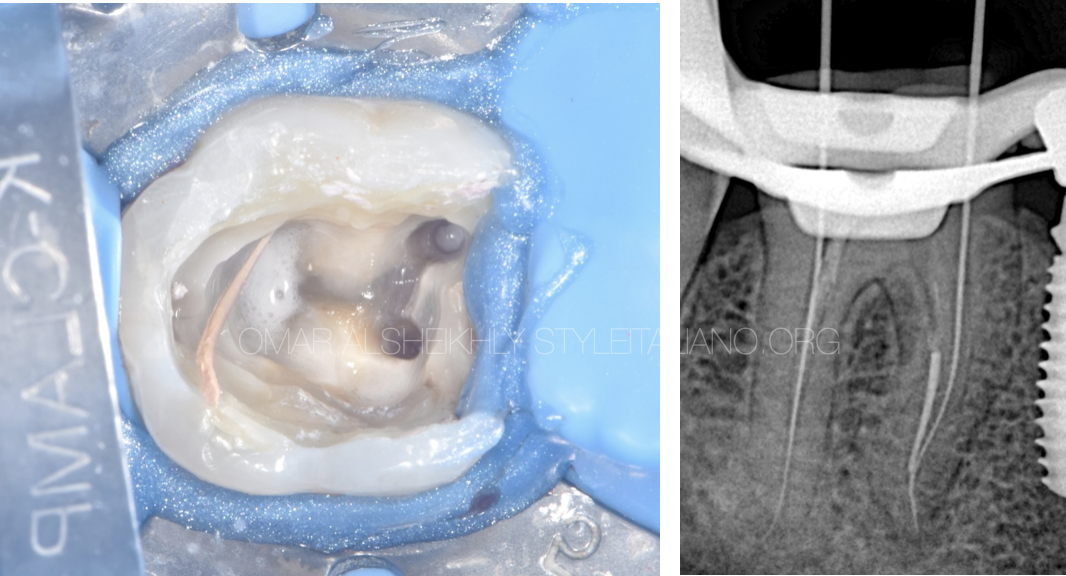
Fig. 6
After removing all the old GP with re-root rotary files Full working length was taken , D-finder No10 and leave the broken file ..
Leaving a broken file in a root canal might be acceptable if removing it poses greater risks or compromises tooth integrity. MB and ML fused it mean have only one apical foramen

