Last check of the working length
05/08/2020
Calogero Bugea
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
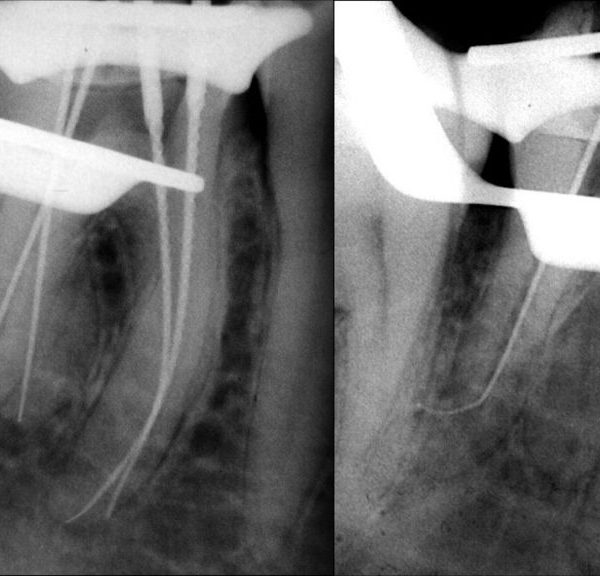
Working lenght (WL) is a controversial topic in Endodontics but, fortunately, Clinicians and Authors agree about respecting it as much is possible during the entire endodontic treatment. WL is the distance from a coronal reference point to the point at which canal preparation and filling should terminate. The respect of an accurate WL determination during the therapy may prevent over-instrumentation and, as immediate consequences, intra-operative bleeding, foramen transportation, overfilling, flare-ups. WL is typically measured with a small k file or with small rotary instruments. WL changes continuously, especially in curved canals, because instrumentation shortens the canal. For this reason a continous check is necessary.
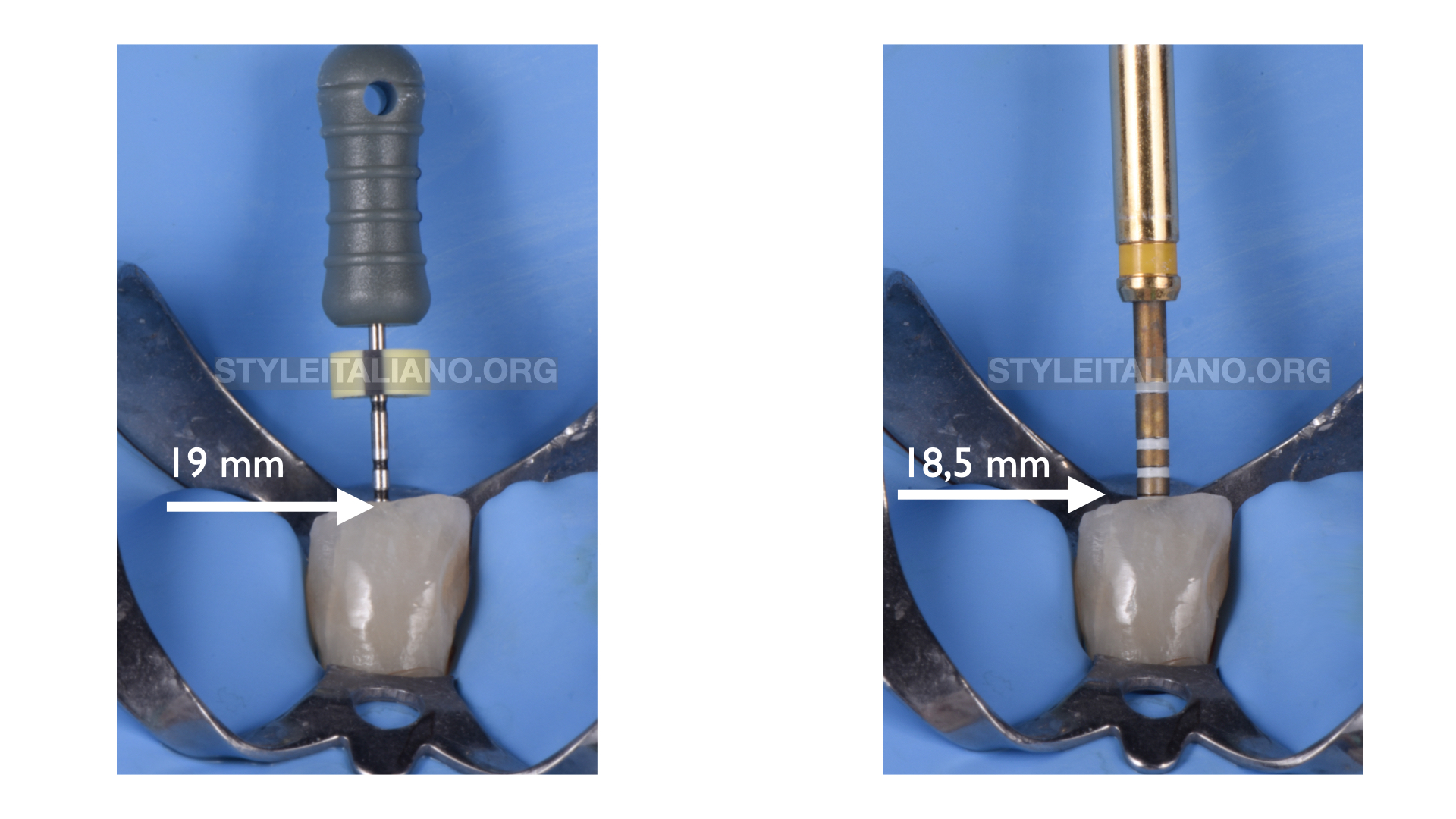
Fig. 1
Canal straightening
During the therapy, especially in case of curved canals, shaping causes the straigthening of the canal. In the picture you can note that the first WL determination was 19 mm, but during the procedure it was double checked in order to avoid over-instrumentation: in fact, it was 18.5 mm.
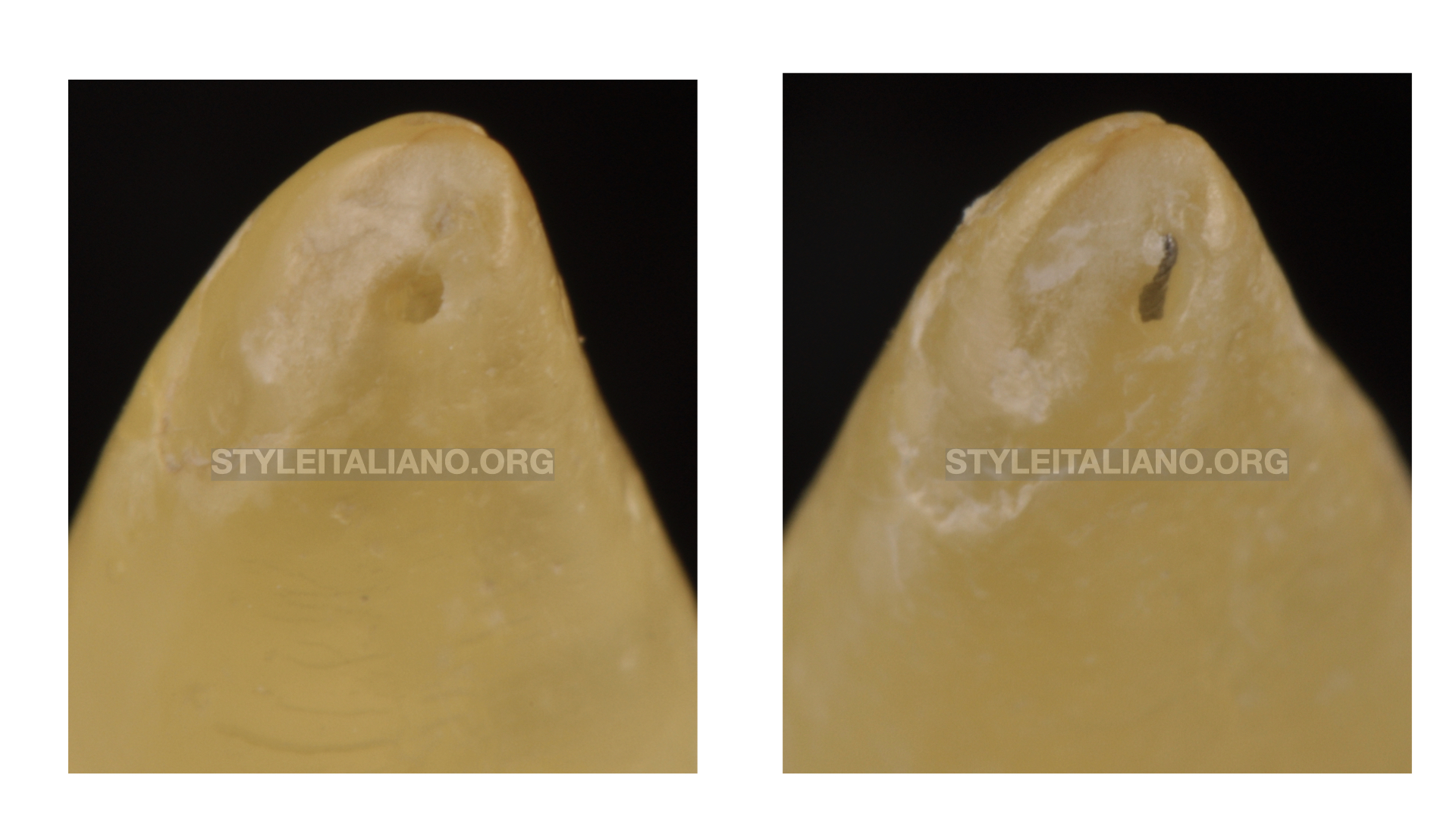
Fig. 2
An overinstrumentation during the therapy can lead foramen transportation, and as immediate consequence poor obturation with lack of seal.
For this reason is very important a continous control of the working lenght.

Fig. 3
Apex locator is more reliable when the instrument inside the canal is approximately the same diameter of the apex
In the picture the apex is 35. The NiTi kfile keep in contact better with the apex walls than k file 10. For this reason usually we overstimate the correct working lengh.

Fig. 4
During the drying procedure, sometimes few drops of blood or exudate can moist the tip of the paper point.
In this cases the first question that the operator should ask himself is: "did I do a proper shaping and irrigation or there is some pulp tissue left"?
In case of doubt, the shaping must be corrected in order to retrieve the residual pulp tissue and a proper irrigation should follow.
On the other hand, if shaping and irrigation are correct, blood or exudate on the paper point tip mean that the paper point goes through the foramen, in the periodontal tissue.

Fig. 5
Tip: the exact working length is the tract between the coronal reference point and and the dried area. If you put a larger point or you cut with scissors the tip of the point, the canal is dry, ready for obturation
The video show clinically what happens during the procedure.
Now the real working length has been determined.

Fig. 6
Another important thing, is that during canal shaping one's reference points rely on silicone stops and inclined plans. For this reasons one last check of the WL before filling is really useful.
Conclusions
Paper points can help the endodontist to confirm or rec-heck the working length.
The performance of this technique is similar to current clinically acceptable standards of estimating the working lenght
Bibliography
Jose Luis Marcos-Arenal , Eric M Rivera, Daniel J Caplan, Martin Trope Evaluating the paper point technique for locating the apical foramen after canal preparation Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009 Nov;108(5):e101-5.
Ricucci D, Langeland K. Apical limit of root canal instrumentation and obturation, part 2. A histological study. Int Endod J. 1998 Nov;31(6):394-409.
Rosenberg DB. The paper point technique, Part 1. Dent Today2003;22:80-6.
Rosenberg DB. The paper point technique, Part 2. Dent Today 2003;22:62-7.