Fig. 7
Cone-fit
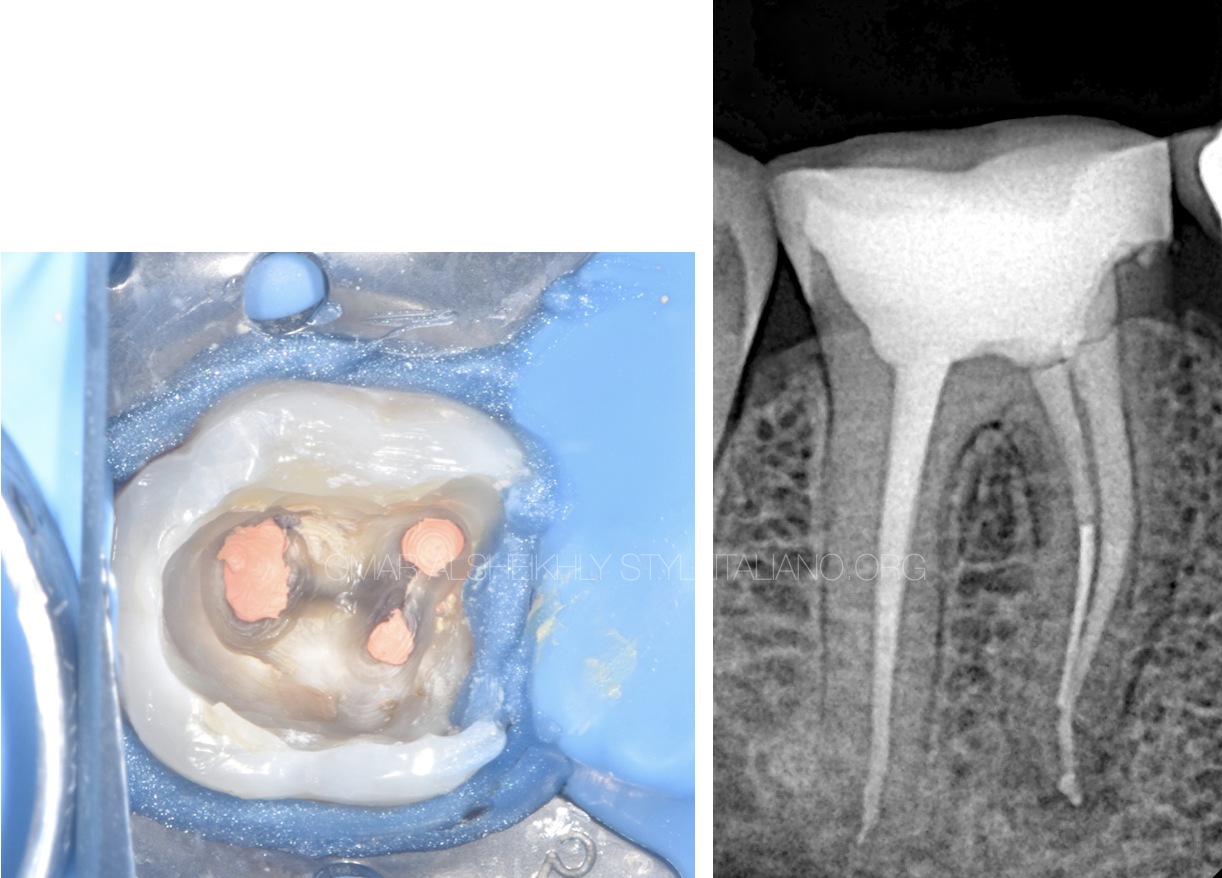
Fig. 8
Post-op x-ray ..obturation with BC sealer with coronal restoration

Fig. 9
6-months follow-up

Fig. 10
About the author:
Dr Omar Alsheikhly
Bachelor of dental surgery (BDS) Ivan Horbachevsky Ternopil State Medical University UKRAIN 2011-2016
Awarded the certificate of equivalency for the diploma Faculty of Dentistry \University of Baghdad IRAQ 2019
MSc master in advanced Endodontics University of Siena \ ITALY 2021\2023
SIE FELLOW MEMBER
Conclusions
In the present case series, an alternate technique for instrument retrieval was successfully performed using a simple and cost-effective, customized chairside syringe and loop technique. This modified approach can be considered an alternative for general dental practitioners and endodontists who do not have access to instrument retrieval systems in their daily clinical practice.
The management of broken files in endodontics requires both a comprehensive understanding of the underlying causes and the development of appropriate strategies to mitigate complications. While non-surgical methods are often effective, in some cases, surgical intervention may be necessary. By following preventive guidelines and adopting the latest advancements in technology and materials, endodontists can reduce the risk of broken files and provide the best possible care for their patients.
Bibliography
1.Shenoy A., Mandava P., Bolla N., Vemuri S. A novel technique for removal of broken instrument from root canal in mandibular second molar. Indian Journal of Dental Research. 2014;25(1):107–110. doi: 10.4103/0970-9290.131157. [DOI] [PubMed] [Google Scholar]
2.Cohen S., Hargreaves K. Pathway’s of the Pulp. 11th. Kansas, MO, USA: Elsevier; 2016. [Google Scholar]
3.Lambrianidis T. Management of Fractured Endodontic Instruments. Cham, Switzerland: Springer; 2018. [Google Scholar]
4.McGuigan M. B., Louca C., Duncan H. F. Clinical decision-making after endodontic instrument fracture. British Dental Journal. 2013;214(8):395–400. doi: 10.1038/sj.bdj.2013.379. [DOI] [PubMed] [Google Scholar]
5.Gluskin A. H., Ruddle C. J., Zinman E. J. Thermal injury through intraradicular heat transfer using ultrasonic devices: precautions and practical preventive strategies. The Journal of the American Dental Association. 2005;136(9):1286–1293. doi: 10.14219/jada.archive.2005.0346.



